Restoration of Neurological Function Following Peripheral Nerve Trauma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -
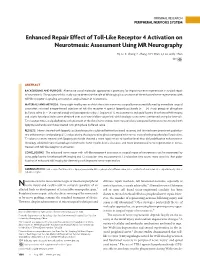
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Biomaterials for the Development of Peripheral Nerve Guidance Conduits
TISSUE ENGINEERING: Part B Volume 18, Number 1, 2012 ª Mary Ann Liebert, Inc. DOI: 10.1089/ten.teb.2011.0240 Biomaterials for the Development of Peripheral Nerve Guidance Conduits Alexander R. Nectow, B.S., M.S.,1 Kacey G. Marra, Ph.D.,2 and David L. Kaplan, Ph.D.1 Currently, surgical treatments for peripheral nerve injury are less than satisfactory. The gold standard of treatment for peripheral nerve gaps > 5 mm is the autologous nerve graft; however, this treatment is associated with a variety of clinical complications, such as donor site morbidity, limited availability, nerve site mismatch, and the formation of neuromas. Despite many recent advances in the field, clinical studies implementing the use of artificial nerve guides have yielded results that are yet to surpass those of autografts. Thus, the development of a nerve guidance conduit, which could match the effectiveness of the autologous nerve graft, would be beneficial to the field of peripheral nerve surgery. Design strategies to improve surgical outcomes have included the development of biopolymers and synthetic polymers as primary scaffolds with tailored mechanical and physical properties, luminal ‘‘fillers’’ such as laminin and fibronectin as secondary internal scaffolds, surface micropatterning, stem cell inclusion, and controlled release of neurotrophic factors. The current article highlights approaches to peripheral nerve repair through a channel or conduit, implementing chemical and physical growth and guidance cues to direct that repair process. Introduction by compression syndrome and often required secondary surgeries for removal.13 Since then, there have been a variety eripheral nerve injury affects 2.8% of patients with of different biomaterials approved for clinical use, such as trauma, presenting a critical clinical issue.1 The postinjury P type I collagen, polyglycolic acid (PGA), poly-DL-lactide-co- axonal anatomy is characterized by primary degeneration with caprolactone (PLCL), and polyvinyl alcohol (PVA). -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Grant Project Che 575 Friday, April 29, 2016 By: Julie Boshar, Matthew
Grant Project ChE 575 Friday, April 29, 2016 By: Julie Boshar, Matthew Long, Andrew Mason, Chelsea Orefice, Gladys Saruchera, Cory Thomas Specific Aims The spinal cord is the body’s most important organ for relaying nerve signals to and from the brain and the body. However, when an individual's spinal cord becomes injured due to trauma, their quality of life is greatly diminished. In the United States today, there are an estimated quarter of a million individuals living with a spinal cord injury (SCI). With an additional 12,000 cases being added every year. Tragically, there is no approved FDA treatment strategy to help restore function to these individuals. SCIs are classified as either primary or secondary events. Primary injuries occur when the spinal cord is displaced by bone fragments or disk material. In this case, nerve signaling rarely ceases upon injury but in severe cases axons are beyond repair. Secondary injuries occur when biochemical processes kill neural cells and strip axons of their myelin sheaths, inducing an inflammatory immune response. In the CNS, natural repair mechanisms are inhibited by proteins and matrix from glial cells, which embody the myelin sheath of axons. This actively prevents the repair of axons, via growth cone inhibition by oligodendrocytes and axon extension inhibition by astrocytes. A promising treatment to SCI use tissue engineered scaffolds that are biocompatible, biodegradable and have strong mechanical properties in vivo. These scaffolds can secrete neurotrophic factors and contain neural progenitor cells to promote axon regeneration, but further research is required to develop this into a comprehensive treatment. -

Axotomy Increases NADPH-Diaphorase Activity in the Dorsal Root Ganglia and Lumbar Spinal Cord of the Turtle Trachemys Dorbigni
Brazilian Journal of Medical and Biological Research (1999) 32: 489-493 NADPH-d after peripheral axotomy in the turtle 489 ISSN 0100-879X Axotomy increases NADPH-diaphorase activity in the dorsal root ganglia and lumbar spinal cord of the turtle Trachemys dorbigni W.A. Partata1, Departamentos de 1Fisiologia and 2Ciências Morfológicas, A.M.R. Krepsky1, Instituto de Ciências Básicas e da Saúde, M. Marques1 and Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brasil M. Achaval2 Abstract Correspondence Seven days after transection of the sciatic nerve NADPH-diaphorase Key words W.A. Partata activity increased in the small and medium neurons of the dorsal root · NADPH-diaphorase Departamento de Fisiologia ganglia of the turtle. However, this increase was observed only in · Axotomy ICBS, UFRGS · medium neurons for up to 90 days. At this time a bilateral increase of Turtle Rua Sarmento Leite, 500 90050-170 Porto Alegre, RS NADPH-diaphorase staining was observed in all areas and neuronal Brasil types of the dorsal horn, and in positive motoneurons in the lumbar Fax: +55-51-316-3166 spinal cord, ipsilateral to the lesion. A similar increase was also demonstrable in spinal glial and endothelial cells. These findings are Research supported by CAPES, CNPq discussed in relation to the role of nitric oxide in hyperalgesia and and FINEP (No. 66.91.0509.00). neuronal regeneration or degeneration. Introduction ever, no studies on the changes of NADPH- Received April 28, 1998 diaphorase activity in turtle spinal cord have Accepted January 11, 1999 Nicotinamide adenine dinucleotide phos- been done. Turtles are interesting experi- phate diaphorase (NADPH-d) is considered mental models because they are thought to to be equivalent to nitric oxide synthase be most closely related to the stem reptilian (NOS), which is the enzyme responsible for and mammalian ancestors. -

Localized Sympathectomy Reduces Mechanical Hypersensitivity by Restoring Normal Immune Homeostasis in Rat Models of Inflammatory Pain
8712 • The Journal of Neuroscience, August 17, 2016 • 36(33):8712–8725 Neurobiology of Disease Localized Sympathectomy Reduces Mechanical Hypersensitivity by Restoring Normal Immune Homeostasis in Rat Models of Inflammatory Pain Wenrui Xie,1 Sisi Chen,1 XJudith A. Strong,1 Ai-Ling Li,1 Ian P. Lewkowich,2 and XJun-Ming Zhang1 1Pain Research Center, Department of Anesthesiology, University of Cincinnati College of Medicine, Cincinnati, Ohio 45267, and 2Division of Immunobiology, Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio 45229 Some forms of chronic pain are maintained or enhanced by activity in the sympathetic nervous system (SNS), but attempts to model this have yielded conflicting findings. The SNS has both pro- and anti-inflammatory effects on immunity, confounding the interpretation of experiments using global sympathectomy methods. We performed a “microsympathectomy” by cutting the ipsilateral gray rami where they entered the spinal nerves near the L4 and L5 DRG. This led to profound sustained reductions in pain behaviors induced by local DRG inflammation (a rat model of low back pain) and by a peripheral paw inflammation model. Effects of microsympathectomy were evident within one day, making it unlikely that blocking sympathetic sprouting in the local DRGs or hindpaw was the sole mechanism. Prior microsympathectomy greatly reduced hyperexcitability of sensory neurons induced by local DRG inflammation observed 4 d later. Microsympathectomy reduced local inflammation and macrophage density in the affected tissues (as indicated by paw swelling and histochemical staining). Cytokine profiling in locally inflamed DRG showed increases in pro-inflammatory Type 1 cytokines and de- creases in the Type 2 cytokines present at baseline, changes that were mitigated by microsympathectomy. -

Peripheral Nerve Regeneration and Muscle Reinnervation
International Journal of Molecular Sciences Review Peripheral Nerve Regeneration and Muscle Reinnervation Tessa Gordon Department of Surgery, University of Toronto, Division of Plastic Reconstructive Surgery, 06.9706 Peter Gilgan Centre for Research and Learning, The Hospital for Sick Children, Toronto, ON M5G 1X8, Canada; [email protected]; Tel.: +1-(416)-813-7654 (ext. 328443) or +1-647-678-1314; Fax: +1-(416)-813-6637 Received: 19 October 2020; Accepted: 10 November 2020; Published: 17 November 2020 Abstract: Injured peripheral nerves but not central nerves have the capacity to regenerate and reinnervate their target organs. After the two most severe peripheral nerve injuries of six types, crush and transection injuries, nerve fibers distal to the injury site undergo Wallerian degeneration. The denervated Schwann cells (SCs) proliferate, elongate and line the endoneurial tubes to guide and support regenerating axons. The axons emerge from the stump of the viable nerve attached to the neuronal soma. The SCs downregulate myelin-associated genes and concurrently, upregulate growth-associated genes that include neurotrophic factors as do the injured neurons. However, the gene expression is transient and progressively fails to support axon regeneration within the SC-containing endoneurial tubes. Moreover, despite some preference of regenerating motor and sensory axons to “find” their appropriate pathways, the axons fail to enter their original endoneurial tubes and to reinnervate original target organs, obstacles to functional recovery that confront nerve surgeons. Several surgical manipulations in clinical use, including nerve and tendon transfers, the potential for brief low-frequency electrical stimulation proximal to nerve repair, and local FK506 application to accelerate axon outgrowth, are encouraging as is the continuing research to elucidate the molecular basis of nerve regeneration. -

A Tissue-Engineered Conduit for Peripheral Nerve Repair
ORIGINAL ARTICLE A Tissue-Engineered Conduit for Peripheral Nerve Repair Tessa Hadlock, MD; Jennifer Elisseeff, BS; Robert Langer, ScD; Joseph Vacanti, MD; Mack Cheney, MD Background: Peripheral nerve repair using autograft ma- formed using a dip-molding technique. They were cre- terial has several shortcomings, including donor site mor- ated containing 1, 2, 4, or 5 sublumina, or “fascicular ana- bidity, inadequate return of function, and aberrant re- logs.” Populations of Schwann cells were isolated, ex- generation. Recently, peripheral nerve research has panded in culture, and plated onto these polymer films, focused on the generation of synthetic nerve guidance where they demonstrated excellent adherence to the poly- conduits that might overcome these phenomena to im- mer surfaces. Regeneration was demonstrated through prove regeneration. In our laboratory, we use the unique several constructs. chemical and physical properties of synthetic polymers in conjunction with the biological properties of Schwann Conclusions: A tubular nerve guidance conduit pos- cells to create a superior prosthesis for the repair of mul- sessing the macroarchitecture of a polyfascicular periph- tiply branched peripheral nerves, such as the facial nerve. eral nerve was created. The establishment of resident Schwann cells onto poly-L-lactic acid and polylactic–co- Objectives: To create a polymeric facial nerve analog glycolic acid surfaces was demonstrated, and the feasi- approximating the fascicular architecture of the extra- bility of in vivo regeneration through the conduit was temporal facial nerve, to introduce a population of shown. It is hypothesized that these tissue-engineered de- Schwann cells into the analog, and to implant the vices, composed of widely used biocompatible, biode- prosthesis into an animal model for assessment of gradable polymer materials and adherent Schwann cells, regeneration. -

Heat Shock Protein 27: Developmental Regulation and Expression After Peripheral Nerve Injury
The Journal of Neuroscience, August 1, 1998, 18(15):5891–5900 Heat Shock Protein 27: Developmental Regulation and Expression after Peripheral Nerve Injury Michael Costigan,1,2 Richard J. Mannion,1,2 Giles Kendall,1 Susan E. Lewis,2 Jason A. Campagna,2 Richard E. Coggeshall,3 Jacqueta Meridith-Middleton,1 Simon Tate,4 and Clifford J. Woolf1,2 1Department of Anatomy and Developmental Biology, University College London, London WC1E 6BT, United Kingdom, 2Neural Plasticity Research Group, Department of Anesthesia and Critical Care, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts 02129, 3Department of Anatomy and Neurobiology, University of Texas Medical Branch, Galveston, Texas 77551, and 4Glaxo-Wellcome Research and Development, Gene Function Unit, Stevenage, Herts SG1 2NY, United Kingdom The heat shock protein (HSP) 27 is constitutively expressed at HSP27 after 24 hr in culture with prominent label throughout the low levels in medium-sized lumbar dorsal root ganglion (DRG) neuron, including the growth cone. HSP27 differs from most cells in adult rats. Transection of the sciatic nerve results in a axonal injury-regulated and growth-associated genes, which ninefold upregulation of HSP27 mRNA and protein in axoto- are typically present at high levels in early development and mized neurons in the ipsilateral DRG at 48 hr, without equivalent downregulated on innervation of their targets, in that its mRNA changes in the mRNAs encoding HSP56, HSP60, HSP70, and is first detectable in the DRG late in development and only HSP90. Dorsal rhizotomy, injuring the central axon of the DRG approaches adult levels by postnatal day 21. In non-neuronal neuron, does not upregulate HSP27 mRNA levels.