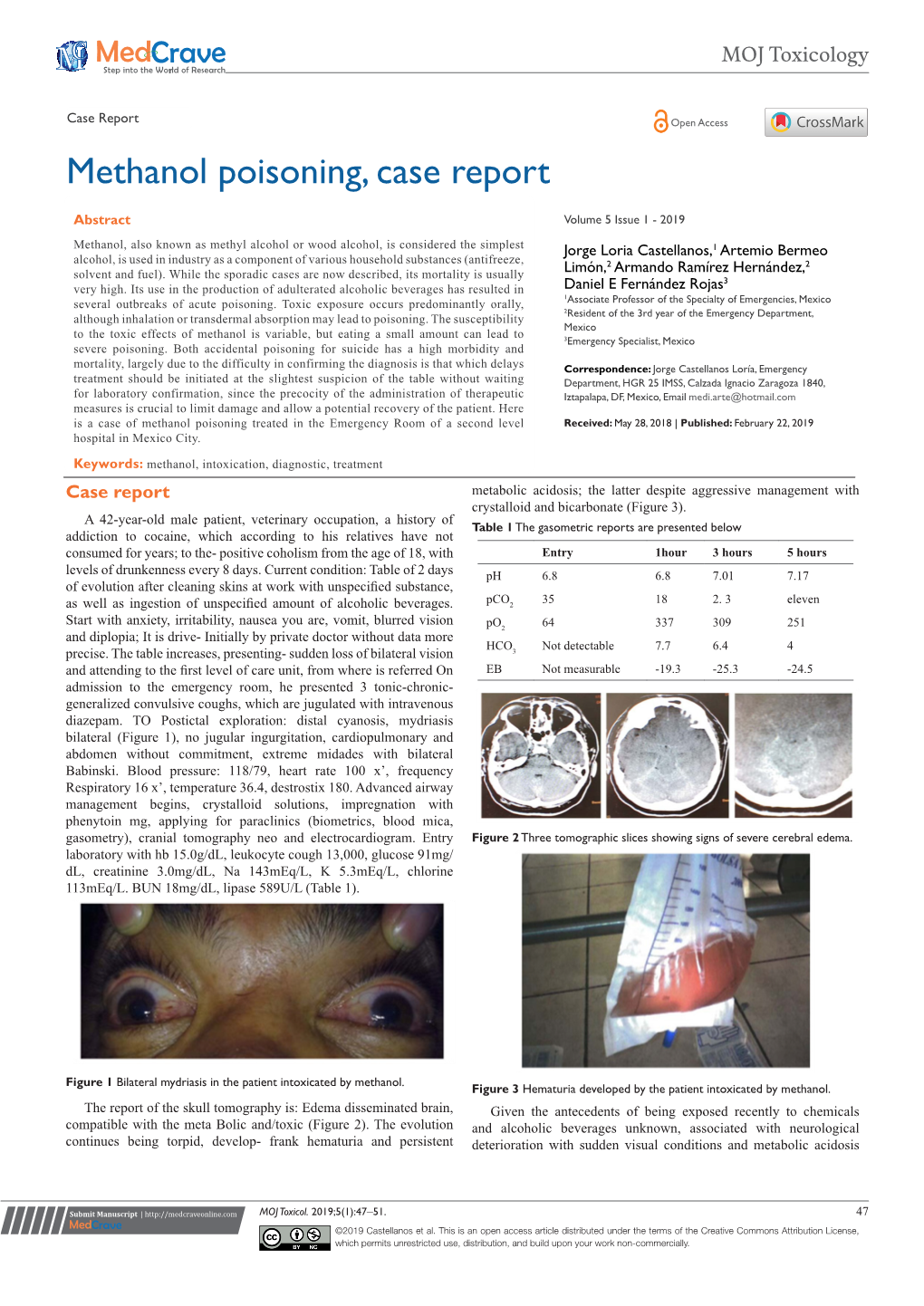
Methanol Poisoning, Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Four Patients with Amanita Phalloides Poisoning CASE SERIE
CASE SERIE 353 Four patients with Amanita Phalloides poisoning S. Vanooteghem1, J. Arts2, S. Decock2, P. Pieraerts3, W. Meersseman4, C. Verslype1, Ph. Van Hootegem2 (1) Department of hepatology, UZ Leuven ; (2) Department of gastroenterology, AZ St-Lucas, Brugge ; (3) General Practitioner, Zedelgem ; (4) Department of internal medicine, UZ Leuven. Abstract because they developed stage 2 hepatic encephalopathy. With maximal supportive therapy, all patients gradually Mushroom poisoning by Amanita phalloides is a rare but poten- improved from day 3 and recovered without the need for tially fatal disease. The initial symptoms of nausea, vomiting, ab- dominal pain and diarrhea, which are typical for the intoxication, liver transplantation. They were discharged from the can be interpreted as a common gastro-enteritis. The intoxication hospital between 6 to 10 days after admission. can progress to acute liver and renal failure and eventually death. Recognizing the clinical syndrome is extremely important. In this case report, 4 patients with amatoxin intoxication who showed the Discussion typical clinical syndrome are described. The current therapy of amatoxin intoxication is based on small case series, and no ran- Among mushroom intoxications, amatoxin intoxica- domised controlled trials are available. The therapy of amatoxin intoxication consists of supportive care and medical therapy with tion accounts for 90% of all fatalities. Amatoxin poison- silibinin and N-acetylcysteine. Patients who develop acute liver fail- ing is caused by mushroom species belonging to the gen- ure should be considered for liver transplantation. (Acta gastro- era Amanita, Galerina and Lepiota. Amanita phalloides, enterol. belg., 2014, 77, 353-356). commonly known as the “death cap”, causes the majority Key words : amanita phalloides, mushroom poisoning, acute liver of fatal cases. -

Clinical Biochemistry of Hepatotoxicity
linica f C l To o x l ic a o n r l o u g Singh, J Clinic Toxicol 2011, S:4 o y J Journal of Clinical Toxicology DOI: 10.4172/2161-0495.S4-001 ISSN: 2161-0495 ReviewResearch Article Article OpenOpen Access Access Clinical Biochemistry of Hepatotoxicity Anita Singh1, Tej K Bhat2 and Om P Sharma2* 1CSK Himachal Pradesh, Krishi Vishva Vidyalaya, Palampur (HP) 176 062, India 2Biochemistry Laboratory, Indian Veterinary Research Institute, Regional Station, Palampur (HP) 176 061, India Abstract Liver plays a central role in the metabolism and excretion of xenobiotics which makes it highly susceptible to their adverse and toxic effects. Liver injury caused by various toxic chemicals or their reactive metabolites [hepatotoxicants) is known as hepatotoxicity. The present review describes the biotransformation of hepatotoxicants and various models used to study hepatotoxicity. It provides an overview of pathological and biochemical mechanism involved during hepatotoxicity together with alteration of clinical biochemistry during liver injury. The review has been supported by a list of important hepatotoxicants as well as common hepatoprotective herbs. Keywords: Hepatotoxicity; Hepatotoxicant; In Vivo models; In Vitro production of bile thus leading to the body’s inability to flush out the models; Pathology; Alanine aminotransferase; Alkaline phosphatase; chemicals through waste. Smooth endoplasmic reticulum of the liver is Bilirubin; Hepatoprotective the principal ‘metabolic clearing house’ for both endogenous chemicals like cholesterol, steroid hormones, fatty acids and proteins, and Introduction exogenous substances like drugs and alcohol. The central role played by liver in the clearance and transformation of chemicals exposes it to Hepatotoxicity refers to liver dysfunction or liver damage that is toxic injury [4]. -

Methanol Interim AEGL Document
INTERIM 1: 1/2003 INTERIM 2: 2/2005 INTERIM ACUTE EXPOSURE GUIDELINE LEVELS (AEGLs) METHANOL (CAS Reg. No. 67-56-1) For NAS/COT Subcommittee for AEGLs February 2005 METHANOL Interim 2: 2/2005 PREFACE Under the authority of the Federal Advisory Committee Act (FACA) P. L. 92-463 of 1972, the National Advisory Committee for Acute Exposure Guideline Levels for Hazardous Substances (NAC/AEGL Committee) has been established to identify, review and interpret relevant toxicologic and other scientific data and develop AEGLs for high priority, acutely toxic chemicals. AEGLs represent threshold exposure limits for the general public and are applicable to emergency exposure periods ranging from 10 minutes to 8 hours. AEGL-2 and AEGL-3 levels, and AEGL-1 levels as appropriate, will be developed for each of five exposure periods (10 and 30 minutes, 1 hour, 4 hours, and 8 hours) and will be distinguished by varying degrees of severity of toxic effects. It is believed that the recommended exposure levels are applicable to the general population including infants and children, and other individuals who may be sensitive or susceptible. The three AEGLs have been defined as follows: AEGL-1 is the airborne concentration (expressed as ppm or mg/m;) of a substance above which it is predicted that the general population, including susceptible individuals, could experience notable discomfort, irritation, or certain asymptomatic, non-sensory effects. However, the effects are not disabling and are transient and reversible upon cessation of exposure. AEGL-2 is the airborne concentration (expressed as ppm or mg/m;) of a substance above which it is predicted that the general population, including susceptible individuals, could experience irreversible or other serious, long-lasting adverse health effects, or an impaired ability to escape. -

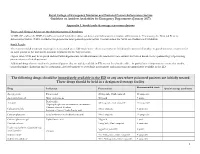
Guideline on Antidote Availability for Emergency Departments January 2017
Royal College of Emergency Medicine and National Poisons Information Service Guideline on Antidote Availability for Emergency Departments January 2017 TOXBASE and/or the BNF should be consulted for further advice on doses and indications for antidote administration and, if necessary, the National Poisons Information Service (NPIS) should be telephoned for more patient-specific advice. Contact details for NPIS are available on TOXBASE. Additional drugs that are used in the poisoned patient that are widely available in ED are not listed in the table – in particular it is important to ensure that insulin, benzodiazepines (diazepam and/or lorazepam), glyceryl trinitrate or isosorbide dinitrate and magnesium are immediately available in the ED. The following drugs should be immediately available in the ED or any area where poisoned patients are initially treated. These drugs should be held in a designated storage facility* The stock held should be sufficient to initiate treatment (stocking guidance is in Appendix 1). Drug Indication Acetylcysteine Paracetamol Activated charcoal Many oral poisons Atropine Organophosphorus or carbamate insecticides Bradycardia Calcium chloride Calcium channel blockers Systemic effects of hydrofluoric acid Calcium gluconate Local infiltration for hydrofluoric acid Calcium gluconate gel Hydrofluoric acid Cyanide antidotes Cyanide Dicobalt edetate The choice of antidote depends on the severity of poisoning, certainty of diagnosis and cause Hydroxocobalamin (Cyanokit®) of poisoning/source of cyanide. Sodium nitrite - Dicobalt edetate is the antidote of choice in severe cases when there is a high clinical Sodium thiosulphate suspicion of cyanide poisoning e.g. after cyanide salt exposure. - Hydroxocobalamin (Cyanokit®) should be considered in smoke inhalation victims who have a severe lactic acidosis, are comatose, in cardiac arrest or have significant cardiovascular compromise - Sodium nitrite may be used if dicobalt edetate is not available. -

Methanol: Toxicological Overview
Methanol Toxicological Overview Key Points Kinetics and metabolism readily absorbed by all routes and distributed in the body water undergoes extensive metabolism, but small quantities are excreted unchanged by the lungs and in the urine Health effects of acute exposure methanol is toxic following ingestion, inhalation or dermal exposure exposure may initially result in CNS depression, followed by an asymptomatic latent period metabolic acidosis and ocular toxicity, which may result in blindness, are subsequent manifestations of toxicity coma and death may occur following substantial exposures long-term effects may include blindness and, following more substantial exposures, permanent damage to the CNS Health effects of chronic exposure long-term inhalation exposure to methanol has resulted in headaches and eye irritation in workers methanol is considered not to be a mutagen or carcinogen in humans methanol is considered not to be a reproductive toxicant in humans PHE publications gateway number: 2014790 Published: August 2015 Compendium of Chemical Hazards: Methanol Summary of Health Effects Methanol may be acutely toxic following inhalation, oral or dermal exposure. Acute methanol toxicity often follows a characteristic series of features; initially central nervous system (CNS) depression and gastrointestinal tract (GI) irritation may be observed. This is typically followed by a latent period of varying duration from 12–24 hours and occasionally up to 48 hours. Subsequently, a severe metabolic acidosis develops with nausea, vomiting and headache. Ocular toxicity ranges from photophobia and misty or blurred vision to markedly reduced visual acuity and complete blindness following high levels of exposure. Ingestion of as little as 4–10 mL of methanol in adults may cause permanent damage. -
RCEM NPIS Antidote Guideline Appx 1
Royal College of Emergency Medicine and National Poisons Information Service Guideline on Antidote Availability for Emergency Departments (January 2017) Appendix 1. Stock levels & storage recommendations Doses and Clinical Advice on the Administration of Antidotes TOXBASE and/or the BNF should be consulted for further advice on doses and indications for antidote administration. If necessary, the National Poisons Information Service (NPIS) should be telephoned for more patient-specific advice. Contact details for NPIS are available on TOXBASE. Stock Levels The recommended minimum stocking levels (rounded up to full “pack-sizes” where necessary) are based on the amount of antidote required to initiate treatment for an adult patient in the ED and to continue treatment for the first 24 hours. Higher stock levels may be required and individual departments should determine the amount of each antidote they stock based on the epidemiology of poisoning presentations to their department. Additional drugs that are used in the poisoned patient that are widely available in ED are not listed in the table – in particular it is important to ensure that insulin, benzodiazepines (diazepam and/or lorazepam), glyceryl trinitrate or isosorbide mononitrate and magnesium are immediately available in the ED. The following drugs should be immediately available in the ED or any area where poisoned patients are initially treated These drugs should be held in a designated storage facility Recommended stock Drug Indication Presentation Special storage conditions -

The Effect of Bacillus Larvicidal Toxins on Mammals
The effect of Bacillus larvicidal toxins On mammals By Nadia Adam Mohammed Ahmed B.Sc. of Veterinary Sciences University of Bahr-Elgazal ٢٠٠٠ Thesis submitted for the partial fulfillment of the requirements For the degree of Master of Science (M.Sc.) in microbiology Supervisor Professor: Mohammed Sulieman El-sanosi Department of microbiology Faculty of Veterinary Medicine University of Khartoum ٢٠٠٦ May To My lovely parents, My husband (M/Elmurtada) and my children (Reem&Rwan) To My brothers and sisters, And To Those who suffer from malaria, I dedicate this work. Nadia I would like to express my sincere thanks to my supervisor Prof. Elsanosi for his valuable supervision and encouragement. I also like to extend my thanks to Prof.Ahamed.A.Gameel for his great help in histopathological investigation of this study. Thanks also extend to all staff and technicians of the Department of Microbiology for their valuable advices and assistance. Iam also greatfull to my colleague and all my friends Special thanks to my family for their patience and continuous encouragement during this work. Abstract Mosquito control is the key for hopeful and sustainable eradication of different socio-economic as well as fatal viral, bacterial and parasitological diseases in the tropical and subtropical countries. In addition the safety of any pesticide should be assured before application. In the present study the susceptibility of arabiensis mosquito larvae to the toxin of two endo-spores forming bacilli strain was examined. Both Bacilli spp B. ٪١٠٠ thuringiensis and B. sphaericus were found to be highly toxic and fatal with was found to be tolerant to the (٤_Instar) ٤_mortality rate. -

Fomepizole for Acetaminophen Toxicity
Clinical Pharmacology & Toxicology Pearl of the Week Fomepizole for Acetaminophen Toxicity Mechanisms There are two ways that fomepizole works to help prevent hepatotoxicity in APAP overdose. The primary mechanism involves inhibition of CYP450 2E1. o When a toxic amount of APAP is ingested, the pathways that convert it into nontoxic metabolites become overwhelmed. o Thus, more APAP gets converted into NAPQI. o Fomepizole inhibits the 2E1 pathway, thus preventing conversion of APAP into NAPQI. The second mechanism of action is the JNK (“junk”) enzyme. o NAPQI-induced mitochondrial dysfunction leads to formation of reactive oxidant species. This oxidant stress leads to activation of c-jun N-terminal kinase, or JNK, enzyme. o This enzyme translocates to the mitochondria, amplifying oxidant stress, and ultimately resulting in the cessation of ATP production. o Additionally, the JNK enzyme can lead to the rupture of the outer mitochondrial membrane, causing release of intermembrane proteins, which can potentially lead to DNA fragmentation o Interestingly, it is thought that both metabolic acidosis, as well as elevated lactate levels, may be the result of alterations in mitochondrial respiratory function o Fomepizole works by preventing the APAP-induced activation of this enzyme. Role in Acetaminophen poisoning management In cases where fomepizole and NAC were administered together, evidence has shown that the combination has contributed to a decrease in both hepatotoxicity and mortality. Most of the evidence has come from case reports and animal models. Currently, fomepizole is recommended for massive APAP ingestions (as in, ingestions over 500- 600 mg/kg or in cases where 4-hour equivalent acetaminophen concentrations over 5000 umol/L). -

METHANOL 6 (CAS Reg
1 INTERIM 1: 1/2003 2 INTERIM 2: 2/2005 3 INTERIM ACUTE EXPOSURE GUIDELINE LEVELS 4 (AEGLs) 5 METHANOL 6 (CAS Reg. No. 67-56-1) 7 For 8 NAS/COT Subcommittee for AEGLs 9 February 2005 METHANOL Interim 2: 2/2005 10 PREFACE 11 Under the authority of the Federal Advisory Committee Act (FACA) P. L. 92-463 of 1972, the 12 National Advisory Committee for Acute Exposure Guideline Levels for Hazardous Substances 13 (NAC/AEGL Committee) has been established to identify, review and interpret relevant toxicologic and 14 other scientific data and develop AEGLs for high priority, acutely toxic chemicals. 15 AEGLs represent threshold exposure limits for the general public and are applicable to emergency 16 exposure periods ranging from 10 minutes to 8 hours. AEGL-2 and AEGL-3 levels, and AEGL-1 levels as 17 appropriate, will be developed for each of five exposure periods (10 and 30 minutes, 1 hour, 4 hours, and 18 8 hours) and will be distinguished by varying degrees of severity of toxic effects. It is believed that the 19 recommended exposure levels are applicable to the general population including infants and children, and 20 other individuals who may be sensitive or susceptible. The three AEGLs have been defined as follows: 21 AEGL-1 is the airborne concentration (expressed as ppm or mg/m³) of a substance above which it 22 is predicted that the general population, including susceptible individuals, could experience notable 23 discomfort, irritation, or certain asymptomatic, non-sensory effects. However, the effects are not disabling 24 and are transient and reversible upon cessation of exposure. -

Estonian Statistics on Medicines 2016 1/41
Estonian Statistics on Medicines 2016 ATC code ATC group / Active substance (rout of admin.) Quantity sold Unit DDD Unit DDD/1000/ day A ALIMENTARY TRACT AND METABOLISM 167,8985 A01 STOMATOLOGICAL PREPARATIONS 0,0738 A01A STOMATOLOGICAL PREPARATIONS 0,0738 A01AB Antiinfectives and antiseptics for local oral treatment 0,0738 A01AB09 Miconazole (O) 7088 g 0,2 g 0,0738 A01AB12 Hexetidine (O) 1951200 ml A01AB81 Neomycin+ Benzocaine (dental) 30200 pieces A01AB82 Demeclocycline+ Triamcinolone (dental) 680 g A01AC Corticosteroids for local oral treatment A01AC81 Dexamethasone+ Thymol (dental) 3094 ml A01AD Other agents for local oral treatment A01AD80 Lidocaine+ Cetylpyridinium chloride (gingival) 227150 g A01AD81 Lidocaine+ Cetrimide (O) 30900 g A01AD82 Choline salicylate (O) 864720 pieces A01AD83 Lidocaine+ Chamomille extract (O) 370080 g A01AD90 Lidocaine+ Paraformaldehyde (dental) 405 g A02 DRUGS FOR ACID RELATED DISORDERS 47,1312 A02A ANTACIDS 1,0133 Combinations and complexes of aluminium, calcium and A02AD 1,0133 magnesium compounds A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 811120 pieces 10 pieces 0,1689 A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 3101974 ml 50 ml 0,1292 A02AD83 Calcium carbonate+ Magnesium carbonate (O) 3434232 pieces 10 pieces 0,7152 DRUGS FOR PEPTIC ULCER AND GASTRO- A02B 46,1179 OESOPHAGEAL REFLUX DISEASE (GORD) A02BA H2-receptor antagonists 2,3855 A02BA02 Ranitidine (O) 340327,5 g 0,3 g 2,3624 A02BA02 Ranitidine (P) 3318,25 g 0,3 g 0,0230 A02BC Proton pump inhibitors 43,7324 A02BC01 Omeprazole -

Research Article Presentations Related to Acute
Hindawi Emergency Medicine International Volume 2019, Article ID 3130843, 7 pages https://doi.org/10.1155/2019/3130843 Research Article Presentations Related to Acute Paracetamol Intoxication in an Urban Emergency Department in Switzerland Natalia Piotrowska,1 Jolanta Klukowska-Ro¨tzler ,1 Beat Lehmann ,1 Gert Krummrey,1 Manuel Haschke,2,3 Aristomenis K. Exadaktylos,1 and Evangelia Liakoni 2,3 1Department of Emergency Medicine, Inselspital, University Hospital Bern, University of Bern, Bern, Switzerland 2Clinical Pharmacology and Toxicology, Department of General Internal Medicine, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland 3Institute of Pharmacology, University of Bern, Bern, Switzerland Correspondence should be addressed to Evangelia Liakoni; [email protected] Received 25 March 2019; Accepted 22 November 2019; Published 6 December 2019 Academic Editor: $eodore J. Gaeta Copyright © 2019 Natalia Piotrowska et al. $is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Aim. To investigate the characteristics of Emergency Department (ED) presentations due to acute paracetamol intoxication. Methods. Retrospective observational study of patients presenting to the ED of Bern University Hospital between May 1, 2012, and October 31, 2018, due to a paracetamol overdose (defined as intake of >4 g/24 h). Cases were identified using the full-text search of the electronic patient database and were grouped into intentional (suicidal/parasuicidal) and unintentional in- toxications (e.g., patient unaware of maximal daily dose). Results. During the study period, 181 cases were included and 143 (79%) of those were intentional. -

Ethanol and Tobacco Abuse in Pregnancy: Anaesthetic Considerations
REVIEW ARTICLE Ethanol and tobacco abuse in pregnancy: Anaesthetic considerations K M Kuczkowski M.D, Assistant Clinical Professor of Anesthesiology and Reproductive Medicine, Co-Director of Obstetric Anesthesia, Departments of Anesthesiology and Reproductive Medicine, University of California, San Diego , USA Introduction The illicit drug abuse in pregnancy has received significant attention over the past two decades.1 However, far too little attention has been given to the consequences of the use of social drugs such as ethanol and tobacco, which are by far the most commonly abused substances during pregnancy. While the deleterious effects of cocaine or amphetamines on the mother and the fetus are more pronounced and easier to detect, the addiction to ethanol and tobacco is usually subtle and more difficult to diagnose.1, 2-4 As a result recreational use of alcohol and tobacco may continue undetected in pregnancy, significantly effecting pregnancy outcome and obstetric and anaesthetic management of these patients. This article reviews the consequences of ethanol and tobacco use in pregnancy and offers recommendation for anaesthetic management of these potentially complicated pregnancies. General considerations rette smoking.2, 17 The American College of Obstetricians and Substance abuse is defined as “self-administration of various drugs Gynaecologists (ACOG) has made multiple recommendations regard- that deviates from medically or socially accepted use, which if pro- ing management of patients with drug abuse during pregnancy. longed can lead to the development of physical and psychological Women who acknowledge use of illicit substance during pregnancy dependence”.5 This chemical dependency is characterized by peri- should be counseled and offered necessary treatment.