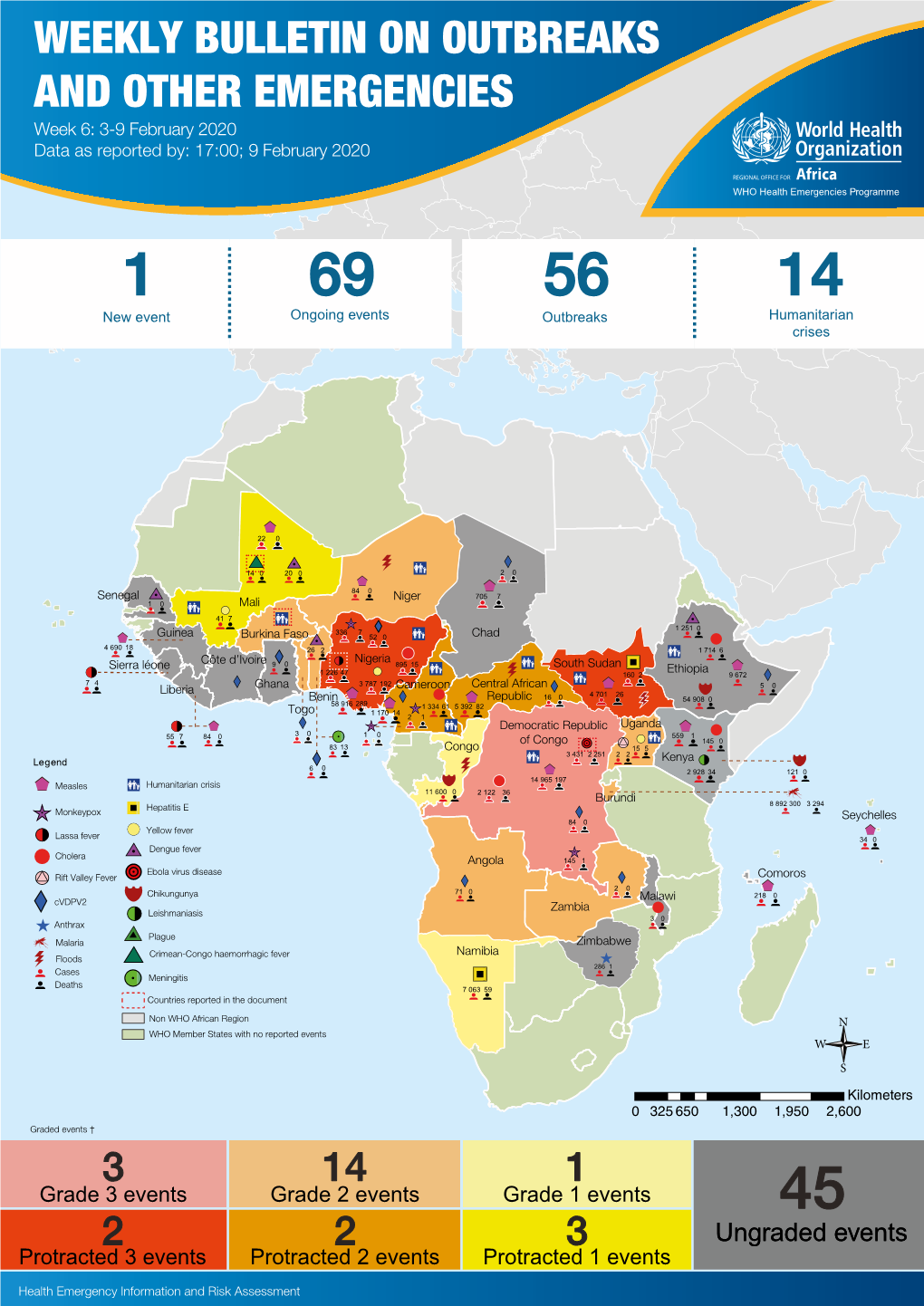
WEEKLY BULLETIN on OUTBREAKS and OTHER EMERGENCIES Week 6: 3-9 February 2020 Data As Reported By: 17:00; 9 February 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses
ARIZONA ARBOVIRAL HANDBOOK FOR CHIKUNGUNYA, DENGUE, AND ZIKA VIRUSES 7/31/2017 Arizona Department of Health Services | P a g e 1 Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses OBJECTIVES .............................................................................................................. 4 I: CHIKUNGUNYA ..................................................................................................... 5 Chikungunya Ecology and Transmission ....................................... 6 Chikungunya Clinical Disease and Case Management ............... 7 Chikungunya Laboratory Testing .................................................. 8 Chikungunya Case Definitions ...................................................... 9 Chikungunya Case Classification Algorithm ............................... 11 II: DENGUE .............................................................................................................. 12 Dengue Ecology and Transmission .............................................. 14 Dengue Clinical Disease and Case Management ...................... 14 Dengue Laboratory Testing ......................................................... 17 Dengue Case Definitions ............................................................ 19 Dengue Case Classification Algorithm ....................................... 23 III: ZIKA .................................................................................................................. -

Uveal Involvement in Marburg Virus Disease B
Br J Ophthalmol: first published as 10.1136/bjo.61.4.265 on 1 April 1977. Downloaded from British Journal of Ophthalmology, 1977, 61, 265-266 Uveal involvement in Marburg virus disease B. S. KUMING AND N. KOKORIS From the Department of Ophthalmology, Johannesburg General Hospital and University of the Witwatersrand SUMMARY The first reported case of uveal involvement in Marburg virus disease is described. 'Ex Africa semper aliquid novi'. Two outbreaks of Marburg virus disease have been Rhodesia and had also been constantly at his documented. The first occurred in Marburg and bedside till his death. Lassa fever was suspected and Frankfurt, West Germany, in 1967 (Martini, 1969) she was given a unit of Lassa fever convalescent and the second in Johannesburg in 1975 (Gear, serum when she became desperately ill on the fifth 1975). This case report describes the third patient day. She also developed acute pancreatitis. Within in the Johannesburg outbreak, who developed an 52 hours she made a dramatic and uneventful anterior uveitis. The cause of the uveitis was proved recovery. Her illness mainly affected the haema- to be the Marburg virus by identiying it in a tissue topoietic, hepatic, and pancreatic systems. culture of her aqueous fluid. The subject of this report was a nurse who had helped to nurse patients 1 and 2. Nine days after the Case report death ofthe first patient she presented with lower back pain and high fever. She developed hepatitis, a mild Before describing the case history of the patient the disseminated intravascular coagulation syndrome, events leading to her contracting the disease must successfully treated with heparin, and the classical be briefly described. -

African Traditional Medicine Day Rganization Regional Office for Africa O Rganization of the World H Ealth a Serial Publication
august 2010 · special issue 14 · a serial publication of the World health organization regional office for africa · issn 2077 6136 tHe AfricAn monitor Healt 31 August 31 Day Medicine Traditional African special H issue r EG i O n AL O ffic E f O r Africa The African Health Monitor is a magazine of the World Health Organization Regional Office for Africa (WHO- AFRO) published four times a year (January, April, July and October). It is a multilingual publication with peer- reviewed articles in English, French and Portuguese. REGIONAL OFFICE FOR Africa The aim of the African Health Monitor is to promote and facilitate evidence-based policy and decisions to strengthening programmes for health promotion, protection, and restoration in the African Region. In order to achieve its aim, the Monitor serves as a medium for publication of articles that monitor the health n A situation and trends, and track progress toward the health-related Millennium Development Goals and other internationally agreed-upon goals. It will publish and disseminate relevant and scientifically rigorous public HealtH health information. It will also disseminate information on public health interventions carried out in the Member States with the cooperation of AFRO technical programmes. Afric e Prospective authors should follow the Monitor stylesheet, which can be obtained by sending an email H t monitor message to the Editorial Office at [email protected] or by using this intranet link http://intranet.afro.who.int/ guidelines/ahm.pdf african traditional Paul Lusamba-Dikassa (Editor-in-Chief) for the African Health Monitor Special Issue on Traditional Medicine medicine day, 31 august EditorialUche Amazigo Board ExpErt adviSorY panel special issue Rufaro Chatora Dr Kofi Busia, WAHO, Burkina Faso Alimata J. -

Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis
Antiviral Research 99 (2013) 345–370 Contents lists available at SciVerse ScienceDirect Antiviral Research journal homepage: www.elsevier.com/locate/antiviral Review Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy ⇑ Simon-Djamel Thiberville a,b, , Nanikaly Moyen a,b, Laurence Dupuis-Maguiraga c,d, Antoine Nougairede a,b, Ernest A. Gould a,b, Pierre Roques c,d, Xavier de Lamballerie a,b a UMR_D 190 ‘‘Emergence des Pathologies Virales’’ (Aix-Marseille Univ. IRD French Institute of Research for Development EHESP French School of Public Health), Marseille, France b University Hospital Institute for Infectious Disease and Tropical Medicine, Marseille, France c CEA, Division of Immuno-Virologie, Institute of Emerging Diseases and Innovative Therapies, Fontenay-aux-Roses, France d UMR E1, University Paris Sud 11, Orsay, France article info abstract Article history: Chikungunya virus (CHIKV) is the aetiological agent of the mosquito-borne disease chikungunya fever, a Received 7 April 2013 debilitating arthritic disease that, during the past 7 years, has caused immeasurable morbidity and some Revised 21 May 2013 mortality in humans, including newborn babies, following its emergence and dispersal out of Africa to the Accepted 18 June 2013 Indian Ocean islands and Asia. Since the first reports of its existence in Africa in the 1950s, more than Available online 28 June 2013 1500 scientific publications on the different aspects of the disease and its causative agent have been pro- duced. Analysis of these publications shows that, following a number of studies in the 1960s and 1970s, Keywords: and in the absence of autochthonous cases in developed countries, the interest of the scientific commu- Chikungunya virus nity remained low. -

Antibody-Mediated Enhancement Aggravates Chikungunya Virus
www.nature.com/scientificreports OPEN Antibody-mediated enhancement aggravates chikungunya virus infection and disease severity Received: 14 July 2017 Fok-Moon Lum 1,2, Thérèse Couderc3,4, Bing-Shao Chia1,8, Ruo-Yan Ong1,9, Zhisheng Her1,10, Accepted: 17 January 2018 Angela Chow5, Yee-Sin Leo5, Yiu-Wing Kam1, Laurent Rénia1, Marc Lecuit 3,4,6 & Published: xx xx xxxx Lisa F. P. Ng1,2,7 The arthropod-transmitted chikungunya virus (CHIKV) causes a fu-like disease that is characterized by incapacitating arthralgia. The re-emergence of CHIKV and the continual risk of new epidemics have reignited research in CHIKV pathogenesis. Virus-specifc antibodies have been shown to control virus clearance, but antibodies present at sub-neutralizing concentrations can also augment virus infection that exacerbates disease severity. To explore this occurrence, CHIKV infection was investigated in the presence of CHIKV-specifc antibodies in both primary human cells and a murine macrophage cell line, RAW264.7. Enhanced attachment of CHIKV to the primary human monocytes and B cells was observed while increased viral replication was detected in RAW264.7 cells. Blocking of specifc Fc receptors (FcγRs) led to the abrogation of these observations. Furthermore, experimental infection in adult mice showed that animals had higher viral RNA loads and endured more severe joint infammation in the presence of sub-neutralizing concentrations of CHIKV-specifc antibodies. In addition, CHIKV infection in 11 days old mice under enhancing condition resulted in higher muscles viral RNA load detected and death. These observations provide the frst evidence of antibody-mediated enhancement in CHIKV infection and pathogenesis and could also be relevant for other important arboviruses such as Zika virus. -

Viral Hemorrhagic Fevers and Bioterrorism
What you need to know about . Viral Hemorrhagic Fevers and Bioterrorism What are viral hemorrhagic fevers? How are viral hemorrhagic fevers Viral hemorrhagic fevers (VHFs) are a spread? group of illnesses caused by several distinct In nature, viruses causing hemorrhagic fever families of viruses. In general the term typically are passed from mice, rats, fleas “viral hemorrhagic fever” describes severe and ticks to humans. People can be infected problems affecting several organ systems when they come in contact with urine, fecal in the body. Typically, the entire system of ma�er, saliva or other body fluids from blood vessels is damaged, and the body has infected rodents. Fleas and ticks transmit the problems regulating itself. Symptoms o�en viruses when they bite a person or when a include bleeding, but the bleeding itself is person crushes a tick. Hosts for some viruses rarely life-threatening. VHFs are caused by such as Ebola and Marburg are not known. viruses of four families: Some viruses such as Ebola, Marburg and Lassa can be spread from person to person • Arenavirus including Lassa fever and by direct contact with infected blood or Argentine, Bolivian, Brazilian and organs or indirectly through contact with Venezuelan hemorrhagic fevers; objects such as syringes or needles that are • Filovirus including Ebola and Marburg; contaminated with infected body fluids. • Bunyavirus including Hantavirus and Ri� Valley Fever; What are the symptoms? • Flavivirus including yellow fever and Symptoms vary with the different virus dengue fever. families, but first signs o�en include sudden fever, weakness, muscle pain, tiredness, Can viral hemorrhagic fevers be used headache and sore throat. -

Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on Suspicion of Infection During Business Hours
Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on suspicion of infection during business hours PROTOCOL CHECKLIST Enter available information into Merlin upon receipt of initial report Review background information on the disease (see Section 2), case definitions (see Section 3 for dengue and for chikungunya), and laboratory testing (see Section 4) Forward specimens to the Florida Department of Health (DOH) Bureau of Public Health Laboratories (BPHL) for confirmatory laboratory testing (as needed) Inform local mosquito control personnel of suspected chikungunya or dengue case as soon as possible (if applicable) Inform state Arbovirus Surveillance Coordinator on suspicion of locally acquired arbovirus infection Contact provider (see Section 5A) Interview case-patient Review disease facts (see Section 2) Mode of transmission Ask about exposure to relevant risk factors (see Section 5. Case Investigation) History of travel, outdoor activities, and mosquito bites two weeks prior to onset History of febrile illness or travel for household members or other close contacts in the month prior to onset History of previous arbovirus infection or vaccination (yellow fever, Japanese encephalitis) Provide education on transmission and prevention (see Section 6) Awareness of mosquito-borne diseases Drain standing water at least weekly to stop mosquitoes from multiplying Discard items that collect water and are not being used Cover skin with clothing or Environmental Protection Agency (EPA)-registered repellent such as DEET (N,N-diethyl-meta-toluamide) Use permethrin on clothing (not skin) according to manufacturer’s directions Cover doors and windows with intact screens to keep mosquitoes out of the house Enter additional data obtained from interview into Merlin (see Section 5D) Arrange for a convalescent specimen to be taken (if necessary) Dengue/Chikungunya Guide to Surveillance and Investigation Dengue Fever/Severe Dengue/Chikungunya 1. -

Defeating Malaria Through Pharmaceutical Systems Strengthening Results from the Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program
DEFEATING MALARIA THROUGH PHARMACEUTICAL SYSTEms STRENGTHENING Results from the Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program Seydou Doumbia, Aubrey Clark, and Andwele Mwansasu Acknowledgements The authors would like to thank the 70+ in-country staff, partners, and stakeholders who shared their insights through in-depth interviews, without which this report would not have been possible. Photos taken by Aubrey Clark (MSH/SIAPS) unless otherwise noted. ABOUT SIAPS | The Systems for Improved Access to Pharmaceuticals and Services (SIAPS) program works to ensure access to quality pharmaceutical products and effective pharmaceutical services through systems-strengthening approaches to achieve positive and lasting health outcomes. SIAPS is funded by the US Agency for International Development (USAID) and implemented by Management Sciences for Health. For more information, visit www.SIAPSprogram.org. The information provided in this document does not reflect or represent the position or views of the US Agency for International Development or the US Government. ACRONYMS ACT artemisinin-based combination therapy APTS Auditable Pharmacy Transactions and Services CRMS Continuous Results Monitoring System DNPL Direction Nationale de la Pharmacie et des Laboratoires DRC Democratic Republic of the Congo DTC drug and therapeutics committee EML essential medicines list EUV End Use Verification GFATM Global Fund to Fight AIDS, TB, and Malaria IPTp intermittent preventive treatment in pregnancy LMIS logistics management information -

Viral Hemorrhagic Fevers (Lassa, Marburg, Ebola, Crimean-Congo, and Other Emerging Viruses)
Viral Hemorrhagic Fevers (Lassa, Marburg, Ebola, Crimean-Congo, and other emerging viruses) What Are They? Viral hemorrhagic fevers are a group of illnesses causes by several viruses. These viruses affect multiple organs in the body by damaging the vascular (blood vessel) system. The bleeding or hemorrhaging caused by the virus is not usually life threatening but damage to organ systems in the body can range from mild to deadly. The viruses responsible for this type of illness include Lassa, Marburg, Ebola, and Crimean-Congo hemorrhagic fever. How can you get it? These emerging viral hemorrhagic fevers are presumed to be animal borne (zoonotic) and can be transmitted to humans through contact. Infected humans can spread the virus to each other through contact with contaminated objects or blood. The risk of acquiring these diseases is typically restricted to the geographic regions where the virus is found. Given global travel, rare cases have been reported outside of the host region. These rare cases are probably the greatest form of the occupational threat to fire fighters. Lassa Associated with specific rodents Found in West Africa Marburg Transmitted by African fruit bat Found in Africa Ebola Transmitted by unknown animal Found in Africa Crimean-Congo Tick-borne virus Found in Africa, Asia, Europe What are the symptoms? The time to develop symptoms varies by virus but is between 2 to 21 days after exposure to the Ebola virus. The signs and symptoms of viral hemorrhagic fever vary depending on the virus but include: Flu-like symptoms o Fever o Fatigue o Muscle aches Exhaustion Nausea and/or vomiting Abdominal pain Shock Seizures Delirium Bleeding Organ failure The most common complication of Lassa fever is deafness. -

1 Lujo Viral Hemorrhagic Fever: Considering Diagnostic Capacity And
1 Lujo Viral Hemorrhagic Fever: Considering Diagnostic Capacity and 2 Preparedness in the Wake of Recent Ebola and Zika Virus Outbreaks 3 4 Dr Edgar Simulundu1,, Prof Aaron S Mweene1, Dr Katendi Changula1, Dr Mwaka 5 Monze2, Dr Elizabeth Chizema3, Dr Peter Mwaba3, Prof Ayato Takada1,4,5, Prof 6 Guiseppe Ippolito6, Dr Francis Kasolo7, Prof Alimuddin Zumla8,9, Dr Matthew Bates 7 8,9,10* 8 9 1 Department of Disease Control, School of Veterinary Medicine, University of Zambia, 10 Lusaka, Zambia 11 2 University Teaching Hospital & National Virology Reference Laboratory, Lusaka, Zambia 12 3 Ministry of Health, Republic of Zambia 13 4 Division of Global Epidemiology, Hokkaido University Research Center for Zoonosis 14 Control, Sapporo, Japan 15 5 Global Institution for Collaborative Research and Education, Hokkaido University, Sapporo, 16 Japan 17 6 Lazzaro Spallanzani National Institute for Infectious Diseases, IRCCS, Rome, Italy 18 7 World Health Organization, WHO Africa, Brazzaville, Republic of Congo 19 8 Department of Infection, Division of Infection and Immunity, University College London, 20 U.K 21 9 University of Zambia – University College London Research & Training Programme 22 (www.unza-uclms.org), University Teaching Hospital, Lusaka, Zambia 23 10 HerpeZ (www.herpez.org), University Teaching Hospital, Lusaka, Zambia 24 25 *Corresponding author: Dr. Matthew Bates 26 Address: UNZA-UCLMS Research & Training Programme, University Teaching Hospital, 27 Lusaka, Zambia, RW1X 1 28 Email: [email protected]; Phone: +260974044708 29 30 2 31 Abstract 32 Lujo virus is a novel old world arenavirus identified in Southern Africa in 2008 as the 33 cause of a viral hemorrhagic fever (VHF) characterized by nosocomial transmission 34 with a high case fatality rate of 80% (4/5 cases). -
Corruption and Integrity Programme
Anti-Corruption and Integrity Programme A Study on the Link between Corruption and the Causes of Migration and Forced Displacement Human CorruptionSecurity Published by: A Study on the Link between Corruption and the Causes of Migration and Forced Displacement March 29, 2017 Authors: Ortrun Merkle* Julia Reinold* Melissa Siegel* *Maastricht Graduate School of Governance The publication “A Study on the Link between Corruption and the Causes of Migration and Forced Displacement” was commissioned by the Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH, Anti-Corruption and Integrity Programme, on behalf of the German Federal Ministry for Economic Cooperation and Development (BMZ). The contents of this publication do not represent the official position of neither BMZ nor GIZ. Table of Content 3 Table of Content List of Figures ..........................................................5 List of Tables...........................................................6 List of Boxes ...........................................................7 Acknowledgments .......................................................7 Abbreviations ...........................................................7 Executive Summary ......................................................9 1. Introduction ........................................................10 2. Mapping the Conceptual Terrain: Corruption and Migration .....................13 2.1. Corruption - what do we mean? 13 2.2. The concept of human security 16 2.3. Migration – the background 18 3. Methodology -

Orthohantaviruses Belonging to Three Phylogroups All Inhibit Apoptosis in Infected Target Cells
www.nature.com/scientificreports OPEN Orthohantaviruses belonging to three phylogroups all inhibit apoptosis in infected target cells Received: 13 July 2018 Carles Solà-Riera1, Shawon Gupta1,2, Hans-Gustaf Ljunggren1 & Jonas Klingström 1 Accepted: 3 December 2018 Orthohantaviruses, previously known as hantaviruses, are zoonotic viruses that can cause hantavirus Published: xx xx xxxx pulmonary syndrome (HPS) and hemorrhagic fever with renal syndrome (HFRS) in humans. The HPS-causing Andes virus (ANDV) and the HFRS-causing Hantaan virus (HTNV) have anti-apoptotic efects. To investigate if this represents a general feature of orthohantaviruses, we analysed the capacity of six diferent orthohantaviruses – belonging to three distinct phylogroups and representing both pathogenic and non-pathogenic viruses – to inhibit apoptosis in infected cells. Primary human endothelial cells were infected with ANDV, HTNV, the HFRS-causing Puumala virus (PUUV) and Seoul virus, as well as the putative non-pathogenic Prospect Hill virus and Tula virus. Infected cells were then exposed to the apoptosis-inducing chemical staurosporine or to activated human NK cells exhibiting a high cytotoxic potential. Strikingly, all orthohantaviruses inhibited apoptosis in both settings. Moreover, we show that the nucleocapsid (N) protein from all examined orthohantaviruses are potential targets for caspase-3 and granzyme B. Recombinant N protein from ANDV, PUUV and the HFRS-causing Dobrava virus strongly inhibited granzyme B activity and also, to certain extent, caspase-3 activity. Taken together, this study demonstrates that six diferent orthohantaviruses inhibit apoptosis, suggesting this to be a general feature of orthohantaviruses likely serving as a mechanism of viral immune evasion. Orthohantaviruses, of the order Bunyavirales and previously known as hantaviruses, are small single-stranded negative-sense RNA viruses with a tri-segmented genome (S, M and L segments) encoding four to fve proteins.