Intraventricular Hemorrhage (IVH)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -

Apparent Atypical Callosal Dysgenesis: Analysis of MR Findings in Six Cases and Their Relationship to Holoprosencephaly
333 Apparent Atypical Callosal Dysgenesis: Analysis of MR Findings in Six Cases and Their Relationship to Holoprosencephaly A. James Barkovich 1 The MR scans of six pediatric patients with apparent atypical callosal dysgenesis (presence of the dorsal corpus callosum in the absence of a rostral corpus callosum) were critically analyzed and correlated with developmental information in order to assess the anatomic, embryologic, and developmental implications of this unusual anomaly. Four patients had semilobar holoprosencephaly; the dorsal interhemispheric commis sure in these four infants resembled a true callosal splenium. All patients in this group had severe developmental delay. The other two patients had complete callosal agenesis with an enlarged hippocampal commissure mimicking a callosal splenium; both were developmentally and neurologically normal. The embryologic implications of the pres ence of these atypical interhemispheric connections are discussed. Differentiation between semilobar holoprosencephaly and agenesis of the corpus callosum with enlarged hippocampal commissure-two types of apparent atypical callosal dysgenesis-can be made by obtaining coronal, short TR/TE MR images through the frontal lobes. Such differentiation has critical prognostic implications. AJNR 11:333-339, March{Apri11990 Abnormalities of the corpus callosum are frequently seen in patients with con genital brain malformations [1-5); a recent publication [5) reports an incidence of 47%. The corpus callosum normally develops in an anterior to posterior direction. The genu forms first, followed by the body, splenium, and rostrum. Dysgenesis of the corpus callosum is manifested by the presence of the earlier-formed segments (genu , body) and absence of the later-formed segments (splenium, rostrum) [4-6]. We have recently encountered six patients with findings suggestive of atypical callosal dysgenesis in whom there was apparent formation of the callosal splenium in the absence of the genu and body. -

CONGENITAL ABNORMALITIES of the CENTRAL NERVOUS SYSTEM Christopher Verity, Helen Firth, Charles Ffrench-Constant *I3
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.suppl_1.i3 on 1 March 2003. Downloaded from CONGENITAL ABNORMALITIES OF THE CENTRAL NERVOUS SYSTEM Christopher Verity, Helen Firth, Charles ffrench-Constant *i3 J Neurol Neurosurg Psychiatry 2003;74(Suppl I):i3–i8 dvances in genetics and molecular biology have led to a better understanding of the control of central nervous system (CNS) development. It is possible to classify CNS abnormalities Aaccording to the developmental stages at which they occur, as is shown below. The careful assessment of patients with these abnormalities is important in order to provide an accurate prog- nosis and genetic counselling. c NORMAL DEVELOPMENT OF THE CNS Before we review the various abnormalities that can affect the CNS, a brief overview of the normal development of the CNS is appropriate. c Induction—After development of the three cell layers of the early embryo (ectoderm, mesoderm, and endoderm), the underlying mesoderm (the “inducer”) sends signals to a region of the ecto- derm (the “induced tissue”), instructing it to develop into neural tissue. c Neural tube formation—The neural ectoderm folds to form a tube, which runs for most of the length of the embryo. c Regionalisation and specification—Specification of different regions and individual cells within the neural tube occurs in both the rostral/caudal and dorsal/ventral axis. The three basic regions of copyright. the CNS (forebrain, midbrain, and hindbrain) develop at the rostral end of the tube, with the spinal cord more caudally. Within the developing spinal cord specification of the different popu- lations of neural precursors (neural crest, sensory neurones, interneurones, glial cells, and motor neurones) is observed in progressively more ventral locations. -

Germinal Matrix-Intraventricular Hemorrhage: a Tale of Preterm Infants
Hindawi International Journal of Pediatrics Volume 2021, Article ID 6622598, 14 pages https://doi.org/10.1155/2021/6622598 Review Article Germinal Matrix-Intraventricular Hemorrhage: A Tale of Preterm Infants Walufu Ivan Egesa ,1 Simon Odoch,1 Richard Justin Odong,1 Gloria Nakalema,1 Daniel Asiimwe ,2 Eddymond Ekuk,3 Sabinah Twesigemukama,1 Munanura Turyasiima ,1 Rachel Kwambele Lokengama,1 William Mugowa Waibi ,1 Said Abdirashid,1 Dickson Kajoba,1 and Patrick Kumbowi Kumbakulu1 1Department of Paediatrics and Child Health, Faculty of Clinical Medicine and Dentistry, Kampala International University, Uganda 2Department of Surgery, Faculty of Clinical Medicine and Dentistry, Kampala International University, Uganda 3Department of Surgery, Faculty of Medicine, Mbarara University of Science and Technology, Uganda Correspondence should be addressed to Walufu Ivan Egesa; [email protected] Received 20 December 2020; Accepted 26 February 2021; Published 16 March 2021 Academic Editor: Somashekhar Marutirao Nimbalkar Copyright © 2021 Walufu Ivan Egesa et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Germinal matrix-intraventricular hemorrhage (GM-IVH) is a common intracranial complication in preterm infants, especially those born before 32 weeks of gestation and very-low-birth-weight infants. Hemorrhage originates in the fragile capillary network of the subependymal germinal matrix of the developing brain and may disrupt the ependymal lining and progress into the lateral cerebral ventricle. GM-IVH is associated with increased mortality and abnormal neurodevelopmental outcomes such as posthemorrhagic hydrocephalus, cerebral palsy, epilepsy, severe cognitive impairment, and visual and hearing impairment. -

Sonic Hedgehog Regulates Proliferation and Inhibits Differentiation of CNS Precursor Cells
The Journal of Neuroscience, October 15, 1999, 19(20):8954–8965 Sonic hedgehog Regulates Proliferation and Inhibits Differentiation of CNS Precursor Cells David H. Rowitch,1,2 Benoit St.-Jacques,1 Scott M. K. Lee,1 Jonathon D. Flax,2 Evan Y. Snyder,2 and Andrew P. McMahon1 1Department of Molecular and Cellular Biology, Harvard University, Cambridge, Massachusetts 02138, and 2Division of Newborn Medicine, Department of Pediatrics, Harvard Medical School, Boston, Massachusetts 02115 Activation of the Sonic hedgehog (Shh) signal transduction Shh-responsive but postmitotic were present in persistent pathway is essential for normal pattern formation and cellular structures reminiscent of the ventricular zone germinal matrix. differentiation in the developing CNS. However, it is also This tissue remained blocked in an undifferentiated state. These thought to be etiological in primitive neuroectodermal tumors. results indicate that cellular competence restricts the prolifera- We adapted GAL4/UAS methodology to ectopically express tive response to Shh in vivo and provide evidence that prolifer- full-length Shh in the dorsal neural tube of transgenic mouse ation and differentiation can be regulated separately in precur- embryos commencing at 10 d postcoitum (dpc), beyond the sor cells of the spinal cord. Thus, Hedgehog signaling may period of primary dorsal–ventral pattern formation and floor- contribute to CNS tumorigenesis by directly enhancing prolif- plate induction. Expression of Shh was maintained until birth, eration and preventing neural differentiation in selected precur- permitting us to investigate effects of ongoing exposure to Shh sor cells. on CNS precursors in vivo. Proliferative rates of spinal cord Key words: Sonic hedgehog; tumorigenesis; GAL4; central precursors were twice that of wild-type littermates at 12.5 dpc. -

Development of the Skin and Its Derivatives
Development of the skin and its derivatives Resources: http://php.med.unsw.edu.au/embryology/ Larsen’s Human Embryology – Chapter 7 The Developing Human: Clinically Oriented Embryology Dr Annemiek Beverdam – School of Medical Sciences, UNSW Wallace Wurth Building Room 234 – [email protected] Lecture overview Skin function and anatomy Skin origins Development of the overlying epidermis Development of epidermal appendages: Hair follicles Glands Nails Teeth Development of melanocytes Development of the Dermis Resources: http://php.med.unsw.edu.au/embryology/ Larsen’s Human Embryology – Chapter 7 The Developing Human: Clinically Oriented Embryology Dr Annemiek Beverdam – School of Medical Sciences, UNSW Wallace Wurth Building Room 234 – [email protected] Skin Function and Anatomy Largest organ of our body Protects inner body from outside world (pathogens, water, sun) Thermoregulation Diverse: thick vs thin skin, scalp skin vs face skin, etc Consists of: - Overlying epidermis - Epidermal appendages: - Hair follicles, - Glands: sebaceous, sweat, apocrine, mammary - Nails - Teeth - Melanocytes - (Merkel Cells - Langerhans cells) - Dermis - Hypodermis Skin origins Trilaminar embryo Ectoderm (Neural crest) brain, spinal cord, eyes, peripheral nervous system epidermis of skin and associated structures, melanocytes, cranial connective tissues (dermis) Mesoderm musculo-skeletal system, limbs connective tissue of skin and organs urogenital system, heart, blood cells Endoderm epithelial linings of gastrointestinal and respiratory tracts Ectoderm -

Moderate-Grade Germinal Matrix Haemorrhage Activates Cell Division in the 1 Neonatal Mouse Subventricular Zone. 2 3 William J Da
1 Moderate-grade germinal matrix haemorrhage activates cell division in the 2 neonatal mouse subventricular zone. 3 4 William J Dawes1*, Xinyu Zhang1, Stephen P.J. Fancy2, David Rowitch2 and Silvia 5 Marino1* 6 7 1 Blizard Institute, Barts and The London School of Medicine and Dentistry, Queen 8 Mary University of London, 4 Newark Street, London E1 2AT, UK 9 2 Departments of Pediatrics and Neurosurgery, Eli and Edythe Broad Institute for 10 Stem Cell Research and Regeneration Medicine and Howard Hughes Medical 11 Institute, University of California San Francisco, 513 Parnassus Avenue, San 12 Francisco, CA, 94143, USA 13 * Corresponding authors 14 William J Dawes and Silvia Marino 15 Blizard Institute, 4 Newark Street, London E1 2AT 16 Tel +44 207 882 2585, 17 Fax +44 207 882 2180, 18 Email: [email protected] 19 20 Running title: Neural stem cells and neonatal brain haemorrhage 21 22 Abstract 23 Precise temporal and spatial control of the neural stem progenitor cells within the 24 subventricular zone germinal matrix of the brain is important for normal development 25 in the third trimester and early postnatal period. High metabolic demands of 26 proliferating germinal matrix precursors, coupled with the flimsy structure of the 27 germinal matrix cerebral vasculature, are thought to account for high rates of 28 haemorrhage in extremely- and very-low birth weight preterm infants. Germinal 29 matrix haemorrhage can commonly extend to intraventricular haemorrhage. Because 30 neural stem progenitor cells are sensitive to micro-environmental cues from the 31 ventricular, intermediate and basal domains within the germinal matrix, haemorrhage 32 has been postulated to impact neurological outcome through aberration of normal 33 neural stem/progenitor cells behaviour 34 35 We have developed an animal model of neonatal germinal matrix haemorrhage using 36 stereotactic injection of autologous blood into the mouse neonatal germinal matrix. -

Pericytes in Microvessels: from “Mural” Function to Brain and Retina Regeneration
International Journal of Molecular Sciences Review Pericytes in Microvessels: From “Mural” Function to Brain and Retina Regeneration 1, 2, 2 3 Nunzia Caporarello y, Floriana D’Angeli y, Maria Teresa Cambria , Saverio Candido , Cesarina Giallongo 4, Mario Salmeri 5, Cinzia Lombardo 5, Anna Longo 2, Giovanni Giurdanella 2, Carmelina Daniela Anfuso 2,* and Gabriella Lupo 2,* 1 Department of Physiology & Biomedical Engineering, Mayo Clinic, Rochester, MN 55905, USA; [email protected] 2 Section of Medical Biochemistry, Department of Biomedical and Biotechnological Sciences, School of Medicine, University of Catania, 95123 Catania, Italy; fl[email protected] (F.D.); [email protected] (M.T.C.); [email protected] (A.L.); [email protected] (G.G.) 3 Section of General and Clinical Pathology and Oncology, Department of Biomedical and Biotechnological Sciences, School of Medicine, University of Catania, 95123 Catania, Italy; [email protected] 4 Section of Haematology, Department of General Surgery and Medical-Surgical Specialties, University of Catania, 95123 Catania, Italy; [email protected] 5 Section of Microbiology, Department of Biomedical and Biotechnological Sciences, School of Medicine, University of Catania, 95123 Catania, Italy; [email protected] (M.S.); [email protected] (C.L.) * Correspondence: [email protected] (G.L.); [email protected] (C.D.A.); Tel.: +39-095-4781158 (G.L.); +39-095-4781170 (C.D.A.) These authors contributed equally to this work. y Received: 31 October 2019; Accepted: 14 December 2019; Published: 17 December 2019 Abstract: Pericytes are branched cells located in the wall of capillary blood vessels that are found throughout the body, embedded within the microvascular basement membrane and wrapping endothelial cells, with which they establish a strong physical contact. -
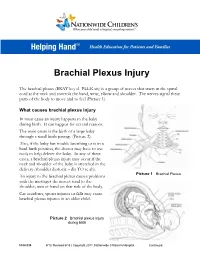
Brachial Plexus Injury
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye .