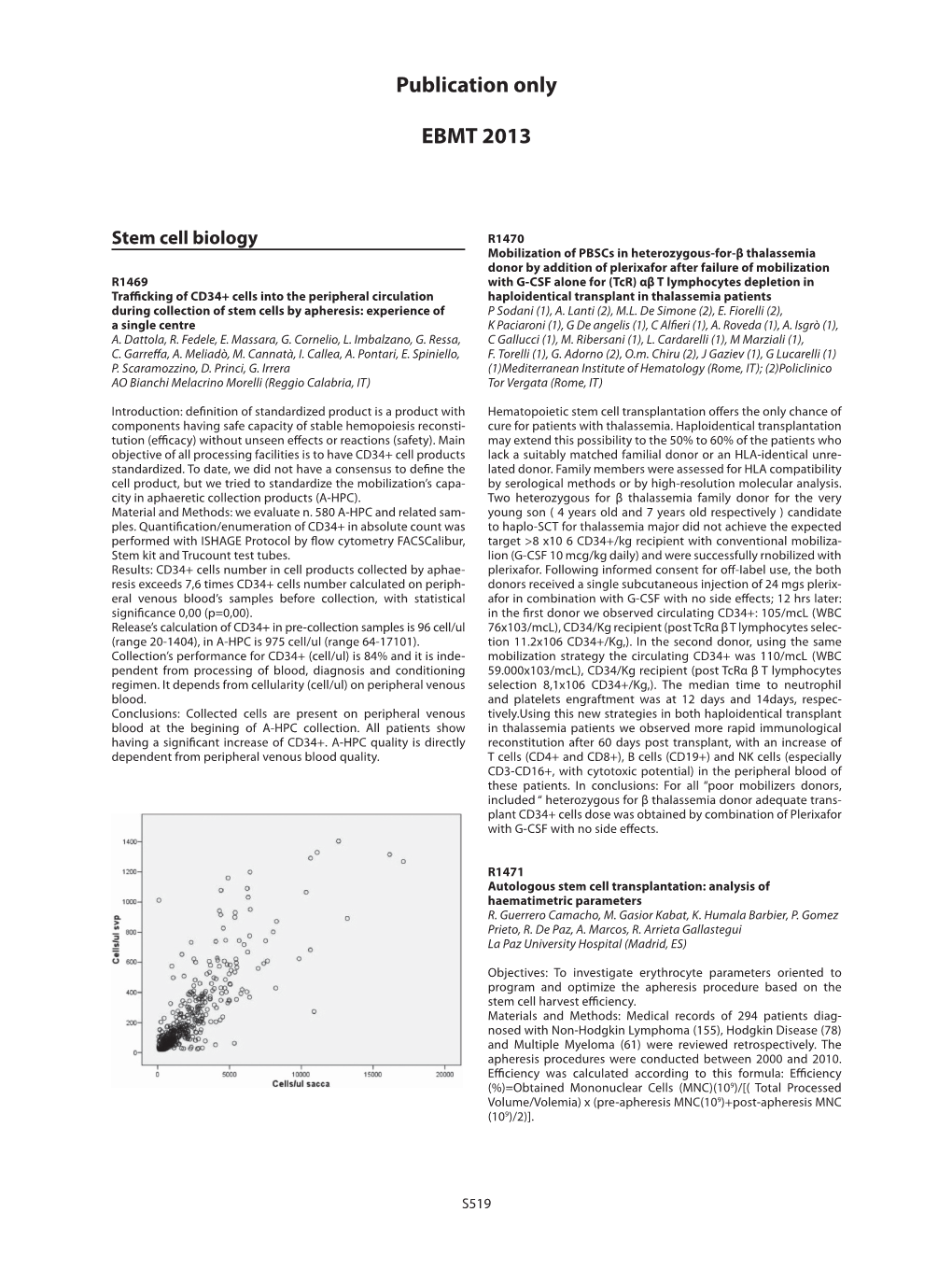
Publication Only
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Therapeutic Class Overview Colony Stimulating Factors
Therapeutic Class Overview Colony Stimulating Factors Therapeutic Class Overview/Summary: This review will focus on the granulocyte colony stimulating factors (G-CSFs) and granulocyte- macrophage colony stimulating factors (GM-CSFs).1-5 Colony-stimulating factors (CSFs) fall under the naturally occurring glycoprotein cytokines, one of the main groups of immunomodulators.6 In general, these proteins are vital to the proliferation and differentiation of hematopoietic progenitor cells.6-8 The G- CSFs commercially available in the United States include pegfilgrastim (Neulasta®), filgrastim (Neupogen®), filgrastim-sndz (Zarxio®), and tbo-filgrastim (Granix®). While filgrastim-sndz and tbo- filgrastim are the same recombinant human G-CSF as filgrastim, only filgrastim-sndz is considered a biosimilar drug as it was approved through the biosimilar pathway. At the time tbo-filgrastim was approved, a regulatory pathway for biosimilar drugs had not yet been established in the United States and tbo-filgrastim was filed under its own Biologic License Application.9 Only one GM-CSF is currently available, sargramostim (Leukine). These agents are Food and Drug Administration (FDA)-approved for a variety of conditions relating to neutropenia or for the collection of hematopoietic progenitor cells for collection by leukapheresis.1-5 Due to the pathway taken, tbo-filgrastim does not share all of the same indications as filgrastim and these two products are not interchangeable. It is important to note that although filgrastim-sndz is a biosimilar product, and it was approved with all the same indications as filgrastim at the time, filgrastim has since received FDA-approval for an additional indication that filgrastim-sndz does not have, to increase survival in patients with acute exposure to myelosuppressive doses of radiation.1-3A complete list of indications for each agent can be found in Table 1. -

Comparison Between Filgrastim and Lenograstim Plus Chemotherapy For
Bone Marrow Transplantation (2010) 45, 277–281 & 2010 Macmillan Publishers Limited All rights reserved 0268-3369/10 $32.00 www.nature.com/bmt ORIGINAL ARTICLE Comparison between filgrastim and lenograstim plus chemotherapy for mobilization of PBPCs R Ria, T Gasparre, G Mangialardi, A Bruno, G Iodice, A Vacca and F Dammacco Department of Biomedical Sciences and Human Oncology, Section of Internal Medicine and Clinical Oncology, University of Bari Medical School, Bari, Italy Recombinant human (rHu) G-CSF has been widely used during transplantation.4 However, the use of G-CSF after to treat neutropenia and mobilize PBPCs for their autologous PBPC transplantation has been queried, as its autologous and allogeneic transplantation. It shortens further reduction in time to a safe neutrophil count5,6 does neutropenia and thus reduces the frequency of neutropenic not always imply fewer significant clinical events, such as fever. We compared the efficiency of glycosylated rHu infections, length of hospitalization, extrahematological and non-glycosylated Hu G-CSF in mobilizing hemato- toxicities or mortality.7,8 Even so, the ASCO guidelines still poietic progenitor cells (HPCs). In total, 86 patients were recommend the use of growth factors after autologous consecutively enrolled for mobilization with CY plus either PBPC transplantation.9 glycosylated or non-glycosylated G-CSF, and under- G-CSF induces the proliferation and differentiation of went leukapheresis. The HPC content of each collection, myeloid precursor cells, and also provides a functional toxicity, days of leukapheresis needed to reach the activity that influences chemotaxis, respiratory burst and minimum HPC target and days to recover WBC (X500 Ag expression of neutrophils. -

Human G-CSF ELISA Kit (ARG80143)
Product datasheet [email protected] ARG80143 Package: 96 wells Human G-CSF ELISA Kit Store at: 4°C Component Cat. No. Component Name Package Temp ARG80143-001 Antibody-coated 8 X 12 strips 4°C. Unused strips microplate should be sealed tightly in the air-tight pouch. ARG80143-002 Standard 3 X 2 ng/vial 4°C (Lyophilized) ARG80143-003 Standard diluent 20 ml 4°C buffer ARG80143-004 Antibody conjugate 400 µl 4°C concentrate ARG80143-005 Antibody diluent 16 ml 4°C buffer ARG80143-006 HRP-Streptavidin 400 µl 4°C (Protect from concentrate light) ARG80143-007 HRP-Streptavidin 16 ml 4°C diluent buffer ARG80143-008 20X Wash buffer 50 ml 4°C ARG80143-009 TMB substrate 12ml 4°C (Protect from light) ARG80143-010 STOP solution 12ml 4°C ARG80143-011 Plate sealer 4 strips Room temperature Summary Product Description ARG80143 Human G-CSF ELISA Kit is an Enzyme Immunoassay kit for the quantification of Human G-CSF in Serum, Plasma, Cell culture supernatants. Tested Reactivity Hu Tested Application ELISA Specificity No significant cross-reactivity or interference with Human CT-1,IL-11,OSM,CNTF,HGF,M-CSF;mouse IL-6;rat IL-6,CNTF Target Name G-CSF Conjugation HRP Conjugation Note Substrate: TMB and read at 450 nm Sensitivity 15 pg/ml Sample Type Serum, Plasma, Cell culture supernatants Standard Range 31.25 - 2000 pg/ml www.arigobio.com 1/3 Sample Volume 100 µl Precision CV: Alternate Names Granulocyte colony-stimulating factor; Lenograstim; C17orf33; GCSF; G-CSF; Filgrastim; Pluripoietin; CSF3OS Application Instructions Assay Time 4 hours Properties Form 96 well Storage instruction Store the kit at 2-8°C. -

Hematopoietic Growth Factors Version 2.2019 — March 27, 2019
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Hematopoietic Growth Factors Version 2.2019 — March 27, 2019 NCCN.org Continue Version 2.2019, 03/27/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN. NCCN Guidelines Index NCCN Guidelines Version 2.2019 Table of Contents Hematopoietic Growth Factors Discussion *Pamela Sue Becker, MD/PhD/Chair ‡ Þ ξ Dwight D. Kloth, PharmD, BCOP ∑ Vivek Roy, MD ‡ Fred Hutchinson Cancer Research Center/ Fox Chase Cancer Center Mayo Clinic Cancer Center Seattle Cancer Care Alliance Eric H. Kraut, MD ‡ Hope S. Rugo, MD † ‡ * Elizabeth A. Griffiths, MD/Vice Chair ‡ Þ † The Ohio State University Comprehensive UCSF Helen Diller Family Roswell Park Comprehensive Cancer Center Cancer Center - James Cancer Hospital Comprehensive Cancer Center and Solove Research Institute Laura Alwan, PharmD ∑ Sepideh Shayani, PharmD ∑ ‡ Fred Hutchinson Cancer Research Center/ Gary H. Lyman, MD, MPH † ‡ City of Hope National Medical Center Seattle Cancer Care Alliance Fred Hutchinson Cancer Research Center/ Saroj Vadhan-Raj, MD † Þ Kimo Bachiashvili, MD ‡ Seattle Cancer Care Alliance The University of Texas University of Alabama at Birmingham MD Anderson Cancer Center Comprehensive Cancer Center Mary Mably, RPh, BCOP ∑ ‡ University of Wisconsin Sumithira Vasu, MBBS ‡ Mona Benrashid, PharmD ∑ Carbone Cancer Center The Ohio State University Comprehensive Vanderbilt-Ingram -

Role of HMOX1 Promoter Genetic Variants in Chemoresistance and Chemotherapy Induced Neutropenia in Children with Acute Lymphoblastic Leukemia
International Journal of Molecular Sciences Article Role of HMOX1 Promoter Genetic Variants in Chemoresistance and Chemotherapy Induced Neutropenia in Children with Acute Lymphoblastic Leukemia Karolina Bukowska-Strakova 1,* , Joanna Włodek 1, Ewelina Pitera 1 , Magdalena Kozakowska 2, Anna Konturek-Cie´sla 2, Maciej Cie´sla 2, Monika Go ´nka 2, Witold Nowak 2 , Aleksandra Wieczorek 3 , Katarzyna Pawi ´nska-W˛asikowska 3, Alicja Józkowicz 2,* and Maciej Siedlar 1,* 1 Department of Clinical Immunology, Institute of Pediatrics, Jagiellonian University Medical College, 31-663 Kraków, Poland; [email protected] (J.W.); [email protected] (E.P.) 2 Department of Medical Biotechnology, Faculty of Biochemistry, Biophysics and Biotechnology, Jagiellonian University, 31-007 Kraków, Poland; [email protected] (M.K.); [email protected] (A.K.-C.); [email protected] (M.C.); [email protected] (M.G.); [email protected] (W.N.) 3 Pediatric, Oncology and Hematology Department, Institute of Pediatrics, Jagiellonian University Medical College, 30-387 Krakow, Poland; [email protected] (A.W.); [email protected] (K.P.-W.) * Correspondence: [email protected] (K.B.-S.); [email protected] (A.J.); [email protected] (M.S.); Tel.: +48-(12)-664-6411 (A.J.); +48-(12)-658-2486 (M.S.); Fax: +48-(12)-658-1756 (M.S.) Citation: Bukowska-Strakova, K.; Włodek, J.; Pitera, E.; Kozakowska, Abstract: Whilst the survival rates of childhood acute lymphoblastic leukemia (ALL) have increased M.; Konturek-Cie´sla,A.; Cie´sla,M.; remarkably over the last decades, the therapy resistance and toxicity are still the major causes Go´nka,M.; Nowak, W.; Wieczorek, of treatment failure. -
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Myeloid Growth Factors
NCCN Guidelines Index MGF Table of Contents Discussion NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines® ) Myeloid Growth Factors Version 2.2013 NCCN.org Continue Version 2.2013, 08/02/13 © National Comprehensive Cancer Network, Inc. 2013, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®. NCCN Guidelines Version 2.2013 Panel Members NCCN Guidelines Index MGF Table of Contents Myeloid Growth Factors Discussion * Jeffrey Crawford, MD/Chair †‡ Susan Hudock, PharmD å Lee S. Schwartzberg, MD † ‡ Þ Duke Cancer Institute The Sidney Kimmel Comprehensive St. Jude Children's Research Hospital/ Cancer Center at Johns Hopkins The University of Tennessee Health Science James Armitage, MD † x Center- The West Clinic UNMC Eppley Cancer Center at Dwight D. Kloth, PharmD å å The Nebraska Medical Center Fox Chase Cancer Center Sepideh Shayani, PharmD City of Hope Comprehensive Cancer Center Lodovico Balducci, MD † ‡ David J. Kuter, MD, DPhil † ‡ Moffitt Cancer Center Massachusetts General David P. Steensma, MD†‡Þ Hospital Cancer Center Dana-Farber/Brigham and Women’s Pamela Sue Becker, MD, PhD ‡ Þ x Cancer Center Fred Hutchinson Cancer Research Center/ Gary H. Lyman, MD, MPH † ‡ å Seattle Cancer Care Alliance Duke Cancer Institute Mahsa Talbott, PharmD Vanderbilt-Ingram Cancer Center Douglas W. Blayney, MD † Brandon McMahon, MD ‡ Stanford Cancer Institute Robert H. Lurie Comprehensive Cancer Saroj Vadhan-Raj, MD † Þ Center of Northwestern University The University of Texas Spero R. Cataland, MD ‡ MD Anderson Cancer Center The Ohio State University Comprehensive Hope S. Rugo, MD † ‡ x Cancer Center - James Cancer Hospital UCSF Helen Diller Family Peter Westervelt, MD, PhD † Siteman Cancer Center at Barnes- and Solove Research Institute Comprehensive Cancer Center Jewish Hospital and Washington University School of Medicine Mark L. -

Improving Outcomes of Chemotherapy: Established and Novel Options for Myeloprotection in the COVID-19 Era
REVIEW published: 08 July 2021 doi: 10.3389/fonc.2021.697908 Improving Outcomes of Chemotherapy: Established and Novel Options for Myeloprotection in the COVID-19 Era Gary H. Lyman 1,2*, Nicole M. Kuderer 3 and Matti Aapro 4 1 Public Health Sciences and Clinical Research, Fred Hutchinson Cancer Research Center, Seattle, WA, United States, 2 Department of Medicine, University of Washington, Seattle, WA, United States, 3 Advanced Cancer Research Group, Seattle, WA, United States, 4 Genolier Cancer Center, Clinique de Genolier, Genolier, Switzerland Chemotherapy-induced damage of hematopoietic stem and progenitor cells (HPSCs) often results in myelosuppression that adversely affects patient health and quality of life. Currently, chemotherapy-induced myelosuppression is managed with chemotherapy dose delays/reductions and lineage-specific supportive care interventions, such as Edited by: hematopoietic growth factors and blood transfusions.However,theCOVID-19 Fabrizio Martelli, National Institute of Health (ISS), Italy pandemic has created additional challenges for the optimal management of Reviewed by: myelosuppression. In this review, we discuss the impact of this side effect on patients Jorge J. Nieva, treated with myelosuppressive chemotherapy, with a focus on the prevention of University of Southern California, United States myelosuppression in the COVID-19 era. During the COVID-19 pandemic, short-term Leonidas Apostolidis, recommendations on the use of supportive care interventions have been issued with the National Center for Tumor Diseases aim of minimizing the risk of infection, reducing the need for hospitalization, and preserving Heidelberg (NCT), Germany *Correspondence: limited blood supplies. Recently, trilaciclib, an intravenous cyclin-dependent kinase 4 and Gary H. Lyman 6 inhibitor, was approved to decrease the incidence of myelosuppression in adult patients [email protected] when administered prior to platinum/etoposide-containing or topotecan-containing Specialty section: chemotherapy for extensive-stage small cell lung cancer (ES-SCLC). -

Pharmacology of Recombinant Or Genetically Engineered Drugs
Pharmacology Pharmacology of Recombinant or Genetically Engineered Drugs Kamal Kishore, Pawan Krishan1 Departments of Pharmacy, M.J.P. Rohilkhand University, Bareilly-243 006, Uttar Pradesh, 1Pharmaceutical Sciences and Drug Research, Punjabi University, Patiala-147 002, Punjab, India Address for correspondence: Dr. Kamal Kishore; E-mail: [email protected] ABSTRACT Recombinant technology or genetic engineering is a modern method used for the synthesis of therapeutic agents. The central theme of recombinant technology is the process of “gene cloning” which consists of the production of a deÞ ned fragment of DNA and its propagation and ampliÞ cation in a suitable host cell. Drugs developed by recombinant technology or genetic engineering are known as biologics, biopharmaceuticals, recombinant DNA expressed products, bioengineered, or genetically engineered drugs. A current list of various products developed by recombinant technology includes erythropoietin, coagulation modulators, enzymes, hormones, interferons, interleukins, granulocyte colony-stimulating factors, anti-rheumatoid drugs, and various other agents like TNF, becaplermin, hepatitis-B vaccine, antibodies etc. This article provides general as well as recent pharmacological information on different aspects of recombinant drugs that may be useful for their better understanding by users and health care professionals. Key words: Biologics, erythropoietin, interferon, interleukins, insulin, thrombolytic enzymes DOI: 10.4103/0975-1483.55747 INTRODUCTION fragment of DNA and its propagation and ampliÞ cation in a suitable host cell. Recombinant technology was only Drugs developed using living organisms with the help of possible after the discovery of restriction endonucleases, biotechnology or genetic engineering are known as biologics, the enzymes used as cutters for a desired segment[3] of biopharmaceuticals, recombinant DNA expressed genes known as recognition sequences. -

Myeloid Growth Factors, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology
1520 NCCN Ayman A. Saad, MD; Lee S. Schwartzberg, MD; Sepideh Shayani, PharmD; Mahsa Talbott, PharmD; Saroj Vadhan-Raj, MD; Sumithira Vasu, MBBS; Myeloid Growth Factors, Martha Wadleigh, MD; Peter Westervelt, MD, PhD; Jennifer L. Burns; and Lenora Pluchino, PhD Version 2.2017 Overview Clinical Practice Guidelines in Oncology Myeloid growth factors (MGFs) are a class of biolog- Jeffrey Crawford, MD; Pamela Sue Becker, MD, PhD; ic agents that regulate the proliferation, differentia- James O. Armitage, MD; Douglas W. Blayney, MD; tion, survival, and activation of cells in the myeloid Julio Chavez, MD; Peter Curtin, MD; Shira Dinner, MD; Thomas Fynan, MD; Ivana Gojo, MD; lineage. In patients with cancer receiving myelosup- Elizabeth A. Griffiths, MD; Shannon Hough, PharmD, BCOP; pressive chemotherapy, MGFs are primarily used to Dwight D. Kloth, PharmD, BCOP; David J. Kuter, MD, DPhil; reduce the incidence of neutropenia. Neutropenia is Gary H. Lyman, MD, MPH, FRCP; Mary Mably, RPh, BCOP; defined as an absolute neutrophil count (ANC) of Sudipto Mukherjee, MD, PhD, MPH; Shiven Patel, MD; <500 neutrophils/mcL or an ANC of <1,000 neu- Lia E. Perez, MD; Adam Poust, PharmD; trophils/mcL and a predicted decline ≤500 neutro- Raajit Rampal, MD, PhD; Vivek Roy, MD; Hope S. Rugo, MD; phils/mcL over the next 48 hours. Neutropenia can Abstract Please Note Myeloid growth factors (MGFs) are given as supportive care to The NCCN Clinical Practice Guidelines in Oncol- patients receiving myelosuppressive chemotherapy to reduce ogy (NCCN Guidelines®) are a statement of consensus the incidence of neutropenia. This selection from the NCCN of the authors regarding their views of currently accepted Guidelines for MGFs focuses on the evaluation of regimen- approaches to treatment. -

INN Working Document 05.179 Update December 2010
INN Working Document 05.179 Update December 2010 International Nonproprietary Names (INN) for biological and biotechnological substances (a review) INN Working Document 05.179 Distr.: GENERAL ENGLISH ONLY 12/2010 International Nonproprietary Names (INN) for biological and biotechnological substances (a review) Programme on International Nonproprietary Names (INN) Quality Assurance and Safety: Medicines Essential Medicines and Pharmaceutical Policies (EMP) International Nonproprietary Names (INN) for biological and biotechnological substances (a review) © World Health Organization 2010 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. -
Horizon Scanning Status Report December 2020
PCORI Health Care Horizon Scanning System Volume 2 Issue 4 Horizon Scanning Status Report December 2020 Prepared for: Patient-Centered Outcomes Research Institute 1828 L St., NW, Suite 900 Washington, DC 20036 Contract No. MSA-HORIZSCAN-ECRI-ENG-2018.7.12 Prepared by: ECRI Institute 5200 Butler Pike Plymouth Meeting, PA 19462 Investigators: Randy Hulshizer, MA, MS Damian Carlson, MS Christian Cuevas, PhD Andrea Druga, MSPAS, PA-C Marcus Lynch, PhD, MBA Misha Mehta, MS Prital Patel, MPH Brian Wilkinson, MA Donna Beales, MLIS Jennifer De Lurio, MS Eloise DeHaan, BS Eileen Erinoff, MSLIS Cassia Hulshizer, BBA Madison Kimball, MS Maria Middleton, MPH Melinda Rossi, BS Diane Robertson, BA Kelley Tipton, MPH Rosemary Walker, MLIS Andrew Furman, MD, MMM, FACEP Statement of Funding and Purpose This report incorporates data collected during implementation of the Patient-Centered Outcomes Research Institute (PCORI) Health Care Horizon Scanning System, operated by ECRI under contract to PCORI, Washington, DC (Contract No. MSA-HORIZSCAN-ECRI-ENG-2018.7.12). The findings and conclusions in this document are those of the authors, who are responsible for its content. No statement in this report should be construed as an official position of PCORI. An intervention that potentially meets inclusion criteria might not appear in this report simply because the Horizon Scanning System has not yet detected it or it does not yet meet the inclusion criteria outlined in the PCORI Health Care Horizon Scanning System: Horizon Scanning Protocol and Operations Manual. Inclusion or absence of interventions in the horizon scanning reports will change over time as new information is collected; therefore, inclusion or absence should not be construed as either an endorsement or a rejection of specific interventions. -

Evaluation of Effectiveness of Granulocyte-Macrophage Colony-Stimulating Factor Therapy to Cancer Patients After Chemotherapy: a Meta-Analysis
www.oncotarget.com Oncotarget, 2018, Vol. 9, (No. 46), pp: 28226-28239 Meta-Analysis Evaluation of effectiveness of granulocyte-macrophage colony-stimulating factor therapy to cancer patients after chemotherapy: a meta-analysis Wen-Liang Yu1 and Zi-Chun Hua1,2,3 1The State Key Laboratory of Quality Research in Chinese Medicine, Macau Institute for Applied Research in Medicine and Health, Macau University of Science and Technology, Macao, China 2The State Key Laboratory of Pharmaceutical Biotechnology, School of Life Sciences, Nanjing University, Nanjing, China 3Changzhou High-Tech Research Institute of Nanjing University and Jiangsu TargetPharma Laboratories Inc., Changzhou, China Correspondence to: Zi-Chun Hua, email: [email protected] Keywords: GM-CSF; hematologic index; meta-analysis Received: August 14, 2017 Accepted: February 28, 2018 Published: June 15, 2018 Copyright: Yu et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License 3.0 (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT The impact of granulocyte-macrophage colony stimulating factor (GM-CSF) on hematologic indexes and complications remains existing contradictory evidence in cancer patients after treatment of chemotherapy. Eligible studies up to March 2017 were searched and reviewed from PubMed and Wanfang databases. Totally 1043 cancer patients from 15 studies were included in our research. The result indicated that GM-CSF could significantly improve white blood cells count (SMD = 1.16, 95% CI: 0.71 – 1.61, Z = 5.03, P < 0.00001) and reduce the time to leukopenia recovery (SMD = -0.85, 95% CI: -1.16 – -0.54, Z = 5.38, P < 0.00001) in cancer patients after treatment of chemotherapy.