Traumatic Brachial Plexus Injury G
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Strategies to Improve Nerve Regeneration After Radical Prostatectomy: a Narrative Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Institutional Research Information System University of Turin Strategies to improve nerve regeneration after radical prostatectomy: a narrative review Stefano Geuna 1, 2, Luisa Muratori1, 2, Federica Fregnan 1, 2, Matteo Manfredi4 , Riccardo Bertolo 3, 4 , Francesco Porpiglia4. 1 Department of Clinical and Biological Sciences, University of Turin, Orbassano (To), 10043, Italy. 2 Neuroscience Institute Cavalieri Ottolenghi (NICO), Orbassano (To), 10043, Italy. 3 Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, US. 4 Department of Oncology, University of Turin, Orbassano (To), 10043, Italy. Abstract Peripheral nerves are complex organs that spread throughout the entire human body. They are frequently affected by lesions not only as a result of trauma but also following radical tumor resection. In fact, despite the advancement in surgical techniques, such as nerve- sparing robot assisted radical prostatectomy, some degree of nerve injury may occur resulting in erectile dysfunction with significant impairment of the quality of life. The aim of this review is to provide an overview on the mechanisms of the regeneration of injured peripheral nerves and to describe the potential strategies to improve the regeneration process and the functional recovery. Yet, the recent advances in bio- engineering strategies to promote nerve regeneration in the urological field are outlined with a view on the possible future regenerative therapies which might ameliorate the functional outcome after radical prostatectomy. 1 Introduction Radical prostatectomy is the gold standard surgical treatment for organ-confined prostate cancer. The employment of innovative surgical technique such as nerve-sparing robot assisted radical prostatectomy allowed to magnify the anatomical field leading to a three- dimensional perspective obtained through the robotic lenses and a better anatomical knowledge. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -

Some Aspects of Facial Nerve Paralysis* PART Li
13 Januarie 1973 S.-A. MEDIESE TVDSKRIF 65 Some Aspects of Facial Nerve Paralysis* PART lI. ELECTRICAL TESTS AND THE SUBMAXILLARY SALlYARY TEST M. G. POTGIETER,t M.B. CH.B. UNIV. PRET., M.MED. OTOL. UNIV. CAPE TOWN, Department of Otolaryngology, Groote Schuur Hospital, Observatory, Cape SUMMARY fibres are the first to be affected and when there is re generation, the new fibres conduct slowly.' The submaxillary salivary flow test gives reliable in The maintenance of nerve and muscle excitability de formation as to whether neurapraxia, axono:mesis, or pends greatly upon sodium and potassium cations. States neurotmesis of the facial nerve is present. This can be of polarization and depolarization are dependent on the corroborated by electrical studies. This test can make an shift of sodium and potassium cations across the cell important contribution to the topognosis and prognosis of membranes. With injury to the nerve;" elimination of facial paralysis, especially when elaborate electrical the membrane potential takes place and this causes a lack equipment for nerve excitability tests and electromyo of electrical conduction. A shift of potassium from the graphy is not available. cell takes place. An over-all increase in the potassium content of the injured nerve exists where, for instance, S. Afr. Med. J., 47, 65 (1973). bone fragments cause a foreign body reaction. Hyaluronic acid from an inflammatory response, occurs as a potas sium hyaluronate. Fibroblast and mast-cell activities in ELECTRlCAL TESTS crease and elaborate mucopolysaccharides. This may explain the high potassium values, maintained in the In 1872 Duchenne described the technique of nerve ex injured area of the nerve, inhibiting transmission. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -

Respiratory Management in the Patient with Spinal Cord Injury
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 168757, 12 pages http://dx.doi.org/10.1155/2013/168757 Review Article Respiratory Management in the Patient with Spinal Cord Injury Rita Galeiras Vázquez,1 Pedro Rascado Sedes,2 Mónica Mourelo Fariña,1 Antonio Montoto Marqués,3,4 and M. Elena Ferreiro Velasco3 1 Critical Care Unit, Complexo Hospitalario Universitario A Coruna,˜ CP. 15006, A Coruna,˜ Spain 2 Critical Care Unit, Complexo Hospitalario Universitario de Santiago de Compostela, CP. 15702, Santiago de Compostela, Spain 3 Spinal Cord Injury Unit, Complexo Hospitalario Universitario A Coruna,˜ CP. 15006, A Coruna,˜ Spain 4 Department of Medicine, University of A Coruna,˜ CP. 15006, A Coruna,˜ Spain Correspondence should be addressed to Rita Galeiras Vazquez;´ [email protected] Received 30 April 2013; Revised 11 July 2013; Accepted 30 July 2013 Academic Editor: Boris Jung Copyright © 2013 Rita Galeiras Vazquez´ et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Spinal cord injuries (SCIs) often lead to impairment of the respiratory system and, consequently, restrictive respiratory changes. Paresis or paralysis of the respiratory muscles can lead to respiratory insufficiency, which is dependent on the level and completeness of the injury. Respiratory complications include hypoventilation, a reduction in surfactant production, mucus plugging, atelectasis, and pneumonia. Vital capacity (VC) is an indicator of overall pulmonary function; patients with severely impaired VC may require assisted ventilation. It is best to proceed with intubation under controlled circumstances rather than waiting until the condition becomes an emergency. -
Nerve Evaluation Protocol 2014
Nerve Evaluation Protocol 2014 TABLE OF CONTENTS INTRODUCTION .................................................................................................... 1 A REVIEW OF SENSORY NERVE INJURY ................................................................ 3 TERMINOLOGY ...................................................................................................... 5 INFORMED CONSENT ............................................................................................ 6 PREOPERATIVE EVALUATION ................................................................................ 7 TESTS FOR SENSORY NERVE FUNCTION: ........................................................... 12 MATERIALS NEEDED FOR TESTING SENSORY PERCEPTION .............................. 17 TESTING TECHNIQUE .......................................................................................... 20 REFERENCES .......................................................................................................... 23 BIBLIOGRAPHY - CORONECTOMY ..................................................................... 28 SAMPLE SENSORY RECORDING SHEETS ............................................................. 30 A HANDOUT FOR PATIENTS ............................................................................... 33 INTRODUCTION The first edition of this document was produced in the Spring of 1988. Dr. A. F. Steunenberg and Dr. M. Anthony Pogrel collaborated to produce the first edition with input from Mr. Art Curley, Esquire, and with Dr. Charles Alling editing -
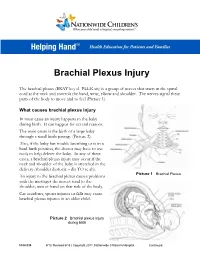
Brachial Plexus Injury
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

Nerve Injury Classifications – Seddon's and Sunderland's
The Pain Source Makes Learning About Pain, Painless http://thepainsource.com Nerve Injury Classifications – Seddon’s and Sunderland’s Author : admin By Chris Faubel, MD -- Understanding nerve injury classification is essential for prognostic value clinically. Some basic anatomy, along with the two classification systems, and their corresponding EMG findings need to be learned and remembered. Two classification systems exist (and are frequently tested in various exams): 1. Seddon's classification (neuropraxia, axonotmesis, neurotmesis) 2. Sunderland's classification (types 1-5) To understand the systems, you must first review some basic nerve anatomy. There are three connective tissue layers in the CNS and PNS. 1. epineurium 2. perineurium 3. endoneurium Individual nerve fibers (single axons) are covered with varying amounts of myelin and then covered by endoneurium. These individually wrapped nerve fibers are then grouped into bundles of fibers called fascicles, which are covered by perineurium. Finally, groups of fascicles are bundled together to form the peripheral nerve (such as the median nerve), which is covered by epineurium. Seddon's classification: Neuropraxia 1 / 3 The Pain Source Makes Learning About Pain, Painless http://thepainsource.com Physical Medicine & Rehabilitation Board Review - Sara Cuccurullo, MD refers to local myelin injury with the axon still intact and functional motor > sensory fibers affected considered a temporary paralysis of the nerve fiber least severe injury usually from crush injury or ischemia Electrodiagnostic -

Peripheral Nerve Regeneration and Muscle Reinnervation
International Journal of Molecular Sciences Review Peripheral Nerve Regeneration and Muscle Reinnervation Tessa Gordon Department of Surgery, University of Toronto, Division of Plastic Reconstructive Surgery, 06.9706 Peter Gilgan Centre for Research and Learning, The Hospital for Sick Children, Toronto, ON M5G 1X8, Canada; [email protected]; Tel.: +1-(416)-813-7654 (ext. 328443) or +1-647-678-1314; Fax: +1-(416)-813-6637 Received: 19 October 2020; Accepted: 10 November 2020; Published: 17 November 2020 Abstract: Injured peripheral nerves but not central nerves have the capacity to regenerate and reinnervate their target organs. After the two most severe peripheral nerve injuries of six types, crush and transection injuries, nerve fibers distal to the injury site undergo Wallerian degeneration. The denervated Schwann cells (SCs) proliferate, elongate and line the endoneurial tubes to guide and support regenerating axons. The axons emerge from the stump of the viable nerve attached to the neuronal soma. The SCs downregulate myelin-associated genes and concurrently, upregulate growth-associated genes that include neurotrophic factors as do the injured neurons. However, the gene expression is transient and progressively fails to support axon regeneration within the SC-containing endoneurial tubes. Moreover, despite some preference of regenerating motor and sensory axons to “find” their appropriate pathways, the axons fail to enter their original endoneurial tubes and to reinnervate original target organs, obstacles to functional recovery that confront nerve surgeons. Several surgical manipulations in clinical use, including nerve and tendon transfers, the potential for brief low-frequency electrical stimulation proximal to nerve repair, and local FK506 application to accelerate axon outgrowth, are encouraging as is the continuing research to elucidate the molecular basis of nerve regeneration. -

Resident Manual of Trauma to the Face, Head, and Neck
Resident Manual of Trauma to the Face, Head, and Neck First Edition ©2012 All materials in this eBook are copyrighted by the American Academy of Otolaryngology—Head and Neck Surgery Foundation, 1650 Diagonal Road, Alexandria, VA 22314-2857, and are strictly prohibited to be used for any purpose without prior express written authorizations from the American Academy of Otolaryngology— Head and Neck Surgery Foundation. All rights reserved. For more information, visit our website at www.entnet.org. eBook Format: First Edition 2012. ISBN: 978-0-615-64912-2 Preface The surgical care of trauma to the face, head, and neck that is an integral part of the modern practice of otolaryngology–head and neck surgery has its origins in the early formation of the specialty over 100 years ago. Initially a combined specialty of eye, ear, nose, and throat (EENT), these early practitioners began to understand the inter-rela- tions between neurological, osseous, and vascular pathology due to traumatic injuries. It also was very helpful to be able to treat eye as well as facial and neck trauma at that time. Over the past century technological advances have revolutionized the diagnosis and treatment of trauma to the face, head, and neck—angio- graphy, operating microscope, sophisticated bone drills, endoscopy, safer anesthesia, engineered instrumentation, and reconstructive materials, to name a few. As a resident physician in this specialty, you are aided in the care of trauma patients by these advances, for which we owe a great deal to our colleagues who have preceded us. Additionally, it has only been in the last 30–40 years that the separation of ophthal- mology and otolaryngology has become complete, although there remains a strong tradition of clinical collegiality.