Using Nerve Transfer to Restore Prehension and Grasp 12 Years Following Spinal Cord Injury: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -
Brachial Plexus Injury
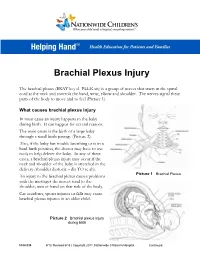
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

Nerve Transfers for Restoration of Finger Flexion in Patients with Tetraplegia
CLINICAL ARTICLE J Neurosurg Spine 26:55–61, 2017 Nerve transfers for restoration of finger flexion in patients with tetraplegia Jayme A. Bertelli, MD, PhD,1,2 and Marcos F. Ghizoni, MD, MSc2 1Center of Biological and Health Sciences, Department of Neurosurgery, University of the South of Santa Catarina (Unisul), Tubarão; and 2Department of Orthopedic Surgery, Governador Celso Ramos Hospital, Florianópolis, Santa Catarina, Brazil OBJECTIVE The purpose of this paper was to report the authors’ results with finger flexion restoration by nerve transfer in patients with tetraplegia. METHOds Surgery was performed for restoration of finger flexion in 17 upper limbs of 9 patients (8 male and 1 female) at a mean of 7.6 months (SD 4 months) after cervical spinal cord injury. The patients’ mean age at the time of surgery was 28 years (SD 15 years). The motor level according to the ASIA (American Spinal Injury Association) classification was C-5 in 4 upper limbs, C-6 in 10, and C-7 in 3. In 3 upper limbs, the nerve to the brachialis was transferred to the anterior interosseous nerve (AIN), which was sepa- rated from the median nerve from the antecubital fossa to the midarm. In 5 upper limbs, the nerve to the brachialis was transferred to median nerve motor fascicles innervating finger flexion muscles in the midarm. In 4 upper limbs, the nerve to the brachioradialis was transferred to the AIN. In the remaining 5 upper limbs, the nerve to the extensor carpi radialis brevis (ECRB) was transferred to the AIN. Patients were followed for an average of 16 months (SD 6 months). -

Bilateral Brachial Plexus Injury Fahim Anwar, Danny Mclaughlin and Bhupinder S
CASE REPORT Bilateral Brachial Plexus Injury Fahim Anwar, Danny McLaughlin and Bhupinder S. Panesar ABSTRACT Brachial plexus injuries can occur as a result of various mechanisms such as stretching, direct and indirect trauma or following childbirth. Bilateral brachial plexus injuries are uncommon and associated with a poor functional outcome. We report a case of bilateral brachial plexus injury resulting from prolonged immobilization of the arms in hyper-abducted position resulting in compression of the brachial plexus on both sides. The injuries were treated conservatively and following 4 months of active rehabilitation in our unit, the patient still had poor arm functions and required care and support in the community on discharge. Key words: Bilateral. Brachial plexus. Injury. Rehabilitation. INTRODUCTION Table I: Summary of neurological findings. Brachial plexus is a network of nerves originating from Medical research council grading of muscle power fifth to seventh cervical (C5-C7) and the first two At admission Following rehabilitation thoracic (T1-T2) spinal nerves. These networks of Right Left Right Left nerves innervate the muscles and skin of the chest, Shoulder abduction 2 1 4 3 Shoulder flexion 0 0 4 3 shoulder, arm and hand. Damage to these nerves Elbow flexion 0 0 0 0 lead to symptoms ranging from a completely paralyzed Elbow extension 0 0 0 0 upper limb to a lack of muscle control in the arm, Wrist flexion 0 0 3 2 wrist or hand and diminished sensations. Injury to the Wrist extension 0 0 0 0 brachial plexus could be the result of trauma to the Finger flexion 1 0 3 2 1 shoulder, traction injury to the spine, inflammation or Finger extension 0 0 0 0 tumour. -
Brachial Plexus Injury Reversing Paralysis & Restoring Function
The Paralysis Center PATIENT GUIDE Brachial Plexus Injury Reversing Paralysis & Restoring Function Justin M. Brown, M.D. Contents 1. Introduction 2. The Anatomy of a Damaged Nerve 3. Assessing Nerve Damage 4. Understanding Brachial Plexus Anatomy 5. Diagnosing Brachial Plexus Injuries - Nerve Conduction & Diagnostic Studies - Diagnostic Testing 6. Understanding Your Treatment Options - Reconstructive Neurosurgery ● Nerve Grafting ● Tendon Transfer ● Muscle Transplant ● Nerve Transfer 7. Why Nerve Transfers are so Successful in Reversing Many Forms of Paralysis - Nerve Transfer as MVP (Most Valuable Player) 8. Post Operative Rehabilitation - Physical and Occupational Therapy 9. But What About …? - Stem Cell Therapy - Robotic Arm 10. Brachial Plexus Patient Stories - Meet Kyle - Meet Diana and Josh 11. Are You a Candidate for Nerve Reconstruction? 12. Tips to Help You Prepare for Your Initial Consult 13. Conclusion 14. About Dr. Brown 15. Contact The Paralysis Center 1 1. Introduction If you are a patient who has suffered injury to your brachial plexus, we are battling against time. Please do not wait to see what kind of function may or may not return following your injury, no matter what you may have been told. More than any other nerve injury, repairing a brachial plexus injury is the most complex and the most time-sensitive of any peripheral nerve injury. We have the greatest chance of restoring maximum function to your arm and hand the faster you can be seen by a Brachial Plexus Specialist - ideally within the first six months following your injury. If this is you, please book a consult immediately with a Brachial Plexus specialist. In 2017, in partnership with Massachusetts General Hospital, Harvard Medical School, and the Spaulding Rehabilitation Hospital, we founded the Paralysis Center - a world-class patient treatment and medical research center for all forms of paralysis. -

Repairing Spinal Roots After Brachial Plexus Injuries
Paraplegia (I 995)n. 359-361 © 1995 International Medical Society of Paraplegia All rights reserved 0031.1758/95$12.00 Repairing spinal roots after brachial plexus injuries MA Glasby! and TEl Hems2 1 Department of Anatomy, University of Edinburgh Medical School, Teviot Place, Edinburgh EH8 9AG; 2Nuffield Orthopaedic Centre, Headington, Oxford, UK The problems of repairing spinal roots after brachial plexus avulsion injuries are discussed in the light of current surgical diagnosis and treatment. An advancing understanding of the cellular mechanisms of nerve regeneration and progress in surgical technology indicates a possibility for the repair at least of ventral roots with grafts which may be of neural or non-neural origin. Enhancement of the regenerative properties may further be made possible by the application of neurotrophic factors at the repair site or centrally. The short and long-term implications of current research into these methods are discussed. Keywords: spinal root repair; nerve regeneration; ventral root implantation; neurotrophic factors The present rarely regained in adults but appears to have a slightly better prognosis in young children.4,5 Over 350 patients suffer severe damage from closed traction injuries of the brachial plexus each year in the United Kingdom.1 Many of these are young adults involved in motorcycle accidents.2 Over recent years, The future surgical exploration has been increasingly recom mended if the mechanism of injury suggests that a The typical traction injury sustained by any spinal root major disruption is likely and if examination reveals a consists of rupture of all neural elements whilst the complete absence of function of all or any part of the integrity of the fibrous epineurium is maintained plexus.1,3-5 Operation should be carried out as soon as (Sunderland type IV).9 Repair is by excision of the possible after injury. -

American College of Radiology ACR Appropriateness Criteria® Plexopathy
Revised 2021 American College of Radiology ACR Appropriateness Criteria® Plexopathy Variant 1: Brachial plexopathy, acute or chronic, nontraumatic. No known malignancy. Initial imaging. Procedure Appropriateness Category Relative Radiation Level MRI brachial plexus without IV contrast Usually Appropriate O MRI brachial plexus without and with IV Usually Appropriate O contrast MRI cervical spine without and with IV May Be Appropriate O contrast MRI cervical spine without IV contrast May Be Appropriate O May Be Appropriate CT neck with IV contrast ☢☢☢ US neck Usually Not Appropriate O MRI brachial plexus with IV contrast Usually Not Appropriate O MRI cervical spine with IV contrast Usually Not Appropriate O Usually Not Appropriate CT cervical spine with IV contrast ☢☢☢ CT cervical spine without and with IV Usually Not Appropriate contrast ☢☢☢ Usually Not Appropriate CT cervical spine without IV contrast ☢☢☢ Usually Not Appropriate CT neck without and with IV contrast ☢☢☢ Usually Not Appropriate CT neck without IV contrast ☢☢☢ Usually Not Appropriate CT myelography cervical spine ☢☢☢☢ Usually Not Appropriate FDG-PET/CT whole body ☢☢☢☢ ACR Appropriateness Criteria® 1 Plexopathy Variant 2: Lumbosacral plexopathy, acute or chronic, nontraumatic. No known malignancy. Initial imaging. Procedure Appropriateness Category Relative Radiation Level MRI lumbosacral plexus without and with IV Usually Appropriate O contrast MRI lumbosacral plexus without IV contrast Usually Appropriate O MRI lumbar spine without and with IV May Be Appropriate O contrast -

The International Standards Booklet for Neurological and Functional Classification of Spinal Cord Injury*
Paraplegia 32 (1994) 70-80 © 1994 International Medical Society of Paraplegia The International Standards Booklet for Neurological and Functional Classification of Spinal Cord Injury* 1 F Ditunno lr MD,! W Young PhD MD,2 W H Donovan MD,3 G Creasey MD-+ 1 Department of Rehabilitation Medicine, Thomas Jefferson University Ho pital � : . Philadelphia, Pennsylvania; 2 Department of eurosurgery, New York Umverslty edlcal 3 ."! . � Center, New York; The Institute for RehabdltatlOn and Research, l!0u�ton, Texas, 4Department of Biomedical Engineering, Case Western Reserve University, Cleveland, Ohio, USA. Introduction recognition of the need for greater accept ance, ASIA sought input from a broader For almost a quarter of a century the international community in spinal cord in array of experts representing. SCI res�a.rch jury (SCI) has advocated a unifor measure interests as well as from dIverse chlllcal � specialis s. The international Medical Soci of SCI severity. 1 Such agreement IS needed � ety of Paraplegia (IMSOP), as ell as ma y for the accurate communication between � � other organizations and professIOnal socie clinicians and for comparisons of research ties interested in classification, were repre results among investigators. The severity f ? sented by members on the committee the injury after SCI is primarily reflecte� III the extent of paralysis and loss of sensation formed in 1990. The international standards revised by the ASIA Committee in 1992 (impairment) and the inability to perform activities of daily living (disability). These were endorsed by IMSOP in Barcelona, in measurements of impairment and disability September 1992. The rationale for these standards evolved serve as the determinants of the clinical from two major influences. -

Download the Brachial Plexus Center Brochure
BRACHIAL PLEXUS CENTER DEPARTMENT OF NEUROSURGERY, NEUROLOGY, AND ORTHOPEDIC SURGERY ESTABLISHED IN 1991 EXPERTISE OF THE ST. LOUIS CHILDREN’S BRACHIAL PLEXUS CENTER HOSPITAL • 390 beds • 3,330 employees • 818 medical staff members • 1,300 auxiliary members and volunteers • More than 45 pediatric subspecialty departments and divisions • Level I Pediatric Trauma Center, the highest level of emergency care available Founded in 1879, St. Louis Children’s Left to Right: Tae Sung Park, MD, Nicole Meyer, PA-C, Lindley Wall, MD, Michael Noetzel, MD Hospital is one of the premier • Recognized as one of the best children’s children’s hospitals in the nation. It hospitals in the nation serves not just the children of St. Established in 1991, the Brachial Plexus Center has extensive by U.S. News & Louis, but children across the world. experience in the treatment of birth brachial plexus injury. World Report As the pediatric teaching hospital Our Center has cared for over 1,000 infants with brachial plexus for Washington University School of injury and performed brachial plexus repair procedures on over • Received the nation’s 250 infants. highest honor for Medicine, St. Louis nursing excellence, Children’s Hospital The Center’s team consists of pediatric neurosurgeons, neurologist, the Magnet designation, offers nationally orthopedic surgeon, occupational and physical therapists, from the American recognized neuroradiologist, and clinical coordinator. Nurses Credentialing programs for At the Brachial Plexus Center at St. Louis Children’s Hospital, Center. physician training parents find hope and unparalleled pediatric expertise. and research. 1 2 The Brachial Plexus THE CAUSE OF BIRTH BRACHIAL PLEXUS PALSY The brachial plexus is a complex arrangement of nerves that controls Diagram 3: Shoulder Dystocia the muscles of the shoulder, arms and hands.