Gut Microbiota Composition Reflects Disease Severity and Dysfunctional
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -

The Gut Microbiota and Inflammation
International Journal of Environmental Research and Public Health Review The Gut Microbiota and Inflammation: An Overview 1, 2 1, 1, , Zahraa Al Bander *, Marloes Dekker Nitert , Aya Mousa y and Negar Naderpoor * y 1 Monash Centre for Health Research and Implementation, School of Public Health and Preventive Medicine, Monash University, Melbourne 3168, Australia; [email protected] 2 School of Chemistry and Molecular Biosciences, The University of Queensland, Brisbane 4072, Australia; [email protected] * Correspondence: [email protected] (Z.A.B.); [email protected] (N.N.); Tel.: +61-38-572-2896 (N.N.) These authors contributed equally to this work. y Received: 10 September 2020; Accepted: 15 October 2020; Published: 19 October 2020 Abstract: The gut microbiota encompasses a diverse community of bacteria that carry out various functions influencing the overall health of the host. These comprise nutrient metabolism, immune system regulation and natural defence against infection. The presence of certain bacteria is associated with inflammatory molecules that may bring about inflammation in various body tissues. Inflammation underlies many chronic multisystem conditions including obesity, atherosclerosis, type 2 diabetes mellitus and inflammatory bowel disease. Inflammation may be triggered by structural components of the bacteria which can result in a cascade of inflammatory pathways involving interleukins and other cytokines. Similarly, by-products of metabolic processes in bacteria, including some short-chain fatty acids, can play a role in inhibiting inflammatory processes. In this review, we aimed to provide an overview of the relationship between the gut microbiota and inflammatory molecules and to highlight relevant knowledge gaps in this field. -

Gut Health in Veterinary Medicine: a Bibliometric Analysis of the Literature
animals Article Gut Health in Veterinary Medicine: A Bibliometric Analysis of the Literature Elena Colombino 1,*,† , Daniel Prieto-Botella 2,† and Maria Teresa Capucchio 1 1 Department of Veterinary Sciences, University of Turin, 10095 Grugliasco, Italy; [email protected] 2 Department of Surgery and Pathology, Miguel Hernandez University, 03550 Alicante, Spain; [email protected] * Correspondence: [email protected] † Equally contribution. Simple Summary: Gut health has been a main topic in veterinary medicine research after the ban on the use of antimicrobial growth promoters. Gut health has been defined as absence/prevention/avoidance of gastrointestinal disease so that the animal is able to perform its physiological functions. A biblio- metric analysis is a set of statistical methods used to explore trends in the scientific literature such as number of publications, most prolific countries and main research areas to highlight publication dynamics and gaps of knowledge. In this case, a bibliometric analysis was performed on veterinary gut health using the database Web of Science and the R package Bibliometrix. A total of 1696 docu- ments were retrieved between 2000 and 2020, showing an increase of 22.4% in the number of annual publications. Pigs (34.8%), poultry (chicken, duck, turkey and quail—33.9%) and aquaculture (fishes, crustaceans and frog—15.0%) were the most studied species while a scarce number of publications was found on felines, cows, horses, rodents, goats and sheep. China (24.7%), USA (17.2%) and Canada (5.7%) were the most productive countries. Three main research lines aimed to explore animal nutrition, prevention of inflammatory diseases and microbiota composition were identified. -

Altered Fecal Microbiota Composition in Patients with Major Depressive Disorder
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector Brain, Behavior, and Immunity 48 (2015) 186–194 Contents lists available at ScienceDirect Brain, Behavior, and Immunity journal homepage: www.elsevier.com/locate/ybrbi Altered fecal microbiota composition in patients with major depressive disorder Haiyin Jiang a,1, Zongxin Ling a,1, Yonghua Zhang b,1, Hongjin Mao c, Zhanping Ma d, Yan Yin c, ⇑ Weihong Wang e, Wenxin Tang c, Zhonglin Tan c, Jianfei Shi c, Lanjuan Li a,2, Bing Ruan a, a Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310003, China b Department of Traditional Chinese Medicine, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China c Department of Psychiatry, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China d Department of Psychiatry, Psychiatric Hospital of Hengshui, Hebei 053000, China e Department of Infectious Diseases, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China article info abstract Article history: Studies using animal models have shown that depression affects the stability of the microbiota, but the Received 29 July 2014 actual structure and composition in patients with major depressive disorder (MDD) are not well under- Received in revised form 29 March 2015 stood. Here, we analyzed fecal samples from 46 patients with depression (29 active-MDD and 17 Accepted 29 March 2015 responded-MDD) and 30 healthy controls (HCs). High-throughput pyrosequencing showed that, accord- Available online 13 April 2015 ing to the Shannon index, increased fecal bacterial a-diversity was found in the active-MDD (A-MDD) vs. -

Identification of Species Belonging to the Bifidobacterium Genus by PCR
Baffoni et al. BMC Microbiology 2013, 13:149 http://www.biomedcentral.com/1471-2180/13/149 METHODOLOGY ARTICLE Open Access Identification of species belonging to the Bifidobacterium genus by PCR-RFLP analysis of a hsp60 gene fragment Loredana Baffoni1*, Verena Stenico1, Erwin Strahsburger2, Francesca Gaggìa1, Diana Di Gioia1, Monica Modesto1, Paola Mattarelli1 and Bruno Biavati1 Abstract Background: Bifidobacterium represents one of the largest genus within the Actinobacteria, and includes at present 32 species. These species share a high sequence homology of 16S rDNA and several molecular techniques already applied to discriminate among them give ambiguous results. The slightly higher variability of the hsp60 gene sequences with respect to the 16S rRNA sequences offers better opportunities to design or develop molecular assays, allowing identification and differentiation of closely related species. hsp60 can be considered an excellent additional marker for inferring the taxonomy of the members of Bifidobacterium genus. Results: This work illustrates a simple and cheap molecular tool for the identification of Bifidobacterium species. The hsp60 universal primers were used in a simple PCR procedure for the direct amplification of 590 bp of the hsp60 sequence. The in silico restriction analysis of bifidobacterial hsp60 partial sequences allowed the identification of a single endonuclease (HaeIII) able to provide different PCR-restriction fragment length polymorphism (RFLP) patterns in the Bifidobacterium spp. type strains evaluated. The electrophoretic analyses allowed to confirm the different RFLP patterns. Conclusions: The developed PCR-RFLP technique resulted in efficient discrimination of the tested species and subspecies and allowed the construction of a dichotomous key in order to differentiate the most widely distributed Bifidobacterium species as well as the subspecies belonging to B. -

The Oral Microbiome of Healthy Japanese People at the Age of 90
applied sciences Article The Oral Microbiome of Healthy Japanese People at the Age of 90 Yoshiaki Nomura 1,* , Erika Kakuta 2, Noboru Kaneko 3, Kaname Nohno 3, Akihiro Yoshihara 4 and Nobuhiro Hanada 1 1 Department of Translational Research, Tsurumi University School of Dental Medicine, Kanagawa 230-8501, Japan; [email protected] 2 Department of Oral bacteriology, Tsurumi University School of Dental Medicine, Kanagawa 230-8501, Japan; [email protected] 3 Division of Preventive Dentistry, Faculty of Dentistry and Graduate School of Medical and Dental Science, Niigata University, Niigata 951-8514, Japan; [email protected] (N.K.); [email protected] (K.N.) 4 Division of Oral Science for Health Promotion, Faculty of Dentistry and Graduate School of Medical and Dental Science, Niigata University, Niigata 951-8514, Japan; [email protected] * Correspondence: [email protected]; Tel.: +81-45-580-8462 Received: 19 August 2020; Accepted: 15 September 2020; Published: 16 September 2020 Abstract: For a healthy oral cavity, maintaining a healthy microbiome is essential. However, data on healthy microbiomes are not sufficient. To determine the nature of the core microbiome, the oral-microbiome structure was analyzed using pyrosequencing data. Saliva samples were obtained from healthy 90-year-old participants who attended the 20-year follow-up Niigata cohort study. A total of 85 people participated in the health checkups. The study population consisted of 40 male and 45 female participants. Stimulated saliva samples were obtained by chewing paraffin wax for 5 min. The V3–V4 hypervariable regions of the 16S ribosomal RNA (rRNA) gene were amplified by PCR. -

Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis
International Journal of Molecular Sciences Review Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis David Johane Machate 1, Priscila Silva Figueiredo 2 , Gabriela Marcelino 2 , Rita de Cássia Avellaneda Guimarães 2,*, Priscila Aiko Hiane 2 , Danielle Bogo 2, Verônica Assalin Zorgetto Pinheiro 2, Lincoln Carlos Silva de Oliveira 3 and Arnildo Pott 1 1 Graduate Program in Biotechnology and Biodiversity in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] (D.J.M.); [email protected] (A.P.) 2 Graduate Program in Health and Development in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; pri.fi[email protected] (P.S.F.); [email protected] (G.M.); [email protected] (P.A.H.); [email protected] (D.B.); [email protected] (V.A.Z.P.) 3 Chemistry Institute, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] * Correspondence: [email protected]; Tel.: +55-67-3345-7416 Received: 9 March 2020; Accepted: 27 March 2020; Published: 8 June 2020 Abstract: Long-term high-fat dietary intake plays a crucial role in the composition of gut microbiota in animal models and human subjects, which affect directly short-chain fatty acid (SCFA) production and host health. This review aims to highlight the interplay of fatty acid (FA) intake and gut microbiota composition and its interaction with hosts in health promotion and obesity prevention and its related metabolic dysbiosis. -
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
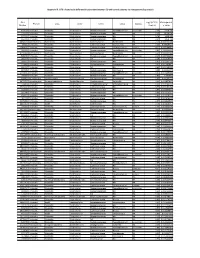
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Changes in the Bacterial Diversity of Human Milk During Late Lactation Period (Weeks 21 to 48)
foods Communication Changes in the Bacterial Diversity of Human Milk during Late Lactation Period (Weeks 21 to 48) Wendy Marin-Gómez ,Ma José Grande, Rubén Pérez-Pulido, Antonio Galvez * and Rosario Lucas Microbiology Division, Department of Health Sciences, Faculty of Experimental Sciences, University of Jaén, 23071 Jaén, Spain; [email protected] (W.M.-G.); [email protected] (M.J.G.); [email protected] (R.P.-P.); [email protected] (R.L.) * Correspondence: [email protected]; Tel.: +34-953-212160 Received: 19 July 2020; Accepted: 25 August 2020; Published: 27 August 2020 Abstract: Breast milk from a single mother was collected during a 28-week lactation period. Bacterial diversity was studied by amplicon sequencing analysis of the V3-V4 variable region of the 16S rRNA gene. Firmicutes and Proteobacteria were the main phyla detected in the milk samples, followed by Actinobacteria and Bacteroidetes. The proportion of Firmicutes to Proteobacteria changed considerably depending on the sampling week. A total of 411 genera or higher taxons were detected in the set of samples. Genus Streptococcus was detected during the 28-week sampling period, at relative abundances between 2.0% and 68.8%, and it was the most abundant group in 14 of the samples. Carnobacterium and Lactobacillus had low relative abundances. At the genus level, bacterial diversity changed considerably at certain weeks within the studied period. The weeks or periods with lowest relative abundance of Streptococcus had more diverse bacterial compositions including genera belonging to Proteobacteria that were poorly represented in the rest of the samples. Keywords: breast milk; biodiversity; lactic acid bacteria; late lactation; metagenomics 1. -

British Society of Gastroenterology Guidelines on the Gut: First Published As 10.1136/Gutjnl-2021-324598 on 26 April 2021
Guidelines British Society of Gastroenterology guidelines on the Gut: first published as 10.1136/gutjnl-2021-324598 on 26 April 2021. Downloaded from management of irritable bowel syndrome Dipesh H Vasant ,1,2 Peter A Paine,2,3 Christopher J Black ,4,5 Lesley A Houghton ,5,6 Hazel A Everitt,7 Maura Corsetti,8 Anurag Agrawal,9 Imran Aziz ,10,11 Adam D Farmer,12,13 Maria P Eugenicos,14 Rona Moss- Morris,15 Yan Yiannakou,16 Alexander C Ford 4,5 ► Additional supplemental ABSTRACT (abdominal pain or discomfort, in association material is published online Irritable bowel syndrome (IBS) remains one of the most with altered bowel habit, for at least 6 months, only. To view, please visit the journal online (http:// dx. doi. org/ common gastrointestinal disorders seen by clinicians in in the absence of alarm symptoms or signs) is 10. 1136/ gutjnl- 2021- 324598). both primary and secondary care. Since publication of the more pragmatic and may be more applicable to last British Society of Gastroenterology (BSG) guideline patients with IBS in primary care than diagnostic For numbered affiliations see end of article. in 2007, substantial advances have been made in criteria derived from patients in secondary care, understanding its complex pathophysiology, resulting in such as the Rome IV criteria (recommendation: Correspondence to its re- classification as a disorder of gut- brain interaction, weak, quality of evidence: low). Professor Alexander C Ford, rather than a functional gastrointestinal disorder. ► All patients presenting with symptoms of IBS Leeds Gastroenterology Moreover, there has been a considerable amount of for the first time in primary care should have Institute, St James’s University new evidence published concerning the diagnosis, a full blood count, C reactive protein or eryth- Hospital, Leeds, UK; alexf12399@ yahoo. -

775 Sixth International Conference on Webometrics, Informetrics And
Sixth International Conference on Webometrics, Informetrics and Scientometrics & Eleventh COLLNET Meeting, October 19 – 22, 2010, University of Mysore, ALGORITHMIC GENERATION OF SPECIALTY PROFILES FOR MEDICAL JOURNALS Pudovkin A.I Institute of Marine Biology, Vladivostok 690041, Russia; e-mail: [email protected] E. Garfield ThomsonReuters Scientific, 1500 Spring Garden Street, Philadelphia, PA 19130-4067, e-mail: [email protected] Abstract A procedure for generating a topical profile of a medical journal is proposed. The procedure consists in calculating of the relatedness index Rgeom of a target journal with all 50 JCR medical categories and identification of top-related ones. The set of highly related categories (3 or 5) may be regarded as the specialty profile of the target journal. We illustrate the method by considering the content of 7 medical journals, 6 specialized ones and a leading multi-scope journal: Annals of Surgery, Circulation, Clinical Infectious diseases, European Heart Journal, Gut, Shock, and New England Journal of Medicine. The data for our analyses are taken from the 2006 and 2009 JCR Science Edition ―Related Journals‖ listings for each medical category. It is shown that the resulting specialty profiles are quite stable in time and well correspond to JCR‘s assignment of journals to subject categories. JCR‘s category assignment is a heuristic procedure performed by an expert, while our procedure is comletely algorithmic. KeyWords: journal topical specification; medical journals; JCR; Journal Relatedness Indexes Introduction The problem of classification, that is, specialty characterization of journals is an old and difficult one (Katz and Hicks, 1995; Boyack et al., 2005; Klavans and Boyack, 2006; Leydesdorff, 2006; Zhang et al., 2010a, b). -

Targeting the Microbiota-Gut-Brain Axis
Author’s Accepted Manuscript Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice“Prebiotics for Stress-Related Disorders” Aurelijus Burokas, Silvia Arboleya, Rachel D. Moloney, Veronica L. Peterson, Kiera Murphy, Gerard Clarke, Catherine Stanton, Timothy G. www.elsevier.com/locate/journal Dinan, John F. Cryan PII: S0006-3223(17)30042-2 DOI: http://dx.doi.org/10.1016/j.biopsych.2016.12.031 Reference: BPS13098 To appear in: Biological Psychiatry Cite this article as: Aurelijus Burokas, Silvia Arboleya, Rachel D. Moloney, Veronica L. Peterson, Kiera Murphy, Gerard Clarke, Catherine Stanton, Timothy G. Dinan and John F. Cryan, Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice“Prebiotics for Stress-Related Disorders”, Biological Psychiatry, http://dx.doi.org/10.1016/j.biopsych.2016.12.031 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting galley proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice Aurelijus Burokas1, Silvia Arboleya1,2*, Rachel D. Moloney1*, Veronica L.