Chemistry Problem Solving Drill
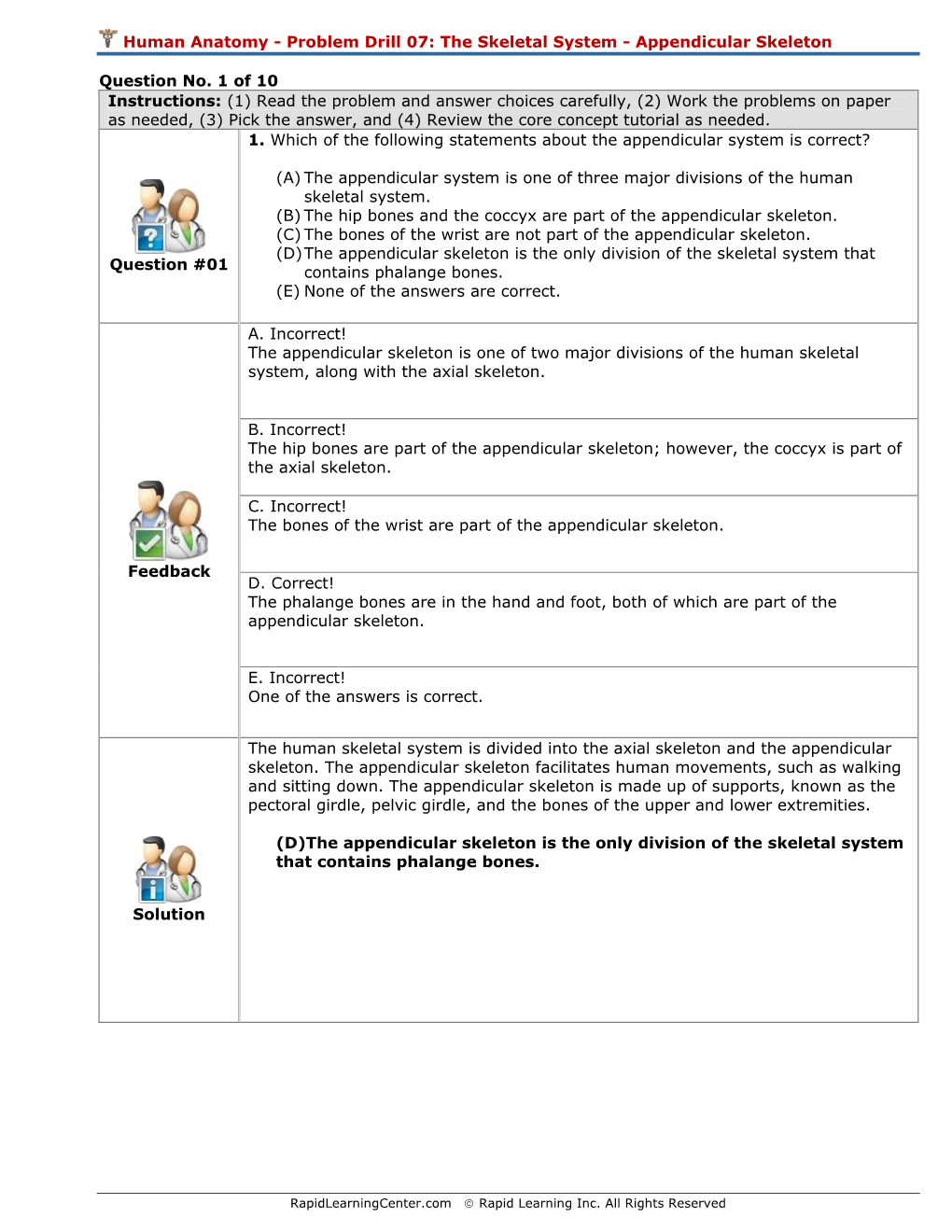
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skeletal Foot Structure
Foot Skeletal Structure The disarticulated bones of the left foot, from above (The talus and calcaneus remain articulated) 1 Calcaneus 2 Talus 3 Navicular 4 Medial cuneiform 5 Intermediate cuneiform 6 Lateral cuneiform 7 Cuboid 8 First metatarsal 9 Second metatarsal 10 Third metatarsal 11 Fourth metatarsal 12 Fifth metatarsal 13 Proximal phalanx of great toe 14 Distal phalanx of great toe 15 Proximal phalanx of second toe 16 Middle phalanx of second toe 17 Distal phalanx of second toe Bones of the tarsus, the back part of the foot Talus Calcaneus Navicular bone Cuboid bone Medial, intermediate and lateral cuneiform bones Bones of the metatarsus, the forepart of the foot First to fifth metatarsal bones (numbered from the medial side) Bones of the toes or digits Phalanges -- a proximal and a distal phalanx for the great toe; proximal, middle and distal phalanges for the second to fifth toes Sesamoid bones Two always present in the tendons of flexor hallucis brevis Origin and meaning of some terms associated with the foot Tibia: Latin for a flute or pipe; the shin bone has a fanciful resemblance to this wind instrument. Fibula: Latin for a pin or skewer; the long thin bone of the leg. Adjective fibular or peroneal, which is from the Greek for pin. Tarsus: Greek for a wicker frame; the basic framework for the back of the foot. Metatarsus: Greek for beyond the tarsus; the forepart of the foot. Talus (astragalus): Latin (Greek) for one of a set of dice; viewed from above the main part of the talus has a rather square appearance. -

Fractures of the Anterior Process of the Calcaneum; a Review and Proposed Treatment Algorithm
Foot and Ankle Surgery 25 (2019) 258–263 Contents lists available at ScienceDirect Foot and Ankle Surgery journal homepage: www.elsevier.com/locate/fas Review Fractures of the anterior process of the calcaneum; a review and proposed treatment algorithm a, b b b b Baljinder S. Dhinsa *, Ahmed Latif , Roland Walker , Ali Abbasian , Diane Back , b Sam Singh a William Harvey Hospital, Kennington Road, Willesborough, Ashford TN24 0LZ, United Kingdom b Guy’s and St Thomas’ NHS Foundation Trust, Great Maze Pond, London SE1 9RT, United Kingdom A R T I C L E I N F O A B S T R A C T Article history: Background: There remains a lack of recognition of these fractures, which leads to a delay in diagnosis and Received 18 June 2017 appropriate management. Received in revised form 1 February 2018 Methods: A comprehensive literature search was performed. Following inclusion and exclusion criteria, Accepted 3 February 2018 23 studies were available for analysis. Results: Delay in diagnosis is common and has a negative impact on outcome. If an APC fracture is Keywords: suspected; anteroposterior, lateral and oblique plain radiographs should be requested. Further Fracture investigation with computed tomography or magnetic resonance imaging is indicated if plain Calcaneum radiographs are inconclusive and patient remains symptomatic. Non-operative measures are usually Anterior process Avulsion adequate for most undisplaced fractures, however surgical intervention maybe required for large, intra- Compression articular fractures in the acute setting and for non-union. Calcaneocuboid Conclusions: A treatment algorithm is suggested that may help with the diagnosis and management of these injuries. -

Morphological and Biomechanical Implications of Cuboid Facet of the Navicular Bone in the Gait
Int. J. Morphol., 37(4):1397-1403, 2019. Morphological and Biomechanical Implications of Cuboid Facet of the Navicular Bone in the Gait Implicaciones Morfológicas y Biomecánicas de la Faceta Cuboídea del Navicular en la Marcha Eduardo Saldías1; Assumpció Malgosa1; Xavier Jordana1 & Albert Isidro2 SALDÍAS, E.; MALGOSA, A.; JORDANA, X. & ISIDRO, A. Morphological and biomechanical implications of cuboid facet of the navicular bone in the gait. Int. J. Morphol., 37(4):1397-1403, 2019. SUMMARY: The cuboid facet of the navicular bone is an irregular flat surface, present in non-human primates and some human ancestors. In modern humans, it is not always present and it is described as an “occasional finding”. To date, there is not enough data about its incidence in ancient and contemporary populations, nor a biomechanical explanation about its presence or absence. The aim of the study was to evaluate the presence of the cuboid facet in ancient and recent populations, its relationship with the dimensions of the midtarsal bones and its role in the biomechanics of the gait. 354 pairs of naviculars and other tarsal bones from historical and contemporary populations from Catalonia, Spain, have been studied. We used nine measurements applied to the talus, navicular, and cuboid to check its relationship with facet presence. To analyze biomechanical parameters of the facet, X-ray cinematography was used in living patients. The results showed that about 50 % of individuals developed this surface without differences about sex or series. We also observed larger sagittal lengths of the talar facet (LSAGTAL) in navicular bones with cuboid facet. No significant differences were found in the bones contact during any of the phases of the gait. -
Bones of the Upper and Lower Limb
Bones of the Upper and Lower limb Musculoskeletal block- Anatomy-lecture 1 Editing file Objectives Color guide : important in Red ✓ Classify the bones of the three regions of the lower Doctor note in Green limb (thigh, leg and foot). Extra information in Grey ✓ Memorize the main features of the – Bones of the thigh (femur & patella) – Bones of the leg (tibia & Fibula) – Bones of the foot (tarsals, metatarsals and phalanges) ✓ Recognize the side of the bone. Note: this lecture is based on female slides since Prof abuel makarem said only things that are mentioned in the female slides will come in the exam Note : All bones picture which are described in this lecture are bones on the right side of the body Before start :Please make yourself familiar with these terms to better understand the lecture Terms Meaning Example Ridge The long and narrow upper edge, angle, or crest The supracondylar ridges (in the distal part of of something (the humerus The trochlear notch (in the proximal part of the Notch An indentation, (incision) on an edge or surface (ulna A nodule or a small rounded projection on the Tubercles (Dorsal tubercle (in the distal part of the radius bone A hollow place (The Notch is not complete but the Subscapular fossa (in the concave part of the Fossa fossa is complete and both of them act as the lock (scapula (of the joint A large prominence on a bone usually serving for Deltoid tuberosity (in the humorous) and it Tuberosity the attachment of muscles or ligaments (is a connects the deltoid muscle (bigger projection than the Tubercle -

PTA019: Anatomy & Physiology Manual
Anatomy & Physiology Full content for both the Level 2 Certificate in Fitness Instructing & Level 3 Certificate in Personal Training LEARN - INSPIRE - SUCCEED Contents Anatomy & Physiology for Exercise ………………………………………. Page 3 • The Musculoskeletal System ………………………………………. Page 3 • Energy Systems ………………………………………. Page 76 • The Cardiorespiratory System ………………………………………. Page 86 • The Neuroendocrine System ………………………………………. Page 105 Performance Training Academy 2 Chapter Two: Anatomy and Physiology Introduction This chapter is to be broken down into many sub-chapters, giving you a great reference point for your study as well as when needed once you are actively working as a Fitness Professional. It is of upmost importance that you continue to recap and learn further about the bio-mechanics and workings of the human body. A great fitness professional won’t just know how to programme for an individual, but will know how to help improve weaknesses and imbalances within the body, knowledge of Anatomy and Physiology is key to be able to do this. The Musculoskeletal System Unit Objectives Our first objective is to understand the biomechanics of the human body. We can do this by learning about the skeletal system, and then how the muscles are layered upon the skeleton. By the end of this unit we want you to have a good subject knowledge of the following: • The main bones of the skeleton • Joint types and joint actions • How exercise can create a strong and healthy skeletal system • The main muscles of the body • Muscle contractions and fibre types We will start by going through the skeletal system before bringing the muscles into the equation. This will allow you to build up your knowledge of bones and terminology before recapping them again by layering the muscles across specific joints. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Osteoid Osteoma of the Trapezoid Bone
'-DIDUL)1DMG0D]KDU Case Report Osteoid Osteoma of the Trapezoid Bone Dawood Jafari MD1)DULG1DMG0D]KDU0'1 Abstract Osteoid osteoma is a benign, bone-forming tumor that rarely involves the carpal bones. We report a case of osteoid osteoma of the trap- H]RLGFDUSDOERQHZLWKH[WHQVLRQWRWKHDGMDFHQWVHFRQGPHWDFDUSDOERQH&KURQLFZULVWSDLQDQGORFDOWHQGHUQHVVZHUHWKHPDMRUFOLQLFDO signs and symptoms. In chronic wrist pain osteoid osteoma and the possibility of extension to the adjacent bones should be considered. Keywords: &DUSDOERQHPHWDFDUSDORVWHRLGRVWHRPDWUDSH]RLG Cite the article as: Jafari D, Najd Mazhar F. Osteoid Osteoma of the Trapezoid Bone. Arch Iran Med. 2012; 15(12): 777 – 779. Introduction RSV\WKURXJKDGRUVDODSSURDFK:HXVHGDVPDOOGULOOELWDQG¿QH osteotome to remove the involved area, which included the adjacent steoid osteoma is a benign bone tumor that rarely localizes articular surface of the trapezoid. The biopsy specimen had a highly to the carpal bones.1,2 Wrist pain usually is the main com- vascular reddish nidus embedded in normal bone (Figure 5). We no- O plaint and because it rarely involves the carpal bone, diag- ticed that the articular surface of the second metacarpal was eroded nosis is often delayed. It has been reported in the scaphoid and lu- and softened (Figure 6). Following curettage, we sent the specimen nate areas; however, the trapezoid is an exceedingly rare location from the base of the second metacarpal in a separate container for for osteoid osteoma. Bifocal involvement of adjacent carpal bones pathologic analysis. The results of the histologic examinations of has been reported previously but to the best of our knowledge ex- both biopsy specimens indicated osteoid osteoma (Figure 7). Since tension of osteoid osteoma through the joint to adjacent bone has we had only one nidus at the CT scan and involvement of both trap- not been mentioned in the literature. -

Osteoblastoma of the Trapezoid Bone and Triquetral Bone: Report of Two Cases
CASE REPORT Acta Orthop Traumatol Turc 2013;47(5):376-378 doi:10.3944/AOTT.2013.3081 Osteoblastoma of the trapezoid bone and triquetral bone: report of two cases ‹brahim KAYA1, Burak BOYNUK2, Caner GÜNERBÜYÜK3, Ak›n U⁄RAfi4 1Department of Orthopedics and Traumatology, Haseki Training and Research Hospital, ‹stanbul, Turkey; 2Department of Orthopedics and Traumatology, Bak›rköy Ac›badem Hospital, ‹stanbul, Turkey; 3Department of Orthopedics and Traumatology, 29 May›s Hospital, ‹stanbul, Turkey; 4Department of Orthopedics and Traumatology, ‹stanbul Medipol University, School of Medicine, ‹stanbul, Turkey Osteoblastoma is a benign local aggressive tumor mostly localized in the vertebra or long bones. Carpal location and recurrence are extremely rare. Treatment options include either curettage or wide en bloc resection which causes functional disability in the hand and wrist and should be reserved only for recurrence. We present a case of recurrent trapezoid osteoblastoma previously treated with curet- tage of the trapezoid bone and a case of primary triquetral osteoblastoma. Key words: Curettage; osteoblastoma; trapezoid bone; triquetral bone. Osteoblastoma is a benign primary bone tumor first pain increased at night and had a good response to non- described as “giant osteoid osteoma” by Dahlin and steroidal analgesic drugs. Radiographs, computerized Johnson in 1954.[1] Later, in 1956, Lichtenstein and Jaffe tomography and magnetic resonance imaging (MRI) named this tumor “osteoblastoma” in two different arti- revealed findings resembling avascular necrosis of the cles.[2] It is an uncommon benign but locally aggressive trapezoid bone, periosteal reaction at the second tumor, most commonly located in the vertebral column metacarpal and generalized edema in the dorsal com- or metaphysis of long bones. -

Carpal Fractures
CURRENT CONCEPTS Carpal Fractures Nina Suh, MD, Eugene T. Ek, MBBS, PhD, Scott W. Wolfe, MD CME INFORMATION AND DISCLOSURES The Review Section of JHS will contain at least 3 clinically relevant articles selected by the Provider Information can be found at http://www.assh.org/Pages/ContactUs.aspx. editor to be offered for CME in each issue. For CME credit, the participant must read the Technical Requirements for the Online Examination can be found at http://jhandsurg. articles in print or online and correctly answer all related questions through an online org/cme/home. examination. The questions on the test are designed to make the reader think and will occasionally require the reader to go back and scrutinize the article for details. Privacy Policy can be found at http://www.assh.org/pages/ASSHPrivacyPolicy.aspx. The JHS CME Activity fee of $30.00 includes the exam questions/answers only and does not ASSH Disclosure Policy: As a provider accredited by the ACCME, the ASSH must ensure fi include access to the JHS articles referenced. balance, independence, objectivity, and scienti c rigor in all its activities. Disclosures for this Article Statement of Need: This CME activity was developed by the JHS review section editors and review article authors as a convenient education tool to help increase or affirm Editors reader’s knowledge. The overall goal of the activity is for participants to evaluate the Ghazi M. Rayan, MD, has no relevant conflicts of interest to disclose. appropriateness of clinical data and apply it to their practice and the provision of patient Authors care. -

Geometric Variations in Load-Bearing Joints
University of Alberta Geometric Variations in Load-Bearing Joints by Kamrul Islam A thesis submitted to the Faculty of Graduate Studies and Research in partial fulfillment of the requirements for the degree of Master of Science in Structural Engineering Department of Civil and Environmental Engineering ©Kamrul Islam Fall 2012 Edmonton, Alberta Permission is hereby granted to the University of Alberta Libraries to reproduce single copies of this thesis and to lend or sell such copies for private, scholarly or scientific research purposes only. Where the thesis is converted to, or otherwise made available in digital form, the University of Alberta will advise potential users of the thesis of these terms. The author reserves all other publication and other rights in association with the copyright in the thesis and, except as herein before provided, neither the thesis nor any substantial portion thereof may be printed or otherwise reproduced in any material form whatsoever without the author's prior written permission. Dedication Dedicated to my dad, A.F.M. Shamsul Islam, my mom, Shahina Akhter Chowdhury, and my brother, Nazmul Islam Abstract The purpose of the current study was to investigate the geometric variations in the load-bearing joints among individuals. Two existing concepts in mathematics were introduced and their application in computational biomechanics was completely novel: 1) computing the depth of penetration between contact objects as an indirect measure of stress; and 2) computing the geometric similarity using the cubic root of volumetric ratio as a scaling law. Furthermore, an alternative geometric method to finite element analysis was proposed, which should be considered as a “proof of concept”. -

Masaryk University Faculty of Medicine REHABILITATION IN
Masaryk University Faculty of Medicine REHABILITATION IN PATIENTS AFTER TOTAL KNEE ARTHROPLASTY Bachelor´s Thesis Physiotherapy Bachelor’s Thesis Supervisor: Author: Mgr. Veronika Mrkvicová Josh Tilrem Brno, 2018 Name and Surname of the Author: Josh Tilrem Title of Bachelor’s thesis: Rehabilitation in patients after total knee arthroplasty Název bakalářské práce: Rehabilitace u pacientů po totální endoprotéze kolenního kloubu Department: Department of Rehabilitation and Physiotherapy MF MU Supervisor: Mgr. Veronika Mrkvicová Year of the Bachelor’s thesis defence: 2018 Summary: This Bachelor’s thesis is composed of two parts. The first part deals with the subject of total knee arthroplasty. The aim of this part is to describe the indication, surgical procedure and treatment, both in acute and long-term phase. The first part also contains the approach and management of the physical therapist and how to utilize proper rehabilitation. The second part is a case study and the aim is to describe the practical procedure of a specific rehabilitation after total knee arthroplasty. This include examination at admittance, discharge and rehabilitation provided by the author. Souhrn: Tato bakalářská práce je složená ze dvou částí. Prní část pojednává o tématu totální endoprotézy kolenního kloubu. Cílem této části je popsat indikace, chirurgický přístup a léčbu, jak v akutní, tak chronické fázi. První část také zahrnuje fyzioterapetické postupy a provádění léčebné rehabilitace. Druhá část obsahuje kazuistiku a jejím cílem je přiblížit praktické postupy speciální rehabilitace po totální endoprotéze kolenního kloubu. To zahrnuje vstupní a výstupní vyšetření a rehabilitaci prováděnou autorem. Keywords: Total knee arthroplasty, rehabilitation, physiotherapy Klíčová slova: Totální endoprotéza kolenního kloubu, rehabilitace, fyzioterapie I agree that this bachelor thesis will be archived in the Masaryk University of Brno library and will be quoted according to citations norms. -

The Structure and Movement of Clarinet Playing D.M.A
The Structure and Movement of Clarinet Playing D.M.A. DOCUMENT Presented in Partial Fulfilment of the Requirements for the Degree Doctor of Musical Arts in the Graduate School of The Ohio State University By Sheri Lynn Rolf, M.D. Graduate Program in Music The Ohio State University 2018 D.M.A. Document Committee: Dr. Caroline A. Hartig, Chair Dr. David Hedgecoth Professor Katherine Borst Jones Dr. Scott McCoy Copyrighted by Sheri Lynn Rolf, M.D. 2018 Abstract The clarinet is a complex instrument that blends wood, metal, and air to create some of the world’s most beautiful sounds. Its most intricate component, however, is the human who is playing it. While the clarinet has 24 tone holes and 17 or 18 keys, the human body has 205 bones, around 700 muscles, and nearly 45 miles of nerves. A seemingly endless number of exercises and etudes are available to improve technique, but almost no one comments on how to best use the body in order to utilize these studies to maximum effect while preventing injury. The purpose of this study is to elucidate the interactions of the clarinet with the body of the person playing it. Emphasis will be placed upon the musculoskeletal system, recognizing that playing the clarinet is an activity that ultimately involves the entire body. Aspects of the skeletal system as they relate to playing the clarinet will be described, beginning with the axial skeleton. The extremities and their musculoskeletal relationships to the clarinet will then be discussed. The muscles responsible for the fine coordinated movements required for successful performance on the clarinet will be described.