Axonotmesis of the Sciatic Nerve
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
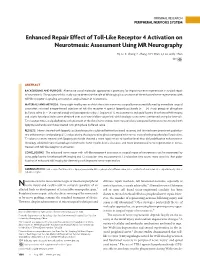
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging
741 Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging DavidS. Titelbaum 1 To investigate the role of MR imaging in wallerian degeneration, a series of animal Joel L. Frazier 2 models of increasingly complex peripheral nerve injury were studied by in vivo MR. Robert I. Grossman 1 Proximal tibial nerves in brown Norway rats were either crushed, transected (neurotomy), Peter M. Joseph 1 or transected and grafted with Lewis rat (allograft) or brown Norway (isograft) donor Leonard T. Yu 2 nerves. The nerves distal to the site of injury were imaged at intervals of 0-54 days after surgery. Subsequent histologic analysis was obtained and correlated with MR Eleanor A. Kassab 1 3 findings. Crush injury, neurotomy, and nerve grafting all resulted in high signal intensity William F. Hickey along the course of the nerve observed on long TR/TE sequences, corresponding to 2 Don LaRossa edema and myelin breakdown from wallerian degeneration. The abnormal signal inten 4 Mark J. Brown sity resolved by 30 days after crush injury and by 45-54 days after neurotomy, when the active changes of wallerian degeneration had subsided. These changes were not seen in sham-operated rats. Our findings suggest that MR is capable of identifying traumatic neuropathy in a peripheral nerve undergoing active wallerian degeneration. The severity of injury may be reflected by the corresponding duration of signal abnormality. With the present methods, MR did not distinguish inflammatory from simple posttraumatic neuropathy. Wallerian degeneration is the axonal degeneration and loss of myelin that occurs when an axon is separated from its cell body. -

Acute Reduction of Microglia Does Not Alter Axonal Injury in a Mouse Model of Repetitive Concussive Traumatic Brain Injury Rachel E
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2014 Acute reduction of microglia does not alter axonal injury in a mouse model of repetitive concussive traumatic brain injury Rachel E. Bennett Washington University School of Medicine David L. Brody Washington University School of Medicine Follow this and additional works at: https://digitalcommons.wustl.edu/open_access_pubs Recommended Citation Bennett, Rachel E. and Brody, David L., ,"Acute reduction of microglia does not alter axonal injury in a mouse model of repetitive concussive traumatic brain injury." Journal of Neurotrauma.31,9. 1647-1663. (2014). https://digitalcommons.wustl.edu/open_access_pubs/4711 This Open Access Publication is brought to you for free and open access by Digital Commons@Becker. It has been accepted for inclusion in Open Access Publications by an authorized administrator of Digital Commons@Becker. For more information, please contact [email protected]. JOURNAL OF NEUROTRAUMA 31:1647–1663 (October 1, 2014) ª Mary Ann Liebert, Inc. DOI: 10.1089/neu.2013.3320 Acute Reduction of Microglia Does Not Alter Axonal Injury in a Mouse Model of Repetitive Concussive Traumatic Brain Injury Rachel E. Bennett and David L. Brody Abstract The pathological processes that lead to long-term consequences of multiple concussions are unclear. Primary mechanical damage to axons during concussion is likely to contribute to dysfunction. Secondary damage has been hypothesized to be induced or exacerbated by inflammation. The main inflammatory cells in the brain are microglia, a type of macrophage. This research sought to determine the contribution of microglia to axon degeneration after repetitive closed-skull traumatic brain injury (rcTBI) using CD11b-TK (thymidine kinase) mice, a valganciclovir-inducible model of macrophage depletion. -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Evidence That Wallerian Degeneration and Localized Axon Degeneration Induced by Local Neurotrophin Deprivation Do Not Involve Caspases
The Journal of Neuroscience, February 15, 2000, 20(4):1333–1341 Evidence That Wallerian Degeneration and Localized Axon Degeneration Induced by Local Neurotrophin Deprivation Do Not Involve Caspases John T. Finn,1 Miguel Weil,1 Fabienne Archer,2 Robert Siman,3 Anu Srinivasan,4 and Martin C. Raff1 1Medical Research Council Laboratory for Molecular Cell Biology and Biology Department and 2Department of Physiology, University College London, London WC1E 6BT, United Kingdom, 3Department of Pharmacology, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania 19104-6084, and 4Idun Pharmaceuticals, Inc., La Jolla, California 92037 The selective degeneration of an axon, without the death of the not activated in the axon during either form of degeneration, parent neuron, can occur in response to injury, in a variety of although it is activated in the dying cell body of the same metabolic, toxic, and inflammatory disorders, and during nor- neurons. Moreover, caspase inhibitors do not inhibit or retard mal development. Recent evidence suggests that some forms either form of axon degeneration, although they inhibit apopto- of axon degeneration involve an active and regulated program sis of the same neurons. Finally, we cannot detect cleaved of self-destruction rather than a passive “wasting away” and in substrates of caspase-3 and its close relatives immunocyto- this respect and others resemble apoptosis. Here we investi- chemically or caspase activity biochemically in axons undergo- gate whether selective axon degeneration depends on some of ing Wallerian degeneration. Our results suggest that a neuron the molecular machinery that mediates apoptosis, namely, the contains at least two molecularly distinct self-destruction pro- caspase family of cysteine proteases. -

Restoration of Neurological Function Following Peripheral Nerve Trauma
International Journal of Molecular Sciences Review Restoration of Neurological Function Following Peripheral Nerve Trauma Damien P. Kuffler 1,* and Christian Foy 2 1 Institute of Neurobiology, Medical Sciences Campus, University of Puerto Rico, 201 Blvd. del Valle, San Juan, PR 00901, USA 2 Section of Orthopedic Surgery, Medical Sciences Campus, University of Puerto Rico, San Juan, PR 00901, USA; [email protected] * Correspondence: dkuffl[email protected] Received: 12 January 2020; Accepted: 3 March 2020; Published: 6 March 2020 Abstract: Following peripheral nerve trauma that damages a length of the nerve, recovery of function is generally limited. This is because no material tested for bridging nerve gaps promotes good axon regeneration across the gap under conditions associated with common nerve traumas. While many materials have been tested, sensory nerve grafts remain the clinical “gold standard” technique. This is despite the significant limitations in the conditions under which they restore function. Thus, they induce reliable and good recovery only for patients < 25 years old, when gaps are <2 cm in length, and when repairs are performed <2–3 months post trauma. Repairs performed when these values are larger result in a precipitous decrease in neurological recovery. Further, when patients have more than one parameter larger than these values, there is normally no functional recovery. Clinically, there has been little progress in developing new techniques that increase the level of functional recovery following peripheral nerve injury. This paper examines the efficacies and limitations of sensory nerve grafts and various other techniques used to induce functional neurological recovery, and how these might be improved to induce more extensive functional recovery. -

Effects of NAD+ in Caenorhabditis Elegans Models of Neuronal Damage
biomolecules Review Effects of NAD+ in Caenorhabditis elegans Models of Neuronal Damage Yuri Lee 1, Hyeseon Jeong 1, Kyung Hwan Park 1 and Kyung Won Kim 1,2,3,* 1 Department of Life Science, Hallym University, Chuncheon 24252, Korea; [email protected] (Y.L.); [email protected] (H.J.); [email protected] (K.H.P.) 2 Convergence Program of Material Science for Medicine and Pharmaceutics, Hallym University, Chuncheon 24252, Korea 3 Multidisciplinary Genome Institute, Hallym University, Chuncheon 24252, Korea * Correspondence: [email protected]; Tel.: +82-33-248-2091 Received: 1 April 2020; Accepted: 30 June 2020; Published: 2 July 2020 Abstract: Nicotinamide adenine dinucleotide (NAD+) is an essential cofactor that mediates numerous biological processes in all living cells. Multiple NAD+ biosynthetic enzymes and NAD+-consuming enzymes are involved in neuroprotection and axon regeneration. The nematode Caenorhabditis elegans has served as a model to study the neuronal role of NAD+ because many molecular components regulating NAD+ are highly conserved. This review focuses on recent findings using C. elegans models of neuronal damage pertaining to the neuronal functions of NAD+ and its precursors, including a neuroprotective role against excitotoxicity and axon degeneration as well as an inhibitory role in axon regeneration. The regulation of NAD+ levels could be a promising therapeutic strategy to counter many neurodegenerative diseases, as well as neurotoxin-induced and traumatic neuronal damage. Keywords: NAD+; Nmnat; NMAT-2; PARP; C. elegans; neuroprotection; axon regeneration 1. NAD+ Biosynthesis Pathway in C. elegans Nicotinamide adenine dinucleotide (NAD+) is found in all living cells and plays an essential role in many fundamental biological processes, such as metabolism, cell signaling, gene expression, and DNA repair [1]. -

Painful Abdominal Wall Nerves
CASE REPORT Reconstructive Treatment of Painful Nerves in the Abdominal Wall Using Processed Nerve Allografts Andrew Bi, BS Eugene Park, MD Summary: Neuromas can be a debilitating cause of pain and often negatively af- Gregory A. Dumanian, MD fect patients’ quality of life. One effective method of treatment involves surgical resection of the painful neuroma and use of a processed nerve allograft to repair the injured nerve segment. Giving the nerve “somewhere to go and something to do” has been shown to effectively alleviate pain in upper and lower extremities. We present the first report of this concept to treat a painful neuroma of the ab- dominal wall that developed following a laparoscopic gastric bypass. The neuroma was excised, and the affected nerve was reconstructed using a processed nerve allograft as an interposition graft, with resolution of pain and gradual return of normal sensation. Patient-reported outcomes were measured using the Patient Reported Outcomes Measurement Information System. Neuroma excision with concurrent interposition grafting using processed nerve allografts may be a promising method of treatment for postsurgical painful neuromas of the trunk. Bi et al. (Plast Reconstr Surg Glob Open 2018;6:e1670; doi: 10.1097/GOX.0000000000001670; Published online 6 March 2018.) INTRODUCTION and unacceptable repeat surgical rates.2 And while wrap- Painful neuromas can form following any surgery when ping the distal point of a painful nerve postneuroma exci- nerves are injured due to cautery or traction. Nerve injury sion -

Diffuse Axonal Injury and Oxidative Stress: a Comprehensive Review
International Journal of Molecular Sciences Review Diffuse Axonal Injury and Oxidative Stress: A Comprehensive Review Alessandro Frati 1,2, Daniela Cerretani 3, Anna Ida Fiaschi 3, Paola Frati 1,4, Vittorio Gatto 4, Raffaele La Russa 1,4 ID , Alessandro Pesce 2, Enrica Pinchi 4, Alessandro Santurro 4 ID , Flavia Fraschetti 2 and Vittorio Fineschi 1,4,* 1 Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Neuromed, Via Atinense 18, 86077 Pozzilli, Italy; [email protected] (A.F.); [email protected] (P.F.); [email protected] (R.L.R.) 2 Department of Neurosciences, Mental Health, and Sensory Organs, Sant’Andrea Hospital, Sapienza University of Rome, Via di Grottarossa 1035, 00189 Rome, Italy; [email protected] (A.P.); fl[email protected] (F.F.) 3 Department of Medicine, Surgery and Neuroscience, University of Siena, Viale Mario Bracci 16, 53100 Siena, Italy; [email protected] (D.C.); annaida.fi[email protected] (A.I.F.) 4 Department of Anatomical, Histological, Forensic and Orthopaedic Sciences, Sapienza University of Rome, Viale Regina Elena 336, 00185 Rome, Italy; [email protected] (V.G.); [email protected] (E.P.); [email protected] (A.S.) * Correspondence: vfi[email protected]; Tel.: +39-06-49912-722; Fax: +39-06-4455-335 Received: 16 September 2017; Accepted: 28 November 2017; Published: 2 December 2017 Abstract: Traumatic brain injury (TBI) is one of the world’s leading causes of morbidity and mortality among young individuals. TBI applies powerful rotational and translational forces to the brain parenchyma, which results in a traumatic diffuse axonal injury (DAI) responsible for brain swelling and neuronal death.