Repairing Spinal Roots After Brachial Plexus Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -

Intrapelvic Causes of Sciatica: a Systematic Review
DOI: 10.14744/scie.2020.59354 Review South. Clin. Ist. Euras. 2021;32(1):86-94 Intrapelvic Causes of Sciatica: A Systematic Review 1 1 1 1 Ahmet Kale, Betül Kuru, Gülfem Başol, Elif Cansu Gündoğdu, 1 1 2 3 Emre Mat, Gazi Yıldız, Navdar Doğuş Uzun, Taner A Usta 1Department of Gynecology and Obstetrics, University of Health Sciences, Kartal Dr. Lütfi Kırdar Training and Research Hospital, İstanbul, Turkey 2Department of Gynecology and Obstetrics, Midyat State Hospital, Mardin, Turkey 3Department of Gynecology and Obstetrics, Acıbadem University, Altunizade Hospital, İstanbul, Turkey ABSTRACT Submitted: 09.09.2020 The sciatic nerve is the nerve of the lower limb. It is derived from spinal nerves, fourth Accepted: 27.11.2020 Lumbar (L4) to third Sacral (S3). The sciatic nerve innervates the muscles of the posterior Correspondence: Ahmet Kale, thigh and additionally has sensory functions. Sciatica is the given name to the pain sourced by SBÜ Kartal Dr. Lütfi Kırdar Eğitim irritation of the sciatic nerve. Sciatica is most commonly induced by compression of a lower ve Araştırma Hastanesi, Kadın lumbar nerve root (L4, L5, or S1). Various intrapelvic pathologies include gynecological, Hastalıkları ve Doğum Kliniği, İstanbul, Turkey vascular, traumatic, inflammatory, and tumoral disorders that may cause sciatica. Intrapelvic E-mail: [email protected] pathologies that mimic disc herniation are quite always ignored. Surgical approach and a functional exploration by laparoscopy or robotic surgery have significantly increased the intrapelvic pathology’s awareness, resulting in sciatica. After a detailed assessment of the patient, which causes intrapelvic pathologies, deciding whether surgical or medical therapy is needed, notable results in sciatic pain remission can be done. -

Lumbar Spine Nerve Pain
Contact details Physiotherapy Department, Torbay Hospital, Newton Road, Torquay, Devon TQ2 7AA PATIENT INFORMATION ( 0300 456 8000 or 01803 614567 TorbayAndSouthDevonFT @TorbaySDevonNHS Lumbar Spine www.torbayandsouthdevon.nhs.uk/ Nerve Pain Useful Websites & References www.spinesurgeons.ac.uk British Association of Spinal Surgeons including useful patient information for common spinal treatments https://www.nice.org.uk/guidance/ng59 NICE Guidelines for assessment and management of low back pain and sciatica in over 16s http://videos.torbayandsouthdevon.nhs.uk/radiology Radiology TSDFT website https://www.torbayandsouthdevon.nhs.uk/services/pain- service/reconnect2life/ Pain Service Website Reconnect2Life For further assistance or to receive this information in a different format, please contact the department which created this leaflet. Working with you, for you 25633/Physiotherapy/V1/TSDFT/07.20/Review date 07.22 A Brief Lower Back Anatomy Treatment The normal lower back (lumbar spine) has 5 bones When the clinical diagnosis and MRI findings correlate, (vertebrae) and a collection of nerves which branch out in a target for injection treatment can be identified. This pairs at each level. In between each vertebra there is a disc is known as a nerve root injection, and can both which acts as a shock absorber and spacer. improve symptoms and aid diagnosis. The spinal nerves are like electrical wiring, providing Nerve root injections or ‘nerve root blocks’ are used to signals to areas within the leg. These control sensation and reduce pain in a particular area if you have lower limb pain movement but can cause pain when they are affected. such as sciatica. The injection is done in Radiology. -

Lumbar Disc Herniation
What is a disc herniation (herniated discs)? A disc herniation occurs when a full thickness tear in the outer part of the disc (tear in the dough of the jelly donut) allows the inner portion of the disc (the jelly inside the donut) to leak out of the tear. Because the nerve root lies right next to the intervertebral disc, it gets compressed by the leaked nucleus pulposus (leaked jelly from the donut). This compression of the nerve root can lead to pain, numbness, tingling, burning or the sensation of “pins and needles” that run down the arm or leg. It can also cause weakness in the arm or leg muscles and rarely may lead to loss of bowel or bladder control. MRI of the lumbar spine demonstrating a disc herniation on the right side. This particular patient had severe pain, numbness, tingling and weakness in the right leg. MRI of the neck demonstrating a LARGE disc herniation causing severe spinal cord compression. In a case like this, non-operative treatment is NOT amenable to relieving the pressure on the spinal cord and surgery is recommended as a first line of treatment. A B L4 L4 L5 L5 Herniated Disc C D E Figure. MRI of the lumbar spine demonstrating a disc herniation at L4-5 on the patient’s right side (arrows are pointing at the herniated disc in A, B, D and E). The picture marked C shows a normal part of the spine where there is no herniation. TREATMENT OPTIONS Disc herniations can be treated nonoperatively or may require surgery. -

Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy
Y Lumbar Disc Herniation with Radiculopathy | NASS Clinical Guidelines 1 G Evidence-Based Clinical Guidelines for Multidisciplinary ETHODOLO Spine Care M NE I DEL I U /G ON Diagnosis and Treatment of I NTRODUCT Lumbar Disc I Herniation with Radiculopathy NASS Evidence-Based Clinical Guidelines Committee D. Scott Kreiner, MD Paul Dougherty, II, DC Committee Chair, Natural History Chair Robert Fernand, MD Gary Ghiselli, MD Steven Hwang, MD Amgad S. Hanna, MD Diagnosis/Imaging Chair Tim Lamer, MD Anthony J. Lisi, DC John Easa, MD Daniel J. Mazanec, MD Medical/Interventional Treatment Chair Richard J. Meagher, MD Robert C. Nucci, MD Daniel K .Resnick, MD Rakesh D. Patel, MD Surgical Treatment Chair Jonathan N. Sembrano, MD Anil K. Sharma, MD Jamie Baisden, MD Jeffrey T. Summers, MD Shay Bess, MD Christopher K. Taleghani, MD Charles H. Cho, MD, MBA William L. Tontz, Jr., MD Michael J. DePalma, MD John F. Toton, MD This clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason- ably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is to be made by the physi- cian and patient in light of all circumstances presented by the patient and the needs and resources particular to the locality or institution. I NTRODUCT 2 Lumbar Disc Herniation with Radiculopathy | NASS Clinical Guidelines I ON Financial Statement This clinical guideline was developed and funded in its entirety by the North American Spine Society (NASS). All participating /G authors have disclosed potential conflicts of interest consistent with NASS’ disclosure policy. -

Protection of L1 Nerve Roots in Vertebral Osteotomy for Severe Rigid Thoracolumbar Spine Deformity
Protection of L1 nerve roots in vertebral osteotomy for severe rigid thoracolumbar spine deformity Hang Liao Shenzhen University Houguang Miao Shenzhen University Peng Xie Shenzhen University Yueyue Wang Shenzhen University Ningdao Li Shenzhen University Guizhou Zheng Shenzhen University Xuedong Li Shenzhen University Shixin Du ( [email protected] ) Shenzhen University Research article Keywords: Thoracolumbar deformity, Nerve roots injury, L1 nerve roots, Parallel endplate osteotomy Posted Date: October 2nd, 2019 DOI: https://doi.org/10.21203/rs.2.15567/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/16 Abstract Background: This is a retrospective study of the use of parallel endplate osteotomy (PEO) for correction of severe rigid thoracolumbar spine deformity. Methods : From July 2016 to June 2017, 10 patients with severe rigid thoracolumbar spine deformity underwent PEO on T12 or L1 vertebrae were studied. Results : Following PEO performed at T12 or L1, the kyphosis and scoliosis correction rates reached averages of 77.4 ± 8.5% and 76.6 ± 6.8%, intraoperative bleeding 1990 ± 1010 ml, operation time 7.12 ± 3.88 h. One year after surgery, the SF-36 scores of physical function, role-physical, bodily pain, general health, vitality, social function, role-emotional and mental health from 60 ± 30, 47 ± 33, 44 ± 30, 32 ± 18, 50 ±30, 46 ± 29, 26 ± 40 and 52 ± 20 to 81 ± 16, 69 ± 19, 73 ± 11, 66 ± 21, 74 ± 16, 74 ± 24, 63 ± 37 and 76 ± 12, respectively (P < 0.01). Three patients had symptoms of L1 nerve root injury, as reected by knee extension and hip exion of lower limb weakness and inner thigh numbness, which further conrmed by electromyography. -

Fibrous Adhesive Entrapment of Lumbosacral Nerve Roots As a Cause of Sciatica
Spinal Cord 2001) 39, 269 ± 273 ã 2001 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/01 $15.00 www.nature.com/sc Original Article Fibrous adhesive entrapment of lumbosacral nerve roots as a cause of sciatica K Ido*,1 and H Urushidani1 1Department of Orthopaedic Surgery, Kurashiki Central Hospital, Okayama, Japan Study design: Report of seven patients with ®brous adhesive entrapment of lumbosacral nerve roots as a cause of sciatica, whose radiographic ®ndings were negative and who experienced relief from sciatica immediately after the entrapment was released. Objectives: To describe a new clinical entity of ®brous adhesive entrapment of lumbosacral nerve roots with negative radiographic ®ndings. Setting: Orthopaedic department, Japan. Methods: Clinical evaluation and post-operative outcome in seven patients with entrapment of lumbosacral nerve roots because of ®brous adhesion con®rmed intraoperatively. Results: Radiographic examinations by magnetic resonance imaging &MRI), myelography, and computed tomographic &CT) myelography demonstrated neither disc herniations nor spinal stenosis in all seven patients, and dierential nerve root block was eective for relieving sciatica and low back pain.We con®rmed, intraoperatively, entrapment of the nerve root by ®brous adhesion, and all seven patients were relieved from sciatica and low back pain postoperatively. Conclusion: This study presented seven patients with sciatica caused by ®brous adhesive entrapment of lumbosacral nerve roots who underwent decompression and release of ®brous adhesion.Radiographic examinations, such as MRI, myelography and CT myelography, showed no compressive shadows and also dierential nerve root block was eective for its diagnosis.This study seems to be the ®rst report of patients with entrapment of lumbosacral nerve roots caused by ®brous adhesion, whose radiographic ®ndings were negative. -
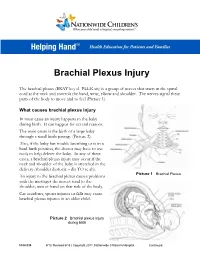
Brachial Plexus Injury
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

Lumbar Degenerative Disease Part 1
International Journal of Molecular Sciences Article Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature 1, , 1,2, 1 Hyeun Sung Kim y * , Pang Hung Wu y and Il-Tae Jang 1 Nanoori Gangnam Hospital, Seoul, Spine Surgery, Seoul 06048, Korea; [email protected] (P.H.W.); [email protected] (I.-T.J.) 2 National University Health Systems, Juronghealth Campus, Orthopaedic Surgery, Singapore 609606, Singapore * Correspondence: [email protected]; Tel.: +82-2-6003-9767; Fax.: +82-2-3445-9755 These authors contributed equally to this work. y Received: 31 January 2020; Accepted: 20 February 2020; Published: 21 February 2020 Abstract: Degenerative disc disease is a leading cause of chronic back pain in the aging population in the world. Sinuvertebral nerve and basivertebral nerve are postulated to be associated with the pain pathway as a result of neurotization. Our goal is to perform a prospective study using radiofrequency ablation on sinuvertebral nerve and basivertebral nerve; evaluating its short and long term effect on pain score, disability score and patients’ outcome. A review in literature is done on the pathoanatomy, pathophysiology and pain generation pathway in degenerative disc disease and chronic back pain. 30 patients with 38 levels of intervertebral disc presented with discogenic back pain with bulging degenerative intervertebral disc or spinal stenosis underwent Uniportal Full Endoscopic Radiofrequency Ablation application through either Transforaminal or Interlaminar Endoscopic Approaches. Their preoperative characteristics are recorded and prospective data was collected for Visualized Analogue Scale, Oswestry Disability Index and MacNab Criteria for pain were evaluated.