The Human Milk Microbiome and Factors Influencing Its
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -

Altered Fecal Microbiota Composition in Patients with Major Depressive Disorder
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector Brain, Behavior, and Immunity 48 (2015) 186–194 Contents lists available at ScienceDirect Brain, Behavior, and Immunity journal homepage: www.elsevier.com/locate/ybrbi Altered fecal microbiota composition in patients with major depressive disorder Haiyin Jiang a,1, Zongxin Ling a,1, Yonghua Zhang b,1, Hongjin Mao c, Zhanping Ma d, Yan Yin c, ⇑ Weihong Wang e, Wenxin Tang c, Zhonglin Tan c, Jianfei Shi c, Lanjuan Li a,2, Bing Ruan a, a Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310003, China b Department of Traditional Chinese Medicine, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China c Department of Psychiatry, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China d Department of Psychiatry, Psychiatric Hospital of Hengshui, Hebei 053000, China e Department of Infectious Diseases, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China article info abstract Article history: Studies using animal models have shown that depression affects the stability of the microbiota, but the Received 29 July 2014 actual structure and composition in patients with major depressive disorder (MDD) are not well under- Received in revised form 29 March 2015 stood. Here, we analyzed fecal samples from 46 patients with depression (29 active-MDD and 17 Accepted 29 March 2015 responded-MDD) and 30 healthy controls (HCs). High-throughput pyrosequencing showed that, accord- Available online 13 April 2015 ing to the Shannon index, increased fecal bacterial a-diversity was found in the active-MDD (A-MDD) vs. -

Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis
International Journal of Molecular Sciences Review Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis David Johane Machate 1, Priscila Silva Figueiredo 2 , Gabriela Marcelino 2 , Rita de Cássia Avellaneda Guimarães 2,*, Priscila Aiko Hiane 2 , Danielle Bogo 2, Verônica Assalin Zorgetto Pinheiro 2, Lincoln Carlos Silva de Oliveira 3 and Arnildo Pott 1 1 Graduate Program in Biotechnology and Biodiversity in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] (D.J.M.); [email protected] (A.P.) 2 Graduate Program in Health and Development in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; pri.fi[email protected] (P.S.F.); [email protected] (G.M.); [email protected] (P.A.H.); [email protected] (D.B.); [email protected] (V.A.Z.P.) 3 Chemistry Institute, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] * Correspondence: [email protected]; Tel.: +55-67-3345-7416 Received: 9 March 2020; Accepted: 27 March 2020; Published: 8 June 2020 Abstract: Long-term high-fat dietary intake plays a crucial role in the composition of gut microbiota in animal models and human subjects, which affect directly short-chain fatty acid (SCFA) production and host health. This review aims to highlight the interplay of fatty acid (FA) intake and gut microbiota composition and its interaction with hosts in health promotion and obesity prevention and its related metabolic dysbiosis. -
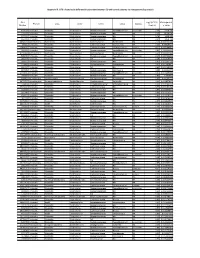
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Changes in the Bacterial Diversity of Human Milk During Late Lactation Period (Weeks 21 to 48)
foods Communication Changes in the Bacterial Diversity of Human Milk during Late Lactation Period (Weeks 21 to 48) Wendy Marin-Gómez ,Ma José Grande, Rubén Pérez-Pulido, Antonio Galvez * and Rosario Lucas Microbiology Division, Department of Health Sciences, Faculty of Experimental Sciences, University of Jaén, 23071 Jaén, Spain; [email protected] (W.M.-G.); [email protected] (M.J.G.); [email protected] (R.P.-P.); [email protected] (R.L.) * Correspondence: [email protected]; Tel.: +34-953-212160 Received: 19 July 2020; Accepted: 25 August 2020; Published: 27 August 2020 Abstract: Breast milk from a single mother was collected during a 28-week lactation period. Bacterial diversity was studied by amplicon sequencing analysis of the V3-V4 variable region of the 16S rRNA gene. Firmicutes and Proteobacteria were the main phyla detected in the milk samples, followed by Actinobacteria and Bacteroidetes. The proportion of Firmicutes to Proteobacteria changed considerably depending on the sampling week. A total of 411 genera or higher taxons were detected in the set of samples. Genus Streptococcus was detected during the 28-week sampling period, at relative abundances between 2.0% and 68.8%, and it was the most abundant group in 14 of the samples. Carnobacterium and Lactobacillus had low relative abundances. At the genus level, bacterial diversity changed considerably at certain weeks within the studied period. The weeks or periods with lowest relative abundance of Streptococcus had more diverse bacterial compositions including genera belonging to Proteobacteria that were poorly represented in the rest of the samples. Keywords: breast milk; biodiversity; lactic acid bacteria; late lactation; metagenomics 1. -

Microbial Strain-Level Population Structure and Genetic Diversity from Metagenomes
Downloaded from genome.cshlp.org on October 1, 2021 - Published by Cold Spring Harbor Laboratory Press Method Microbial strain-level population structure and genetic diversity from metagenomes Duy Tin Truong,1 Adrian Tett,1 Edoardo Pasolli,1 Curtis Huttenhower,2,3 and Nicola Segata1 1Centre for Integrative Biology, University of Trento, 38123 Trento, Italy; 2Biostatistics Department, Harvard School of Public Health, Boston, Massachusetts 02115, USA; 3The Broad Institute, Cambridge, Massachusetts 02142, USA Among the human health conditions linked to microbial communities, phenotypes are often associated with only a subset of strains within causal microbial groups. Although it has been critical for decades in microbial physiology to characterize individual strains, this has been challenging when using culture-independent high-throughput metagenomics. We introduce StrainPhlAn, a novel metagenomic strain identification approach, and apply it to characterize the genetic structure of thou- sands of strains from more than 125 species in more than 1500 gut metagenomes drawn from populations spanning North and South American, European, Asian, and African countries. The method relies on per-sample dominant sequence variant reconstruction within species-specific marker genes. It identified primarily subject-specific strain variants (<5% inter-subject strain sharing), and we determined that a single strain typically dominated each species and was retained over time (for >70% of species). Microbial population structure was correlated in several distinct ways with the geographic structure of the host population. In some cases, discrete subspecies (e.g., for Eubacterium rectale and Prevotella copri) or continuous mi- crobial genetic variations (e.g., for Faecalibacterium prausnitzii) were associated with geographically distinct human populations, whereas few strains occurred in multiple unrelated cohorts. -

Complete Genomic Sequences of Propionibacterium Freudenreichii
UCLA UCLA Previously Published Works Title Complete genomic sequences of Propionibacterium freudenreichii phages from Swiss cheese reveal greater diversity than Cutibacterium (formerly Propionibacterium) acnes phages. Permalink https://escholarship.org/uc/item/7bf0f2q3 Journal BMC microbiology, 18(1) ISSN 1471-2180 Authors Cheng, Lucy Marinelli, Laura J Grosset, Noël et al. Publication Date 2018-03-01 DOI 10.1186/s12866-018-1159-y Peer reviewed eScholarship.org Powered by the California Digital Library University of California Cheng et al. BMC Microbiology (2018) 18:19 https://doi.org/10.1186/s12866-018-1159-y RESEARCH ARTICLE Open Access Complete genomic sequences of Propionibacterium freudenreichii phages from Swiss cheese reveal greater diversity than Cutibacterium (formerly Propionibacterium) acnes phages Lucy Cheng1,2†, Laura J. Marinelli1,2*†, Noël Grosset3, Sorel T. Fitz-Gibbon4, Charles A. Bowman5, Brian Q. Dang5, Daniel A. Russell5, Deborah Jacobs-Sera5, Baochen Shi6, Matteo Pellegrini4, Jeff F. Miller7,2, Michel Gautier3, Graham F. Hatfull5 and Robert L. Modlin1,2 Abstract Background: A remarkable exception to the large genetic diversity often observed for bacteriophages infecting a specific bacterial host was found for the Cutibacterium acnes (formerly Propionibacterium acnes) phages, which are highly homogeneous. Phages infecting the related species, which is also a member of the Propionibacteriaceae family, Propionibacterium freudenreichii, a bacterium used in production of Swiss-type cheeses, have also been described and are common contaminants of the cheese manufacturing process. However, little is known about their genetic composition and diversity. Results: We obtained seven independently isolated bacteriophages that infect P. freudenreichii from Swiss-type cheese samples, and determined their complete genome sequences. -

Product Sheet Info
Product Information Sheet for HM-8 Propionibacterium acidifaciens, Oral Taxon Growth Conditions: 191, Strain F0233 Media: Modified Reinforced Clostridial Broth (ATCC® medium 2107) or equivalent Catalog No. HM-8 Tryptic Soy Agar with 5% defibrinated sheep blood or equivalent For research use only. Not for human use. Incubation: Temperature: 37°C Contributor: Atmosphere: Anaerobic (80% N2:10% CO2:10% H2) Jacques Izard, Assistant Member of the Staff, Department of Propagation: Molecular Genetics, The Forsyth Institute, Boston, 1. Keep vial frozen until ready for use, then thaw. Massachusetts 2. Transfer the entire thawed aliquot into a single tube of broth. Manufacturer: 3. Use several drops of the suspension to inoculate an BEI Resources agar slant and/or plate. 4. Incubate the tube, slant and/or plate at 37°C for 48 to Product Description: 72 hours. Bacteria Classification: Propionibacteriaceae, Propionibacterium Citation: Species: Propionibacterium acidifaciens Acknowledgment for publications should read “The following Subtaxon: Oral Taxon 191 reagent was obtained through BEI Resources, NIAID, NIH as Strain: F0233 part of the Human Microbiome Project: Propionibacterium Original Source: Propionibacterium acidifaciens (P. acidifaciens, Oral Taxon 191, Strain F0233, HM-8.” acidifaciens), Oral Taxon 191, strain F0233 was isolated in March 1983 from the subgingival plaque of a 53-year-old Biosafety Level: 2 black male patient with moderate periodontitis.1,2 Appropriate safety procedures should always be used with Comments: P. acidifaciens, Oral Taxon 191, strain F0233 this material. Laboratory safety is discussed in the following (HMP ID 0682) is a reference genome for The Human publication: U.S. Department of Health and Human Microbiome Project (HMP). -

Breast Milk Microbiota: a Review of the Factors That Influence Composition
Published in "Journal of Infection 81(1): 17–47, 2020" which should be cited to refer to this work. ✩ Breast milk microbiota: A review of the factors that influence composition ∗ Petra Zimmermann a,b,c,d, , Nigel Curtis b,c,d a Department of Paediatrics, Fribourg Hospital HFR and Faculty of Science and Medicine, University of Fribourg, Switzerland b Department of Paediatrics, The University of Melbourne, Parkville, Australia c Infectious Diseases Research Group, Murdoch Children’s Research Institute, Parkville, Australia d Infectious Diseases Unit, The Royal Children’s Hospital Melbourne, Parkville, Australia s u m m a r y Breastfeeding is associated with considerable health benefits for infants. Aside from essential nutrients, immune cells and bioactive components, breast milk also contains a diverse range of microbes, which are important for maintaining mammary and infant health. In this review, we summarise studies that have Keywords: investigated the composition of the breast milk microbiota and factors that might influence it. Microbiome We identified 44 studies investigating 3105 breast milk samples from 2655 women. Several studies Diversity reported that the bacterial diversity is higher in breast milk than infant or maternal faeces. The maxi- Delivery mum number of each bacterial taxonomic level detected per study was 58 phyla, 133 classes, 263 orders, Caesarean 596 families, 590 genera, 1300 species and 3563 operational taxonomic units. Furthermore, fungal, ar- GBS chaeal, eukaryotic and viral DNA was also detected. The most frequently found genera were Staphylococ- Antibiotics cus, Streptococcus Lactobacillus, Pseudomonas, Bifidobacterium, Corynebacterium, Enterococcus, Acinetobacter, BMI Rothia, Cutibacterium, Veillonella and Bacteroides. There was some evidence that gestational age, delivery Probiotics mode, biological sex, parity, intrapartum antibiotics, lactation stage, diet, BMI, composition of breast milk, Smoking Diet HIV infection, geographic location and collection/feeding method influence the composition of the breast milk microbiota. -

Characterization of Weissella Koreensis SK Isolated From
microorganisms Article Characterization of Weissella koreensis SK Isolated from Kimchi Fermented at Low Temperature ◦ (around 0 C) Based on Complete Genome Sequence and Corresponding Phenotype So Yeong Mun and Hae Choon Chang * Department of Food and Nutrition, Kimchi Research Center, Chosun University, 309 Pilmun-daero, Dong-gu, Gwangju 61452, Korea; [email protected] * Correspondence: [email protected] Received: 17 June 2020; Accepted: 28 July 2020; Published: 29 July 2020 Abstract: This study identified lactic acid bacteria (LAB) that play a major role in kimchi fermented at low temperature, and investigated the safety and functionality of the LAB via biologic and genomic analyses for its potential use as a starter culture or probiotic. Fifty LAB were isolated from 45 kimchi samples fermented at 1.5~0 C for 2~3 months. Weissella koreensis strains were determined as the − ◦ dominant LAB in all kimchi samples. One strain, W. koreensis SK, was selected and its phenotypic and genomic features characterized. The complete genome of W. koreensis SK contains one circular chromosome and plasmid. W. koreensis SK grew well under mesophilic and psychrophilic conditions. W. koreensis SK was found to ferment several carbohydrates and utilize an alternative carbon source, the amino acid arginine, to obtain energy. Supplementation with arginine improved cell growth and resulted in high production of ornithine. The arginine deiminase pathway of W. koreensis SK was encoded in a cluster of four genes (arcA-arcB-arcD-arcC). No virulence traits were identified in the genomic and phenotypic analyses. The results indicate that W. koreensis SK may be a promising starter culture for fermented vegetables or fruits at low temperature as well as a probiotic candidate. -

Levels of Firmicutes, Actinobacteria Phyla and Lactobacillaceae
agriculture Article Levels of Firmicutes, Actinobacteria Phyla and Lactobacillaceae Family on the Skin Surface of Broiler Chickens (Ross 308) Depending on the Nutritional Supplement and the Housing Conditions Paulina Cholewi ´nska 1,* , Marta Michalak 2, Konrad Wojnarowski 1 , Szymon Skowera 1, Jakub Smoli ´nski 1 and Katarzyna Czyz˙ 1 1 Institute of Animal Breeding, Wroclaw University of Environmental and Life Sciences, 51-630 Wroclaw, Poland; [email protected] (K.W.); [email protected] (S.S.); [email protected] (J.S.); [email protected] (K.C.) 2 Department of Animal Nutrition and Feed Management, Wroclaw University of Environmental and Life Sciences, 51-630 Wroclaw, Poland; [email protected] * Correspondence: [email protected] Abstract: The microbiome of animals, both in the digestive tract and in the skin, plays an important role in protecting the host. The skin is one of the largest surface organs for animals; therefore, the destabilization of the microbiota on its surface can increase the risk of diseases that may adversely af- fect animals’ health and production rates, including poultry. The aim of this study was to evaluate the Citation: Cholewi´nska,P.; Michalak, effect of nutritional supplementation in the form of fermented rapeseed meal and housing conditions M.; Wojnarowski, K.; Skowera, S.; on the level of selected bacteria phyla (Firmicutes, Actinobacteria, and family Lactobacillaceae). The Smoli´nski,J.; Czyz,˙ K. Levels of study was performed on 30 specimens of broiler chickens (Ross 308), individually kept in metabolic Firmicutes, Actinobacteria Phyla and cages for 36 days. They were divided into 5 groups depending on the feed received. -

Food Microbial Ecology - Eugenia Bezirtzoglou
MEDICAL SCIENCES - Food Microbial Ecology - Eugenia Bezirtzoglou FOOD MICROBIAL ECOLOGY Eugenia Bezirtzoglou, Democritus University of Thrace, Faculty of Agricultural Development, Department of Food Science and Technology, Laboratory of Microbiology, Biotechnology and Hygiene and Laboratory of food Processing, Orestiada, Greece Keywords: Food, Microbial Ecology Contents 1. Scope of Microbial Ecology 2. Food Microbial Ecosystem 3. Diversity of Habitat 4. Factors influencing the Growth and Survival of Microorganisms in Foods 5. Food Spoilage and its Microbiology 6. Fermented and Microbial Foods 7. Conclusions Related Chapters Glossary Bibliography Biographical Sketch Summary Microbial ecology is the study of microorganisms in their proper environment and their interactions with it. Microbial ecology can give us answers about our origin, our place in the earth ecosystem as well as on our connection to the great diversity of all other organisms. In this vein, studying microbial ecology questions should help to explain the role of microbes in the environment, in food production, in bioengineering and chemicals items and as result will improve our lives. There is a plethora of microorganisms on our planet, most microorganisms remain unknown. It is estimated that we have knowledge only of 1% of the microbial species on Earth. Multiple studies in intestinal ecology have been greatly hampered by the inaccuracy and limitations of culture methods. Many bacteria are difficult to culture or are unculturable, and often media are not truly specific or are too selective for certain bacteria. Furthermore it is impossible to study and compare complete ecosystems, as they exist in the human body, by culturing methods. Molecular tools introduced in microbial ecology made it possible to study the composition of the microecosystems in a different way, which is not dependent on culture techniques.