Faecal Transplant in Recurrent Clostridium Difficile Infection
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Official Nh Dhhs Health Alert
THIS IS AN OFFICIAL NH DHHS HEALTH ALERT Distributed by the NH Health Alert Network [email protected] May 18, 2018, 1300 EDT (1:00 PM EDT) NH-HAN 20180518 Tickborne Diseases in New Hampshire Key Points and Recommendations: 1. Blacklegged ticks transmit at least five different infections in New Hampshire (NH): Lyme disease, Anaplasma, Babesia, Powassan virus, and Borrelia miyamotoi. 2. NH has one of the highest rates of Lyme disease in the nation, and 50-60% of blacklegged ticks sampled from across NH have been found to be infected with Borrelia burgdorferi, the bacterium that causes Lyme disease. 3. NH has experienced a significant increase in human cases of anaplasmosis, with cases more than doubling from 2016 to 2017. The reason for the increase is unknown at this time. 4. The number of new cases of babesiosis also increased in 2017; because Babesia can be transmitted through blood transfusions in addition to tick bites, providers should ask patients with suspected babesiosis whether they have donated blood or received a blood transfusion. 5. Powassan is a newer tickborne disease which has been identified in three NH residents during past seasons in 2013, 2016 and 2017. While uncommon, Powassan can cause a debilitating neurological illness, so providers should maintain an index of suspicion for patients presenting with an unexplained meningoencephalitis. 6. Borrelia miyamotoi infection usually presents with a nonspecific febrile illness similar to other tickborne diseases like anaplasmosis, and has recently been identified in one NH resident. Tests for Lyme disease do not reliably detect Borrelia miyamotoi, so providers should consider specific testing for Borrelia miyamotoi (see Attachment 1) and other pathogens if testing for Lyme disease is negative but a tickborne disease is still suspected. -

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -

Altered Fecal Microbiota Composition in Patients with Major Depressive Disorder
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector Brain, Behavior, and Immunity 48 (2015) 186–194 Contents lists available at ScienceDirect Brain, Behavior, and Immunity journal homepage: www.elsevier.com/locate/ybrbi Altered fecal microbiota composition in patients with major depressive disorder Haiyin Jiang a,1, Zongxin Ling a,1, Yonghua Zhang b,1, Hongjin Mao c, Zhanping Ma d, Yan Yin c, ⇑ Weihong Wang e, Wenxin Tang c, Zhonglin Tan c, Jianfei Shi c, Lanjuan Li a,2, Bing Ruan a, a Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310003, China b Department of Traditional Chinese Medicine, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China c Department of Psychiatry, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China d Department of Psychiatry, Psychiatric Hospital of Hengshui, Hebei 053000, China e Department of Infectious Diseases, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China article info abstract Article history: Studies using animal models have shown that depression affects the stability of the microbiota, but the Received 29 July 2014 actual structure and composition in patients with major depressive disorder (MDD) are not well under- Received in revised form 29 March 2015 stood. Here, we analyzed fecal samples from 46 patients with depression (29 active-MDD and 17 Accepted 29 March 2015 responded-MDD) and 30 healthy controls (HCs). High-throughput pyrosequencing showed that, accord- Available online 13 April 2015 ing to the Shannon index, increased fecal bacterial a-diversity was found in the active-MDD (A-MDD) vs. -

Naeglaria and Brain Infections
Can bacteria shrink tumors? Cancer Therapy: The Microbial Approach n this age of advanced injected live Streptococcus medical science and into cancer patients but after I technology, we still the recipients unfortunately continue to hunt for died from subsequent innovative cancer therapies infections, Coley decided to that prove effective and safe. use heat killed bacteria. He Treatments that successfully made a mixture of two heat- eradicate tumors while at the killed bacterial species, By Alan Barajas same time cause as little Streptococcus pyogenes and damage as possible to normal Serratia marcescens. This Alani Barajas is a Research and tissue are the ultimate goal, concoction was termed Development Technician at Hardy but are also not easy to find. “Coley’s toxins.” Bacteria Diagnostics. She earned her bachelor's degree in Microbiology at were either injected into Cal Poly, San Luis Obispo. The use of microorganisms in tumors or into the cancer therapy is not a new bloodstream. During her studies at Cal Poly, much idea but it is currently a of her time was spent as part of the undergraduate research team for the buzzing topic in cancer Cal Poly Dairy Products Technology therapy research. Center studying spore-forming bacteria in dairy products. In the late 1800s, German Currently she is working on new physicians W. Busch and F. chromogenic media formulations for Fehleisen both individually Hardy Diagnostics, both in the observed that certain cancers prepared and powdered forms. began to regress when patients acquired accidental erysipelas (cellulitis) caused by Streptococcus pyogenes. William Coley was the first to use New York surgeon William bacterial injections to treat cancer www.HardyDiagnostics.com patients. -

Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis
International Journal of Molecular Sciences Review Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis David Johane Machate 1, Priscila Silva Figueiredo 2 , Gabriela Marcelino 2 , Rita de Cássia Avellaneda Guimarães 2,*, Priscila Aiko Hiane 2 , Danielle Bogo 2, Verônica Assalin Zorgetto Pinheiro 2, Lincoln Carlos Silva de Oliveira 3 and Arnildo Pott 1 1 Graduate Program in Biotechnology and Biodiversity in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] (D.J.M.); [email protected] (A.P.) 2 Graduate Program in Health and Development in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; pri.fi[email protected] (P.S.F.); [email protected] (G.M.); [email protected] (P.A.H.); [email protected] (D.B.); [email protected] (V.A.Z.P.) 3 Chemistry Institute, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] * Correspondence: [email protected]; Tel.: +55-67-3345-7416 Received: 9 March 2020; Accepted: 27 March 2020; Published: 8 June 2020 Abstract: Long-term high-fat dietary intake plays a crucial role in the composition of gut microbiota in animal models and human subjects, which affect directly short-chain fatty acid (SCFA) production and host health. This review aims to highlight the interplay of fatty acid (FA) intake and gut microbiota composition and its interaction with hosts in health promotion and obesity prevention and its related metabolic dysbiosis. -

Diagnostic Code Descriptions (ICD9)
INFECTIONS AND PARASITIC DISEASES INTESTINAL AND INFECTIOUS DISEASES (001 – 009.3) 001 CHOLERA 001.0 DUE TO VIBRIO CHOLERAE 001.1 DUE TO VIBRIO CHOLERAE EL TOR 001.9 UNSPECIFIED 002 TYPHOID AND PARATYPHOID FEVERS 002.0 TYPHOID FEVER 002.1 PARATYPHOID FEVER 'A' 002.2 PARATYPHOID FEVER 'B' 002.3 PARATYPHOID FEVER 'C' 002.9 PARATYPHOID FEVER, UNSPECIFIED 003 OTHER SALMONELLA INFECTIONS 003.0 SALMONELLA GASTROENTERITIS 003.1 SALMONELLA SEPTICAEMIA 003.2 LOCALIZED SALMONELLA INFECTIONS 003.8 OTHER 003.9 UNSPECIFIED 004 SHIGELLOSIS 004.0 SHIGELLA DYSENTERIAE 004.1 SHIGELLA FLEXNERI 004.2 SHIGELLA BOYDII 004.3 SHIGELLA SONNEI 004.8 OTHER 004.9 UNSPECIFIED 005 OTHER FOOD POISONING (BACTERIAL) 005.0 STAPHYLOCOCCAL FOOD POISONING 005.1 BOTULISM 005.2 FOOD POISONING DUE TO CLOSTRIDIUM PERFRINGENS (CL.WELCHII) 005.3 FOOD POISONING DUE TO OTHER CLOSTRIDIA 005.4 FOOD POISONING DUE TO VIBRIO PARAHAEMOLYTICUS 005.8 OTHER BACTERIAL FOOD POISONING 005.9 FOOD POISONING, UNSPECIFIED 006 AMOEBIASIS 006.0 ACUTE AMOEBIC DYSENTERY WITHOUT MENTION OF ABSCESS 006.1 CHRONIC INTESTINAL AMOEBIASIS WITHOUT MENTION OF ABSCESS 006.2 AMOEBIC NONDYSENTERIC COLITIS 006.3 AMOEBIC LIVER ABSCESS 006.4 AMOEBIC LUNG ABSCESS 006.5 AMOEBIC BRAIN ABSCESS 006.6 AMOEBIC SKIN ULCERATION 006.8 AMOEBIC INFECTION OF OTHER SITES 006.9 AMOEBIASIS, UNSPECIFIED 007 OTHER PROTOZOAL INTESTINAL DISEASES 007.0 BALANTIDIASIS 007.1 GIARDIASIS 007.2 COCCIDIOSIS 007.3 INTESTINAL TRICHOMONIASIS 007.8 OTHER PROTOZOAL INTESTINAL DISEASES 007.9 UNSPECIFIED 008 INTESTINAL INFECTIONS DUE TO OTHER ORGANISMS -
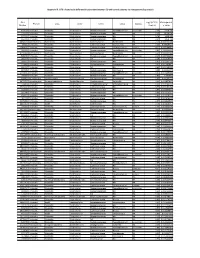
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Microbial Strain-Level Population Structure and Genetic Diversity from Metagenomes
Downloaded from genome.cshlp.org on October 1, 2021 - Published by Cold Spring Harbor Laboratory Press Method Microbial strain-level population structure and genetic diversity from metagenomes Duy Tin Truong,1 Adrian Tett,1 Edoardo Pasolli,1 Curtis Huttenhower,2,3 and Nicola Segata1 1Centre for Integrative Biology, University of Trento, 38123 Trento, Italy; 2Biostatistics Department, Harvard School of Public Health, Boston, Massachusetts 02115, USA; 3The Broad Institute, Cambridge, Massachusetts 02142, USA Among the human health conditions linked to microbial communities, phenotypes are often associated with only a subset of strains within causal microbial groups. Although it has been critical for decades in microbial physiology to characterize individual strains, this has been challenging when using culture-independent high-throughput metagenomics. We introduce StrainPhlAn, a novel metagenomic strain identification approach, and apply it to characterize the genetic structure of thou- sands of strains from more than 125 species in more than 1500 gut metagenomes drawn from populations spanning North and South American, European, Asian, and African countries. The method relies on per-sample dominant sequence variant reconstruction within species-specific marker genes. It identified primarily subject-specific strain variants (<5% inter-subject strain sharing), and we determined that a single strain typically dominated each species and was retained over time (for >70% of species). Microbial population structure was correlated in several distinct ways with the geographic structure of the host population. In some cases, discrete subspecies (e.g., for Eubacterium rectale and Prevotella copri) or continuous mi- crobial genetic variations (e.g., for Faecalibacterium prausnitzii) were associated with geographically distinct human populations, whereas few strains occurred in multiple unrelated cohorts. -

The Human Milk Microbiome and Factors Influencing Its
1 THE HUMAN MILK MICROBIOME AND FACTORS INFLUENCING ITS 2 COMPOSITION AND ACTIVITY 3 4 5 Carlos Gomez-Gallego, Ph. D. ([email protected])1; Izaskun Garcia-Mantrana, Ph. D. 6 ([email protected])2, Seppo Salminen, Prof. Ph. D. ([email protected])1, María Carmen 7 Collado, Ph. D. ([email protected])1,2,* 8 9 1. Functional Foods Forum, Faculty of Medicine, University of Turku, Itäinen Pitkäkatu 4 A, 10 20014, Turku, Finland. Phone: +358 2 333 6821. 11 2. Institute of Agrochemistry and Food Technology, National Research Council (IATA- 12 CSIC), Department of Biotechnology. Valencia, Spain. Phone: +34 96 390 00 22 13 14 15 *To whom correspondence should be addressed. 16 -IATA-CSIC, Av. Agustin Escardino 7, 49860, Paterna, Valencia, Spain. Tel. +34 963900022; 17 E-mail: [email protected] 18 19 20 21 22 23 24 25 26 27 1 1 SUMMARY 2 Beyond its nutritional aspects, human milk contains several bioactive compounds, such as 3 microbes, oligosaccharides, and other substances, which are involved in host-microbe 4 interactions and have a key role in infant health. New techniques have increased our 5 understanding of milk microbiota composition, but little data on the activity of bioactive 6 compounds and their biological role in infants is available. While the human milk microbiome 7 may be influenced by specific factors, including genetics, maternal health and nutrition, mode of 8 delivery, breastfeeding, lactation stage, and geographic location, the impact of these factors on 9 the infant microbiome is not yet known. This article gives an overview of milk microbiota 10 composition and activity, including factors influencing microbial composition and their 11 potential biological relevance on infants' future health. -

Establishment of Listeria Monocytogenes in the Gastrointestinal Tract
microorganisms Review Establishment of Listeria monocytogenes in the Gastrointestinal Tract Morgan L. Davis 1, Steven C. Ricke 1 and Janet R. Donaldson 2,* 1 Center for Food Safety, Department of Food Science, University of Arkansas, Fayetteville, AR 72704, USA; [email protected] (M.L.D.); [email protected] (S.C.R.) 2 Department of Cell and Molecular Biology, The University of Southern Mississippi, Hattiesburg, MS 39406, USA * Correspondence: [email protected]; Tel.: +1-601-266-6795 Received: 5 February 2019; Accepted: 5 March 2019; Published: 10 March 2019 Abstract: Listeria monocytogenes is a Gram positive foodborne pathogen that can colonize the gastrointestinal tract of a number of hosts, including humans. These environments contain numerous stressors such as bile, low oxygen and acidic pH, which may impact the level of colonization and persistence of this organism within the GI tract. The ability of L. monocytogenes to establish infections and colonize the gastrointestinal tract is directly related to its ability to overcome these stressors, which is mediated by the efficient expression of several stress response mechanisms during its passage. This review will focus upon how and when this occurs and how this impacts the outcome of foodborne disease. Keywords: bile; Listeria; oxygen availability; pathogenic potential; gastrointestinal tract 1. Introduction Foodborne pathogens account for nearly 6.5 to 33 million illnesses and 9000 deaths each year in the United States [1]. There are over 40 pathogens that can cause foodborne disease. The six most common foodborne pathogens are Salmonella, Campylobacter jejuni, Escherichia coli O157:H7, Listeria monocytogenes, Staphylococcus aureus, and Clostridium perfringens. -

Molecular Detection of Urogenital Mollicutes in Patients with Invasive Malignant Prostate Tumor Osama Mohammed Saed Abdul-Wahab1, Mishari H
Abdul-Wahab et al. Infectious Agents and Cancer (2021) 16:6 https://doi.org/10.1186/s13027-021-00344-9 RESEARCH ARTICLE Open Access Molecular detection of urogenital mollicutes in patients with invasive malignant prostate tumor Osama Mohammed Saed Abdul-Wahab1, Mishari H. Al-Shyarba2, Boutheina Ben Abdelmoumen Mardassi3, Nessrine Sassi3, Majed Saad Shaya Al Fayi4, Hassan Otifi5, Abdullah Hassan Al Murea6, Béhija Mlik3 and Elhem Yacoub3* Abstract Background: The etiology of prostate cancer (PCa) is multiple and complex. Among the causes recently cited are chronic infections engendered by microorganisms that often go unnoticed. A typical illustration of such a case is infection due to mollicutes bacteria. Generally known by their lurking nature, urogenital mollicutes are the most incriminated in PCa. This study was thus carried out in an attempt to establish the presence of these mollicutes by PCR in biopsies of confirmed PCa patients and to evaluate their prevalence. Methods: A total of 105 Formalin-Fixed Paraffin-Embedded prostate tissues collected from 50 patients suffering from PCa and 55 with benign prostate hyperplasia were subjected to PCR amplification targeting species-specific genes of 5 urogenital mollicutes species, Mycoplasma genitalium, M. hominis, M. fermentans, Ureaplasma parvum, and U. urealyticum. PCR products were then sequenced to confirm species identification. Results significance was statistically assessed using Chi-square and Odds ratio tests. Results: PCR amplification showed no positive results for M. genitalium, M. hominis, and M. fermentans in all tested patients. Strikingly, Ureaplasma spp. were detected among 30% (15/50) of PCa patients. Nucleotide sequencing further confirmed the identified ureaplasma species, which were distributed as follows: 7 individuals with only U. -

Altered Fecal Short-Chain Fatty Acid Concentrations and Dysbiosis In
Received: 9 January 2019 Accepted: 3 May 2019 DOI: 10.1111/jvim.15520 STANDARD ARTICLE Fecal short-chain fatty acid concentrations and dysbiosis in dogs with chronic enteropathy Yasushi Minamoto | Tomomi Minamoto | Anitha Isaiah | Panpicha Sattasathuchana | Agostino Buono | Venkat R. Rangachari | Isaac H. McNeely | Jonathan Lidbury | Jörg M. Steiner | Jan S. Suchodolski Gastrointestinal Laboratory, Department of Small Animal Clinical Sciences, College of Abstract Veterinary Medicine and Biomedical Sciences, Background: Accumulating evidence shows an important relationship between the Texas A&M University, College Station, Texas gastrointestinal (GI) microbiota and host health. Microbial metabolites are believed to Correspondence play a critical role in host-microbial interactions. Short-chain fatty acids (SCFAs) are Jan S. Suchodolski, Gastrointestinal Laboratory, Department of Small Animal major end products of bacterial carbohydrate fermentation in the intestinal tract. Clinical Sciences, College of Veterinary Decreased concentrations of SCFAs have been observed in humans with GI disease. Medicine and Biomedical Sciences, Texas A&M University, 4474 TAMU, College Station, However, large-scale clinical data in dogs are lacking. TX 77843-4474. Hypothesis/Objective: To evaluate fecal concentrations of SCFAs and the fecal Email: [email protected] microbiota in healthy control (HC) dogs and dogs with chronic enteropathy (CE). Animals: Forty-nine privately owned HC dogs and 73 dogs with CE. Methods: Prospective cohort study. Fecal concentrations of SCFAs were measured using gas chromatography/mass spectrometry. Illumina sequencing and quantita- tive real-time polymerase chain reaction were utilized to evaluate the fecal microbiota. Results: Fecal concentrations (median [range] μmol/g of dry matter) of acetate were lower (P = .03) in dogs with CE (185.8 [20.1-1042.1]) than in HC dogs (224.0 [87.7-672.8]).