Timing of Surgery in Traumatic Brachial Plexus Injury: a Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -
Clinical Excellence Series Volume V an Evidence-Based Approach to Traumatic Emergencies
Clinical Excellence Series n Volume V An Evidence-Based Approach To Traumatic Emergencies Inside Neck Trauma: Don’t Put Your Neck On The Line Orthopedic Sports Injuries: Off The Sidelines And Into The Emergency Department Blunt Abdominal Trauma: Priorities, Procedures, And Pragmatic Thinking Wrist Injuries: Emergency Imaging And Management Brought to you exclusively by the publisher of: An Evidence-Based Approach To Traumatic Emergencies CEO: Robert Williford President & Publisher: Stephanie Ivy Associate Editor & CME Director: Jennifer Pai • Associate Editor: Dorothy Whisenhunt Director of Member Services: Liz Alvarez • Marketing & Customer Service Coordinator: Robin Williford Direct all questions to EB Medicine: 1-800-249-5770 • Fax: 1-770-500-1316 • Non-U.S. subscribers, call: 1-678-366-7933 EB Medicine • 5550 Triangle Pkwy Ste 150 • Norcross, GA 30092 E-mail: [email protected] • Web Site: www.ebmedicine.net The Emergency Medicine Practice Clinical Excellence Series, Volume V: An Evidence-Based Approach To Traumatic Emergencies is published by EB Practice, LLC, 5550 Triangle Pkwy Ste 150, Norcross, GA 30092. Opinions expressed are not necessarily those of this publication. Mention of products or services does not constitute endorsement. This publication is intended as a general guide and is intended to supplement, rather than substitute, professional judgment. It covers a highly technical and complex subject and should not be used for making specific medical decisions. The materials contained herein are not intended to establish policy, procedure, or standard of care. Emergency Medicine Practice, The Emergency Medicine Practice Clinical Excel- lence Series, and An Evidence-Based Approach to Traumatic Emergencies are trademarks of EB Practice, LLC. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -

Broken Bones: Common Pediatric Lower Extremity Fractures—Part III
10173-06_ON2506-Hart.qxd 11/9/06 3:51 PM Page 390 Broken Bones: Common Pediatric Lower Extremity Fractures—Part III Erin S. Hart ▼ Brenda Luther ▼ Brian E. Grottkau Lower extremity injuries and fractures occur frequently in young usually have pain with hamstring stretching and hip flex- children and adolescents. Nurses are often one of the first ion/abduction). Patients also frequently demonstrate an healthcare providers to assess a child with an injury or fracture. antalgic gait and have pain during their activity or sport. Although basic fracture care and principles can be applied, An anteroposterior radiograph of the pelvis usually reveals nurses caring for these young patients must have a good under- the avulsed fragment. Comparative views of the contralat- standing of normal bone growth and development as well as eral side are often helpful in confirming the diagnosis and avoiding further unnecessary advanced imaging studies. common mechanisms of injury and fracture patterns seen in This injury is usually treated symptomatically and often children. Similar to many of the injuries in the upper extremity, involves rest, application of ice, and relaxation of the in- fractures in the lower extremity in children often can be treated volved tendon (O’Kane, 1999). Conservative treatment of nonoperatively with closed reduction and casting. However, this pelvic avulsion fractures is usually successful. Crutches are article will also review several lower extremity fractures that often needed for several weeks to reduce symptoms and frequently require surgical intervention to obtain a precise rest the extremity involved. Complications following pelvic anatomical reduction. Common mechanisms of injury, fracture avulsion fractures in children are rare, and most patients patterns, and current management techniques will be discussed. -

Treatment of Large Avulsion Injury in Perianal, Sacral, and Perineal
Hu et al. BMC Surgery (2019) 19:65 https://doi.org/10.1186/s12893-019-0529-1 RESEARCH ARTICLE Open Access Treatment of large avulsion injury in perianal, sacral, and perineal regions by island flaps or skin graft combined with vacuum assisted closure Fu Xing Hu1†, Xiao Xuan Hu2†, Xue Lin Yang1, Xing Hai Han1, Yong Bo Xu3, Kun Li3, Li Yan3*† and Hai Bo Chu3*† Abstract Background: Traumatic avulsion injuries to the anus, although uncommon, can result in serious complications and even death. Management of anal avulsion injuries remains controversial and challenging. This study aimed to investigate the clinical effects of treating large skin and subcutaneous tissue avulsion injuries in the perianal, sacral, and perineal regions with island flaps or skin graft combined with vacuum assisted closure. Methods: Island flaps or skin graft combined with vacuum assisted closure, diverting ileostomy, the rectum packed with double-lumen tubes around Vaseline gauze, negative pressure drainage with continuous distal washing, wounds with skin grafting as well as specialized treatment were performed. Results: The injuries healed in all patients. Six cases had incomplete perianal avulsion without wound infection. Wound infection was seen in four cases with annular perianal avulsion and was controlled, and the separated prowl lacuna was closed. The survival rate in 10 patients who underwent skin grafting was higher than 90%. No anal stenosis was observed after surgery, and ileostomy closure was performed at 3 months (six cases) and 6 months (four cases) after surgery, respectively. Conclusions: Covering a wound with an island flap or skin graft combined with vacuum assisted closure is successful in solving technical problems, protects the function of the anus and rapidly seals the wound at the same time. -
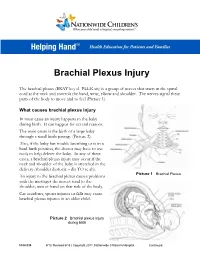
Brachial Plexus Injury
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

Extrusive Luxation and Lateral Luxation
NDR15 1/3/07 6:23 PM Page 411 15 Extrusive Luxation and Lateral Luxation F. M. Andreasen & J. O. Andreasen Definition Clinical findings Extrusive luxation (peripheral dislocation, Extrusion partial avulsion) Extruded teeth appear elongated and most often with Partial displacement of the tooth out of its socket. (Fig. lingual deviation of the crown, as the tooth is suspended 15.1) only by the palatinal gingiva (Fig. 15.1). There is always bleeding from the periodontal ligament. The percussion sound is dull. Lateral luxation Displacement of the tooth in a direction other than axially. Lateral luxation This is accompanied by comminution or fracture of the The crowns of laterally luxated teeth are in most cases dis- alveolar socket. (Fig. 15.2) placed lingually and are usually associated with fractures of the vestibular part of the socket wall (Fig. 15.2). Displace- Frequency ment of teeth after lateral luxation is normally evident by visual inspection. However, in case of marked inclination of The frequency of extrusive and lateral luxation han been maxillary teeth, it can be difficult to decide whether the found to be 7% and 11% among traumatized permanent trauma has caused minor abnormalities in tooth position. teeth examined at a major trauma center (7). In such cases, occlusion should be checked. Due to the fre- quently locked position of the tooth in the alveolus, clinical findings revealed by percussion and mobility tests are iden- Healing and pathology tical with those found in intruded teeth (see Chapter 13, Table 13.1). In these cases there is a complete rupture of the neurovas- cular supply to the pulp and severance of periodontal liga- Radiographic findings ment fibers leading to extrusion. -

Nerve Transfers for Restoration of Finger Flexion in Patients with Tetraplegia
CLINICAL ARTICLE J Neurosurg Spine 26:55–61, 2017 Nerve transfers for restoration of finger flexion in patients with tetraplegia Jayme A. Bertelli, MD, PhD,1,2 and Marcos F. Ghizoni, MD, MSc2 1Center of Biological and Health Sciences, Department of Neurosurgery, University of the South of Santa Catarina (Unisul), Tubarão; and 2Department of Orthopedic Surgery, Governador Celso Ramos Hospital, Florianópolis, Santa Catarina, Brazil OBJECTIVE The purpose of this paper was to report the authors’ results with finger flexion restoration by nerve transfer in patients with tetraplegia. METHOds Surgery was performed for restoration of finger flexion in 17 upper limbs of 9 patients (8 male and 1 female) at a mean of 7.6 months (SD 4 months) after cervical spinal cord injury. The patients’ mean age at the time of surgery was 28 years (SD 15 years). The motor level according to the ASIA (American Spinal Injury Association) classification was C-5 in 4 upper limbs, C-6 in 10, and C-7 in 3. In 3 upper limbs, the nerve to the brachialis was transferred to the anterior interosseous nerve (AIN), which was sepa- rated from the median nerve from the antecubital fossa to the midarm. In 5 upper limbs, the nerve to the brachialis was transferred to median nerve motor fascicles innervating finger flexion muscles in the midarm. In 4 upper limbs, the nerve to the brachioradialis was transferred to the AIN. In the remaining 5 upper limbs, the nerve to the extensor carpi radialis brevis (ECRB) was transferred to the AIN. Patients were followed for an average of 16 months (SD 6 months). -

After Intraspinal Repair of C5–T1 Brachial Plexus Avulsion Injury
Neurosurg Focus 16 (5):Article 7, 2004, Click here to return to Table of Contents Restoration of hand function and so called “breathing arm” after intraspinal repair of C5–T1 brachial plexus avulsion injury Case report THOMAS CARLSTEDT, M.D., D.M., F.R.C.S., PRAVEEN ANAND, M.D., F.R.C.P., MIN HTUT, M.R.C.P., PETER MISRA, M.D., F.R.C.P., AND MIKAEL SVENSSON, M.D., D.M. The Periphery Nerve Injury Unit, The Royal National Orthopaedic Hospital, Stanmore; Peripheral Neuropathy Unit, Imperial College, Hammersmith Hospital, London, United Kingdom; and Department of Neurosurgery, Karolinska Hospital, Stockholm, Sweden This 9-year-old boy sustained a complete right-sided C5–T1 brachial plexus avulsion injury in a motorcycle acci- dent. He underwent surgery 4 weeks after the accident. The motor-related nerve roots in all parts of the avulsed brachial plexus were reconnected to the spinal cord by reimplantation of peripheral nerve grafts. Recovery in the proximal part of the arm started 8 to 10 months later. Motor function was restored throughout the arm and also in the intrinsic mus- cles of the hand by 2 years postoperatively. The initial severe excruciating pain, typical after nerve root avulsions, dis- appeared completely with motor recovery. The authors observed good recruitment of regenerated motor units in all parts of the arm, but there were cocontractions. Transcranial magnetic stimulation produced response in all muscles, with prolonged latency and smaller amplitude compared with the intact side. There was inspiration-evoked muscle activity in proximal arm muscles—that is, the so-called “breathing arm” phenomenon. -

Delayed Diagnosis of Ureteropelvic Junction Avulsion in a Child Owing to Unstable Hemodynamics Jae Min Chung, Su Yung Kim and Sang Don Lee
CASE STUDY Delayed diagnosis of ureteropelvic junction avulsion in a child owing to unstable hemodynamics Jae Min Chung, Su Yung Kim and Sang Don Lee Background. A 7-year-old previously healthy girl was injured in a traffic accident and presented to the emergency room with abdominal pain, microscopic hematuria, and wide skin defects and deep lacerations on the left flank, left upper abdomen, and right inguinal area. Initial CT of the abdomen was unremarkable. 3 weeks later, the patient complained of abdominal distension, left flank pain, and fever. Investigations. Blood and urine tests, CT of the abdomen, chest X-ray, antegrade pyelography, intravenous urography, renal ultrasonography and diuretic renal scan. Diagnosis. Complete avulsion injury of the left ureteropelvic junction Management. The patient underwent 11 plastic reconstructive surgeries, including a skin grafting operation. A percutaneous nephrostomy was performed for temporary diversion. After complete healing of the left flank wound, open pyeloplasty was performed to create a ureteropelvic anastomosis with stent. The patient was discharged 1 week after surgery and the stent was removed 5 weeks later. 5 years after pyeloplasty, her renal function was normal and she had experienced no complications. Chung, J. M. et al. Nat. Rev. Urol. 6, 509–512 (2009); doi:10.1038/nrurol.2009.148 The case A 7‑year‑old previously healthy girl presented to the Blood tests performed 7 days after surgery revealed emergency room after being crushed by a heavy‑duty the patient was hemodynamically stable, with only truck. On presentation, she was tachycardic and hypo‑ mild leuko cytosis (white blood cell count 13.6 × 109/l; tensive with tachypnea.