Chapter 4: Results
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Analisis Pemasaran Emping Melinjo Di Kabupaten Sragen SKRIPSI Oleh
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Sebelas Maret Institutional Repository Analisis pemasaran emping melinjo di kabupaten Sragen SKRIPSI Oleh : Iryani Riastuti H0304081 FAKULTAS PERTANIAN UNIVERSITAS SEBELAS MARET SURAKARTA 2008 I. PENDAHULUAN A. Latar Belakang Pembangunan pertanian pada dasarnya mempunyai tujuan yaitu untuk meningkatkan hasil dan mutu produksi pertanian, memperluas lapangan pekerjaan, meningkatkan taraf hidup petani, meningkatkan devisa negara serta menunjang kegiatan industri. Kegiatan industri di Indonesia telah berkembang di berbagai usaha baik industri skala rumah tangga, industri kecil, dan industri skala besar. Sektor yang sesuai dengan industri tersebut adalah agroindustri, karena didukung oleh sumber daya alam pertanian yang mampu menghasilkan berbagai produk olahan. Menurut Soekartawi (2001), sebagai motor penggerak pembangunan pertanian agroindustri mempunyai peranan penting dalam kegiatan pembangunan daerah, baik dalam sasaran pemerataan pembangunan, pertumbuhan ekonomi maupun stabilitas nasional. Agroindustri terutama usaha skala kecil dan skala rumah tangga menjadi penting dalam perekonomian Indonesia menuju perubahan dari sektor pertanian menuju basis ekonomi non pertanian. Perubahan tersebut berlangsung sejalan dengan semakin meningkatnya kebutuhan masyarakat pada barang dan jasa, kesempatan kerja, dan penghasilan yang lebih baik serta meningkatnya modal. Agroindustri merupakan suatu sistem pengolahan secara terpadu antara sektor pertanian dengan sektor -

Master Thesis
Master thesis in History: Migration and Global Interdependence !Research Master Programme ! ! ! INDONESIAN AND MOROCCAN EATING CULTURES AT THE DUTCH TABLE: A CULINARY HISTORY OF ADAPTATION AND AUTHENTICITY (1950-2000) ! ! ! ! SAMUELA ETOSSI [email protected] ! Supervisor: Prof. Dr. Leo Lucassen Professor of Social History and Academic Director of the Institute of History at Leiden !University Second reviewer: Prof. Dr. Marlou Schrover Professor in Migration History at Leiden University ! ! ! !Contents !Introduction ………………………………………………………………………………….……3 1.The integration of post-colonial and labor migrants within shifting Dutch immigrant policies (1945-2000s)……………………………………………………………………………………..17 1.1.‘Not a country of immigration’ (post-World War II until mid-1970s)……………… 17 1.2. The Dutch multicultural model (1970s)……………………………………………. 25 1.3. The Ethnic Minority Policy (1980s)……………………………………………….. 29 1.4. The Integration Policy (1990s)…………………………………………………….. 32 1.5. The Integration Policy ‘New Style’ (2000s)……………………………………….. 35 1.6. A brief comparison between the integration of post-colonial and labour migrants………………………………………………………………………………….37 ! 2. Change and continuity in the Dutch eating culture (1950s-1990s/2000s)…………………….44 2.1. The post-war Dutch culinary panorama (1950s)……………………………………44 2.2. Social factors and technological developments……………………………………..45 2.3.1960s-1990s: the decades of gastronomic diversity and eating out ethnic…………..46 ! 3. The influence of foreign cuisines at the Dutch table: Margriet’s culinary columns (1950-2000) -

Chocolate Snow Skin Moon Cakes 巧克力冰皮月餅/巧克力冰皮月饼
Chocolate Snow Skin Moon Cakes 巧克力冰皮月餅/巧克力冰皮月饼 Prep time: 60 minutes Make time: 60 minutes Total Time: 2 hours Yield: 12 mooncakes (50g each) Ingredients: Snow Skin Dough: 200g Snow skin premix powder 40g Vegetable shortening 200g Water (in room temperature) A few Coco powders/ any food powder (optional) 1 cup Cooked flour to dust the mooncake and the mold Filling: Half of a Chocolate Cake (break it into pieces): I used this recipe from Add a Pinch. Chocolate Ganache: I also used the recipe from Add a Pinch to make my chocolate ganache. Chocolate covered rice crispies (optional) Milk Instructions: For the Filling: 1. Bake a chocolate cake and break it into pieces. 2. Make a batch of chocolate ganache. After it cools down, add some chocolate cereal for a better texture. 3. Mix both chocolate cake and the ganache together. and add some milk to make it creamy. 4. Put it in the fridge. Chill for at least an hour. For the Snow Skin Dough: 1. Mix all the ingredients together, and add some Coco powder for the color of the dough. 2. Put it in the fridge. Chill for at least an hour. Making the Mooncakes: 1. When both chocolate mixture and the dough are firm enough to handle, divide them into 25g portions each and roll into a ball. 2. In the meantime, put about a cup of flour into a steamer to steam it for 5 minutes. Take it out and cool down. 3. Flatten the dough. Place the filling into the center of the dough. -

Banana Blue Monster Butter Pecan Banana Cream Pie
BANANA BLUE MONSTER BUTTER PECAN Banana flavored Ice Cream Blue Vanilla Ice Cream with Oreo® Cookies Butter Pecan flavored Ice Cream with Using Fresh Bananas and Nestle® Chocolate Chip Cookies Whole Roasted, Buttered and Salted Pecans BANANA CREAM PIE BLUE MOON CAKE BATTER Banana Ice Cream with Marshmallow Ripple Blue Raspberry Yellow Cake Batter and Sugar Cookie Gems flavored Ice Cream flavored Ice Cream BIRTHDAY CAKE BLUEBERRY COBBLER CHEESECAKE WITH OREO® Cake Batter Ice Cream Vanilla Ice Cream Cheesecake flavored Ice Cream with Cheesecake with a Blue Butter Cream Ripple and Sprinkles with Blueberry Ripple and Sugar Cookie Gems Chunks, Oreo® Pieces and Oreo® Crumbs BLACK CHERRY BROWNIE DOUGH CHERRY VANILLA Black Cherry flavored Ice Cream Chocolate and Vanilla Ice Cream Layered Vanilla Ice Cream with Whole Black Cherries with Cookie Dough and Brownie Pieces with Whole Maraschino Cherries BLACK RASPBERRY BUCKEYE CHOC. PEANUT BUTTER BROWNIE Black Raspberry Peanut Butter Ice Cream Chocolate Ice Cream with Reese’s Peanut flavored Ice Cream with Fudge Ripple and Buckeye Candy Pieces Butter® Ripple and Brownie Chunks CHOCOHOLIC CHUNK CHOCOLATE PECAN GRAHAM CENTRAL STATION Deep Dark Chocolate Ice Cream Chocolate Ice Cream Graham flavored Ice Cream with a Graham Cracker with Dark Chocolate Chips with Whole Roasted, Buttered and Salted Pecans Ripple and Chocolate Covered crunchies CHOCOLATE COCONUT CREAM PIE GREEN TEA Chocolate Coconut Ice Cream with Marshmallow Ripple, Green Tea flavored Ice Cream Coconut Flakes and Sugar Cookie Gems flavored -

Ala Carte Menu
Authentic and Creative Asian Inspirations TO START OR SHARE Daily Ocean Harvest Sushi or Sashimi Chuka Wakame Salad “VG” 18 2 pcs. Wagyu Nigiri “SF” 20 Green leaves, avocado, tomato, sesame dressing Sliced wagyu striploin, Krystal caviar, fresh wasabi, scallion Papaya Salad Roll “SF” 18 Vegan Sushi “V” “GF” “VG” 25 Green papaya, tamarind sauce Avocado, red cabbage, mango Soba Noodle Salad “N” “VG” 20 2 pcs. Otoro Nigiri “SF” 30 Brown Japanese noodle, mixed lettuce, peanut sauce Sliced tuna belly glazed with kabayaki sauce, fresh grated wasabi, ginger pickles Gado Gado “V” “N” “GF” 20 Boiled mixed vegetables, white cabbage, long 6 pcs. Crazy Californian Rolls “SF” 38 beans, shimeji mushroom, carrot, potato, King crab meat, avocado, tempura crumble fried tofu, peanut sauce and Emping cracker 6 pcs. Giant Rolls “SF” 38 Tempura Vegetables “V” 23 Prawn tempura, cream cheese, avocado, mango, Asparagus, taro, mushroom, lotus root, spicy mayo, teriyaki sauce pumpkin, sweet potato, onion, tempura sauce 12 Slices Sashimi of the Day “GF” 42 Ebi Katsu “SF” 25 Fresh salmon, tuna belly ottoro, yellow tail, Breaded prawn, fruit, katsu sauce local white fish, Hamachi Tofu & Mushroom Spring Roll “VG” 26 6 pcs. Salmon Truffle Rolls “SF” 45 Oyster, eringi, porcini, shitake, shimeji, chili Kabayaki sauce, avocado, Philadelphia cheese, peanut sauce sliced black truffle Raw Salmon Salad 28 1 pc Lobster Sashimi on Ice “GF” “SF” 85 Lemongrass, shallot, coriander, spring onion, Live lobster, daikon radish shuma, wakame, chili, lime, fish sauce, salmon roe fresh -

Product Catalogue Our Gourmet Treats Individuals 4 Are Your Happiness!
PRODUCT CATALOGUE OUR GOURMET TREATS INDIVIDUALS 4 ARE YOUR HAPPINESS! LARGE CAKES 14 FAMILY OWNED EXCELLENCE AND INNOVATION Ribbons and Bows Cakes is a long established and proud Our fully qualified expert pastry chefs and bakers are family owned business with a strong reputation for highly skilled and innovative – always refining production producing the most amazing gourmet cakes and desserts. techniques and products to create the most amazing We have a deep understanding of customer needs and classic and contemporary cakes and desserts. SLICES 23 service, providing an outstanding customer experience. We continue to develop our product range to meet We have established long and successful relationships with the changing needs and lifestyles of our customers. many well known hospitality and food venues reflecting our ongoing commitment to quality, service and value. Our team of highly experienced and talented pastry NUTRITIONAL PRODUCTS TARTS 24 chefs and bakers are very passionate about their craft. We recognise the trend to healthier eating and balanced diets. Accordingly, we continue to refine and expand our range of products so that they not only look good and HANDMADE GOURMET FRESHNESS taste delicious, but also provide nutritional benefits. We specialise in handcrafted and freshly made gourmet We also cater for people with allergies and intolerances so cakes, desserts and pastries. We are unique in the that they too can enjoy our gourmet cakes and desserts. BAKED TREATS 27 market with the creativity, variety, freshness and We offer a selection of products which are flourless and quality of our products. made from Halal ingredients. We can also produce cakes and desserts made from organic ingredients. -
A 1718 Cookbook Contains a Dessert Recipe Similar to the Sachertorte
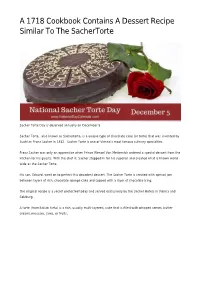
A 1718 Cookbook Contains A Dessert Recipe Similar To The SacherTorte Sacher Torte Day is observed annually on December 5. Sacher Torte, also known as Sachertorte, is a unique type of chocolate cake (or torte) that was invented by Austrian Franz Sacher in 1832. Sacher Torte is one of Vienna’s most famous culinary specialties. Franz Sacher was only an apprentice when Prince Wenzel Von Metternich ordered a special dessert from the kitchen for his guests. With the chef ill, Sacher stepped in for his superior and created what is known world wide as the Sacher Torte. His son, Eduard, went on to perfect this decadent dessert. The Sacher Torte is created with apricot jam between layers of rich, chocolate sponge cake and topped with a layer of chocolate icing. The original recipe is a secret protected today and served exclusively by the Sacher Hotels in Vienna and Salzburg. A torte (from Italian torta) is a rich, usually multi-layered, cake that is filled with whipped cream, butter creams,mousses, jams, or fruits. When comparing tortes and cakes, you will notice that the cake is lighter than the torte. Cakes are made with cake flour alone. Tortes are commonly baked in a spring form pan. The most well-known of the typical tortes include the Austrian Sacher torte. Sacher Torte, a chocolate cake filled with apricot jam and covered with chocolate icing. It was created in Vienna in 1832 by a 16 year old apprentice baker named Franz Sacher for Prince Metternich. Recipes similar to that of the Sacher torte appeared as early as the eighteenth century, one instance being in the 1718 cookbook of Conrad Hagger. -
SPRINGTIME.Compressed.Pdf
Divina Cucina's SWEETS FROM ITALY Judy Witts Francini divinacucina.com divina cucina about me I began my culinary career as a pastry chef at the Stanford Court Hotel in San Francisco. To me, dessert being the last thing you eat at dinner, has to be fabulous or the meal is ruined. I have chosen some of my favorite and simple recipes to end a meal. With Italian recipes, ingredients may vary from where you live, so I always suggest making the recipe once before you serve it for a party. I used grams on some of the recipes where I think it matters. Get a scale! It is worth it for pastry. We use "00" flour which is now available in the USA. Ground almond flour is also more easily available. The ricciarelli are a classic cookie from Siena. The Brutti ma Buoni, vary from town to town. I love the ones made in Prato using walnuts, feel free to use them. Panforte is another dessert from Siena, instead of the richer version with candied fruits, i prefer the simple fig and walnut version. This is perfect served in thin slices with cheese. Salami Dolce is a almost lost recipe, rarely found anymore, except in someone's home. Every Italian mamma has her version of Torta di Mele, this is my version, using tricks from several mamma's i have met. The final dessert is a special chocolate cake from the Island of Capri off the coast of Naples and is also Gluten-free, as are the Ricciarelli and the Fig and Walnut Panforte. -

Intention to Eat Traditional Food Among University Students
International Journal of Academic Research in Business and Social Sciences Vol. 1 1 , No. 13, Beyond 2021 and COVID-19 - New Perspective in the Hospitality & Tourism Industry. 2021, E-ISSN: 2222-6990 © 2021 HRMARS Intention to Eat Traditional Food among University Students Norazlina Rahmat, Mohammad Nuruddin Ramlan, Puteri Nur Athirah Ghazali, Norzaidah Ngali To Link this Article: http://dx.doi.org/10.6007/IJARBSS/v11-i13/8510 DOI:10.6007/IJARBSS/v11-i13/8510 Received: 12 November 2020, Revised: 15 December 2020, Accepted: 31 December 2020 Published Online: 22 January 2021 In-Text Citation: (Rahmat et al., 2021) To Cite this Article: Rahmat, N., Ramlan, M. N., Ghazali, P. N. A., & Ngali, N. (2021). Intention to Eat Traditional Food among University Students. International Journal of Academic Research in Business and Social Sciences, 11(13), 127–138. Copyright: © 2021 The Author(s) Published by Human Resource Management Academic Research Society (www.hrmars.com) This article is published under the Creative Commons Attribution (CC BY 4.0) license. Anyone may reproduce, distribute, translate and create derivative works of this article (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this license may be seen at: http://creativecommons.org/licences/by/4.0/legalcode Special Issue: Beyond 2021 and COVID-19 - New Perspective in the Hospitality & Tourism Industry, 2021, Pg. 127 – 138 http://hrmars.com/index.php/pages/detail/IJARBSS JOURNAL HOMEPAGE Full Terms & Conditions of access and use can be found at http://hrmars.com/index.php/pages/detail/publication-ethics 127 International Journal of Academic Research in Business and Social Sciences Vol. -

Infused Chocolate Molten Mug Cake Recipe FINAL 2
Chocolate Molten Mug Cake About Cozy up and wind down with a mug of warm fluffy chocolate cake surrounding a core of luscious infused molten chocolate. All it takes is a mug and a microwave. Love creamy milk chocolate? You got it. Or maybe you prefer the bitter notes of dark chocolate. It’s your choice. This recipe even allows you to customize your own dosing of THC in the oooey-gooey chocolate lava center. If you prefer an even higher-dosed cake, you can substitute 3 additional squares of Sira Naturals Belgian Chocolate Bar in place of the ½ ounce chopped chocolate in the batter. Be sure to use a mug large enough to hold at least 12 ounces. The Stuff 2 tablespoons unsalted butter 1 pinch salt ½ ounce chopped milk or dark chocolate 2 tablespoons all-purpose flour 2 tablespoons granulated sugar ¼ teaspoon baking soda 1 egg 2-6 squares Sira Naturals Belgian Milk or 1 tablespoon unsweetened cocoa powder Dark Chocolate Bar The Steps Microwave butter and chopped chocolate in microwave-safe bowl or liquid measuring cup at 50 power until just melted, about 1 minute, stirring halfway through cooking. Add sugar, egg, cocoa, and salt and whisk until smooth. Add flour and baking soda and mix until well combined. Transfer batter to coffee mug. Microwave at 50 percent power for 1 minute, stirring halfway through cooking. Submerge squares of Sira Naturals Belgian Chocolate Bar in center of batter. Microwave at 50 percent power for 1 minute. (Cake will look moist on top.) Let rest for 2 minutes and enjoy. -

Csf 35104 Final Year Project 1 Lets Know Malaysian Traditional Foods Ar Semester 1 Session 2019/2020
CSF 35104 FINAL YEAR PROJECT 1 LETS KNOW MALAYSIAN TRADITIONAL FOODS AR SEMESTER 1 SESSION 2019/2020 NAME : AHMAD ZULKHAIRI FAIZ BIN RAZAK MATRIC NUMBER : BTDL 17047800 EMAIL : [email protected] PHONE : 014-2119640 SUPERVISOR : EN. MOHD SUFIAN BIN MAT DERIS ii I DECLARATION I at this moment declare this report based on my original work except for quotations and citations, which have duly acknowledged. I also state that it has not previously or concurrently submitted for any other degree student at University Sultan Zainal Abidin or other institutions. Signature: ___________________ Name : AHMAD ZULKHAIRI FAIZ BIN RAZAK Date : ___________________ ii II CONFIRMATION This project Augmented Reality Malaysia Traditional Food (AR) application was prepared and submitted by Ahmad Zulkhairi Faiz Bin Razak (BTDL 17047800) and has been found satisfactory in terms of scope, quality, and presentation as partial fulfillment of the requirement for the Bachelor of Information Technology (Informatics Media) with honors in University Sultan Zainal Abidin. Signature : _______________ Supervisor : EN. MOHD SUFIAN BIN MAT DERIS Date : _______________ III DEDICATION Firstly and foremost praised to Allah for giving me the opportunity to complete my final year project. Malaysia Traditional Food in AR application using android smartphone forgive me the strength and ability to finish this report. I also would like to express my gratitude to mu supervisor, En Mohd Sufian bin Mat Deris for valuable advice, guidance, and ideas given through the development of research until the end of my final year project. In addition, thanks to my family and my friend that give courage and motivation during my research. IV ABSTRACT Awareness of our society on the value of history traditional food today being at an alarming rate. -

Potensi Dan Peluang Pengembangan Teknologi Pengolahan Melinjo Dalam Mendukung Ketahanan Pangan Di Provinsi Jambi
Linda Yanti POTENSI DAN PELUANG PENGEMBANGAN TEKNOLOGI PENGOLAHAN MELINJO DALAM MENDUKUNG KETAHANAN PANGAN DI PROVINSI JAMBI The Potential and Development Opportunities of Processing Technology of Melinjo in Supporting of Food Security in Jambi Province Linda Yanti Balai Pengkajian Teknologi Pertanian Jambi Jl. Taruna Bumi Panglima Kota Baru Jambi 3600 email : [email protected] ABSTRACT Melinjo (Gnetum gnemon.L) plants is one of the potential commodoties in Jambi province. Part’s of gnetum plants that have a high economic value is melinjo fruit. The nutrient consist of melinjo old fruit is comprised of carbohydrates (63,23%), fats (2,66%), proteins (17,39%) and vitamins. Based on the nutrional content, a wide range of processed products can be made from the melinjo fruit like flakes and crackers. The processing of melinjo products that has penetrated into the export market mainly in chips form that the processing is done traditionally. On the other hand some types of processed products such as chips, sticks and flour (intermediate products) have a good chance to develop industrial scale household and medium industries. Development of technological innovations such melinjo product processing in order to achieve food security by diversifying melinjo refined products is expected to improve the quality, competitiveness and added value and the welfare farmer ultimately. Keywords : melinjo, technology, processing, food security, Jambi ABSTRAK Tanaman melinjo (Gnetum gnemon.L) merupakan salah satu komoditas potensial di provinsi Jambi. Bagian tanaman melinjo yang memiliki nilai ekonomi tinggi adalah buah melinjo. Kandungan gizi buah melinjo tua antara lain terdiri dari karbohidrat (63,23%), lemak (2,66%), protein (17,39%) dan sejumlah vitamin.