Bleeding During Pregnancy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

081999 Disseminated Intravascular Coagulation
The New England Journal of Medicine Current Concepts Systemic activation+ of coagulation DISSEMINATED INTRAVASCULAR COAGULATION Intravascular+ Depletion of platelets+ deposition of fibrin and coagulation factors MARCEL LEVI, M.D., AND HUGO TEN CATE, M.D. Thrombosis of small+ Bleeding and midsize vessels+ ISSEMINATED intravascular coagulation is and organ failure characterized by the widespread activation Dof coagulation, which results in the intravas- Figure 1. The Mechanism of Disseminated Intravascular Coag- cular formation of fibrin and ultimately thrombotic ulation. occlusion of small and midsize vessels.1-3 Intravascu- Systemic activation of coagulation leads to widespread intra- lar coagulation can also compromise the blood sup- vascular deposition of fibrin and depletion of platelets and co- agulation factors. As a result, thrombosis of small and midsize ply to organs and, in conjunction with hemodynam- vessels may occur, contributing to organ failure, and there may ic and metabolic derangements, may contribute to be severe bleeding. the failure of multiple organs. At the same time, the use and subsequent depletion of platelets and coag- ulation proteins resulting from the ongoing coagu- lation may induce severe bleeding (Fig. 1). Bleeding may be the presenting symptom in a patient with disseminated intravascular coagulation, a factor that can complicate decisions about treatment. TABLE 1. COMMON CLINICAL CONDITIONS ASSOCIATED WITH DISSEMINATED ASSOCIATED CLINICAL CONDITIONS INTRAVASCULAR COAGULATION. AND INCIDENCE Sepsis Infectious Disease Trauma Serious tissue injury Disseminated intravascular coagulation is an ac- Head injury Fat embolism quired disorder that occurs in a wide variety of clin- Cancer ical conditions, the most important of which are listed Myeloproliferative diseases in Table 1. -

What Everyone Should Know to Stop Bleeding After an Injury
What Everyone Should Know to Stop Bleeding After an Injury THE HARTFORD CONSENSUS The Joint Committee to Increase Survival from Active Shooter and Intentional Mass Casualty Events was convened by the American College of Surgeons in response to the growing number and severity of these events. The committee met in Hartford Connecticut and has produced a number of documents with rec- ommendations. The documents represent the consensus opinion of a multi-dis- ciplinary committee involving medical groups, the military, the National Security Council, Homeland Security, the FBI, law enforcement, fire rescue, and EMS. These recommendations have become known as the Hartford Consensus. The overarching principle of the Hartford Consensus is that no one should die from uncontrolled bleeding. The Hartford Consensus recommends that all citizens learn to stop bleeding. Further information about the Hartford Consensus and bleeding control can be found on the website: Bleedingcontrol.org 2 SAVE A LIFE: What Everyone Should Know to Stop Bleeding After an Injury Authors: Peter T. Pons, MD, FACEP Lenworth Jacobs, MD, MPH, FACS Acknowledgements: The authors acknowledge the contributions of Michael Cohen and James “Brooks” Hart, CMI to the design of this manual. Some images adapted from Adam Wehrle, EMT-P and NAEMT. © 2017 American College of Surgeons CONTENTS SECTION 1 3 ■ Introduction ■ Primary Principles of Trauma Care Response ■ The ABCs of Bleeding SECTION 2 5 ■ Ensure Your Own Safety SECTION 3 6 ■ A – Alert – call 9-1-1 SECTION 4 7 ■ B – Bleeding – find the bleeding injury SECTION 5 9 ■ C – Compress – apply pressure to stop the bleeding by: ■ Covering the wound with a clean cloth and applying pressure by pushing directly on it with both hands, OR ■Using a tourniquet, OR ■ Packing (stuff) the wound with gauze or a clean cloth and then applying pressure with both hands SECTION 6 13 ■ Summary 2 SECTION 1: INTRODUCTION Welcome to the Stop the Bleed: Bleeding Control for the Injured information booklet. -
Using Tourniquets to Stop Bleeding
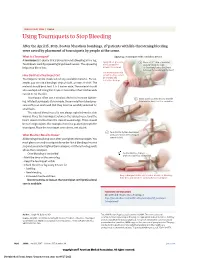
JAMA PATIENT PAGE | Trauma Using Tourniquets to Stop Bleeding After the April 15, 2013, Boston Marathon bombings, 27 patients with life-threatening bleeding were saved by placement of tourniquets by people at the scene. What Is a Tourniquet? Applying a tourniquet with a windlass device A tourniquet is a device that is placed around a bleeding arm or leg. Apply direct pressure 1 Place a 2-3” strip of material Tourniquets work by squeezing large blood vessels. The squeezing to the wound for about 2” from the edge helps stop blood loss. at least 15 minutes. of the wound over a long bone between the wound and the heart. Use a tourniquet only How Do I Put a Tourniquet On? when bleeding cannot be stopped and Tourniquets can be made out of any available material. For ex- is life threatening. ample, you can use a bandage, strip of cloth, or even a t-shirt. The material should be at least 2 to 3 inches wide. The material should also overlap itself. Using thin straps or material less than 2 inches wide can rip or cut the skin. Tourniquets often use a windlass device to increase tighten- 2 Insert a stick or other strong, straight ing. Inflated tourniquets (for example, those made from blood pres- item into the knot to act as a windlass. sure cuffs) can work well. But they must be carefully watched for small leaks. The injured blood vessel is not always right below the skin wound. Place the tourniquet between the injured vessel and the heart, about 2 inches from the closest wound edge. -

How to Evaluate Vaginal Bleeding and Discharge
How to Evaluate Vaginal Bleeding and Discharge Is the bleeding normal or abnormal? When does vaginal discharge reflect something as innocuous as irritation caused by a new soap? And when does it signal something more serious? The authors’ discussion of eight actual patient presentations will help you through the next differential diagnosis for a woman with vulvovaginal complaints. By Vincent Ball, MD, MAJ, USA, Diane Devita, MD, FACEP, LTC, USA, and Warren Johnson, MD, CPT, USA bnormal vaginal bleeding or discharge is typically due to either inadequate levels of estrogen one of the most common reasons women or a persistent corpus luteum. Structural causes of come to the emergency department.1,2 bleeding include leiomyomas, endometrial polyps, or Because the possible underlying causes malignancy. Infectious etiologies include pelvic in- Aare diverse, the patient’s age, key historical factors, flammatory disease (PID). Additionally, a variety of and a directed physical examination are instrumental bleeding dyscrasias involving platelet or clotting fac- in deciding on diagnosis and treatment. This article tors can complicate the normal menstrual period. Iat- will review some common case presentations of rogenic causes of vaginal bleeding include hormone nonpregnant female patients with abnormal vaginal replacement therapy, steroid hormone contraception, bleeding, inflammation, or discharge. and contraceptive intrauterine devices.3-5 Anovulatory bleeding is common in perimenar- ABNORMAL VAGINAL BLEEDING chal girls as a result of an immature hypothalamic- To ensure appropriate patient management, “Is she pituitary axis and in perimenopausal women due to pregnant?” should be the first question addressed, declining levels of estrogen. During reproductive since some vulvovaginal signs and symptoms will years, dysfunctional uterine differ in significance and urgency depending on the bleeding (DUB) is the most >>FAST TRACK<< answer. -

Abnormal Uterine Bleeding: a Management Algorithm
J Am Board Fam Med: first published as 10.3122/jabfm.19.6.590 on 7 November 2006. Downloaded from EVIDENCED-BASED CLINICAL MEDICINE Abnormal Uterine Bleeding: A Management Algorithm John W. Ely, MD, MSPH, Colleen M. Kennedy, MD, MS, Elizabeth C. Clark, MD, MPH, and Noelle C. Bowdler, MD Abnormal uterine bleeding is a common problem, and its management can be complex. Because of this complexity, concise guidelines have been difficult to develop. We constructed a concise but comprehen- sive algorithm for the management of abnormal uterine bleeding between menarche and menopause that was based on a systematic review of the literature as well as the actual management of patients seen in a gynecology clinic. We started by drafting an algorithm that was based on a MEDLINE search for rel- evant reviews and original research. We compared this algorithm to the actual care provided to a ran- dom sample of 100 women with abnormal bleeding who were seen in a university gynecology clinic. Discrepancies between the algorithm and actual care were discussed during audiotaped meetings among the 4 investigators (2 family physicians and 2 gynecologists). The audiotapes were used to revise the algorithm. After 3 iterations of this process (total of 300 patients), we agreed on a final algorithm that generally followed the practices we observed, while maintaining consistency with the evidence. In clinic, the gynecologists categorized the patient’s bleeding pattern into 1 of 4 types: irregular bleeding, heavy but regular bleeding (menorrhagia), severe acute bleeding, and abnormal bleeding associated with a contraceptive method. Subsequent management involved both diagnostic and treatment interven- tions, which often occurred simultaneously. -

Rare Case of Vaginal Bleeding with a Normal Vault Following Surgical Menopause”
Downloaded from www.medrech.com “Rare case of vaginal bleeding with a normal vault following surgical menopause” ISSN No. 2394-3971 Case Report RARE CASE OF VAGINAL BLEEDING WITH A NORMAL VAULT FOLLOWING SURGICAL MENOPAUSE Lakshmi Rathna Markhani, Nidhi Saluja, Swati Mothe Department of Obstetrics and Gynaecology, Nice Hospital for Women Children and Newborn,Hyderabad,India Submitted on: December 2016 Accepted on: January 2017 For Correspondence Email ID: Abstract Post Hysterectomy Causes of bleeding include atrophic vaginitis, vaginal vault granulation, prolapsed fallopian tube, cervical stump cancer, infiltrating ovarian tumors, estrogen secreting tumors in other parts of the body and rarely carcinoma of the fallopian tube. Endometriosis of the vault sometimes can cause postmenopausal bleeding. Post Hysterectomy complications at the vault site such as a bleeding incident can be commonly observed at a short-term post-operative period. Other delayed complications often occur as a hematoma, granuloma, keloid, incision hernia and or vascular formation at the vault. Many of these complications may be accompanied with bleeding symptoms. This case report describes persistent bleeding from vaginal vault 18 months following Hysterectomy. Keywords: Surgical menopause, Vaginal bleeding, Hysterectomy. Introduction Endometriosis has been described Endometriosis is defined as the presence of previously in case reports as a rare functional endometrial glands and stroma complication associated with Laparoscopic outside the usual location in the lining of the Hysterectomy and post abdominal surgery Uterine cavity(1-3). It occurs most (scar endometriosis (6).Post Hysterectomy commonly in the gynecologic organs and complications at the vault site such as a pelvic peritoneum but may frequently bleeding incident can be commonly involve the gastrointestinal system, greater observed at a short-term post-operative omentum, and surgical scars, while it is period. -

ER Guide to Bleeding Disorders
Bleeding disorders ER guide to bleeding disorders 1 Table of contents 4 General Guidelines 4–5 national Hemophilia Foundation guidelines 5–10 Treatment options 10 HemopHilia a Name:__________________________________________________________________________________________________ 10–11 national Hemophilia Foundation guidelines Address:________________________________________________________________________________________________ 12 dosage chart Phone:__________________________________________________________________________________________________ 14–15 Treatment products 16 HemopHilia B In case of emergency, contact: ______________________________________________________________________________ 16 national Hemophilia Foundation guidelines Relation to patient:________________________________________________________________________________________ 17 dosage chart 18 Treatment products 19 HemopHilia a or B with inHiBiTors Diagnosis: Hemophilia A: Mild Moderate Severe 20 national Hemophilia Foundation guidelines Inhibitors Inhibitors Bethesda units (if known) ____________________________________ 21 Treatment products Hemophilia B: Mild Moderate Severe 22–23 Von willeBrand disease Inhibitors Inhibitors Bethesda units (if known) ____________________________________ 23–24 national Hemophilia Foundation guidelines von Willebrand disease: Type 1 Type 2 Type 3 Platelet type 25 Treatment products 27 Bibliography Preferred product:_________________________________________________________________________________________ Dose for life-threatening -
Thrombocytopenia.Pdf
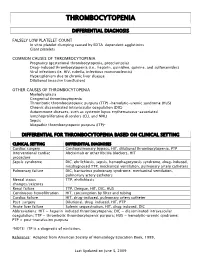
THROMBOCYTOPENIA DIFFERENTIAL DIAGNOSIS FALSELY LOW PLATELET COUNT In vitro platelet clumping caused by EDTA-dependent agglutinins Giant platelets COMMON CAUSES OF THROMBOCYTOPENIA Pregnancy (gestational thrombocytopenia, preeclampsia) Drug-induced thrombocytopenia (i.e., heparin, quinidine, quinine, and sulfonamides) Viral infections (ie. HIV, rubella, infectious mononucleosis) Hypersplenism due to chronic liver disease Dilutional (massive transfusion) OTHER CAUSES OF THROMBOCYTOPENIA Myelodysplasia Congenital thrombocytopenia Thrombotic thrombocytopenic purpura (TTP) -hemolytic-uremic syndrome (HUS) Chronic disseminated intravascular coagulation (DIC) Autoimmune diseases, such as systemic lupus erythematosus-associated lymphoproliferative disorders (CLL and NHL) Sepsis Idiopathic thrombocytopenic purpura (ITP)* DIFFERENTIAL FOR THROMBOCYTOPENIA BASED ON CLINICAL SETTING CLINICAL SETTING DIFFERENTIAL DIAGNOSES Cardiac surgery Cardiopulmonary bypass, HIT, dilutional thrombocytopenia, PTP Interventional cardiac Abciximab or other IIb/IIIa blockers, HIT procedure Sepsis syndrome DIC, ehrlichiosis, sepsis, hemophagocytosis syndrome, drug-induced, misdiagnosed TTP, mechanical ventilation, pulmonary artery catheters Pulmonary failure DIC, hantavirus pulmonary syndrome, mechanical ventilation, pulmonary artery catheters Mental status TTP, ehrlichiosis changes/seizures Renal failure TTP, Dengue, HIT, DIC, HUS Continuous hemofiltration HIT, consumption by filter and tubing Cardiac failure HIT, drug-induced, pulmonary artery catheter Post-surgery -

Colorectal-Vaginal Fistulas: Imaging and Novel Interventional Treatment Modalities
Journal of Clinical Medicine Review Colorectal-Vaginal Fistulas: Imaging and Novel Interventional Treatment Modalities M-Grace Knuttinen *, Johnny Yi ID , Paul Magtibay, Christina T. Miller, Sadeer Alzubaidi, Sailendra Naidu, Rahmi Oklu ID , J. Scott Kriegshauser and Winnie A. Mar ID Mayo Clinic Arizona; Phoenix, AZ 85054 USA; [email protected] (J.Y.); [email protected] (P.M.); [email protected] (C.T.M.); [email protected] (S.A.); [email protected] (S.N.); [email protected] (R.O.); [email protected] (J.S.K.); [email protected](W.A.M.) * Correspondence: [email protected]; Tel.: +480-342-1650 Received: 11 March 2018; Accepted: 16 April 2018; Published: 22 April 2018 Abstract: Colovaginal and/or rectovaginal fistulas cause significant and distressing symptoms, including vaginitis, passage of flatus/feces through the vagina, and painful skin excoriation. These fistulas can be a challenging condition to treat. Although most fistulas can be treated with surgical repair, for those patients who are not operative candidates, limited options remain. As minimally-invasive interventional techniques have evolved, the possibility of fistula occlusion has enriched the therapeutic armamentarium for the treatment of these complex patients. In order to offer optimal treatment options to these patients, it is important to understand the imaging and anatomical features which may appropriately guide the surgeon and/or interventional radiologist during pre-procedural planning. Keywords: colorectal-vaginal fistula; fistula; percutaneous fistula repair 1. Review of Current Literature on Vaginal Fistulas Vaginal fistulas account for some of the most distressing symptoms seen by clinicians today. The symptomatology of vaginal fistulas is related to the type of fistula; these include rectovaginal, anovaginal, colovaginal, enterovaginal, vesicovaginal, ureterovaginal, and urethrovaginal fistulas, with the two most common types reported as being vesicovaginal and rectovaginal [1]. -

ASCCP Clinical Practice Statement Evaluation of the Cervix in Patients with Abnormal Vaginal Bleeding Published: February 7, 2017
ASCCP Clinical Practice Statement Evaluation of the Cervix in Patients with Abnormal Vaginal Bleeding Published: February 7, 2017 All women presenting with abnormal vaginal bleeding should receive evaluation of the cervix and vagina, which should include at minimum visual inspection (speculum exam) and palpation (bimanual exam). If cervical or vaginal lesions are noted, appropriate tissue sampling is recommended, which can include Pap testing in addition to biopsy with or without colposcopy. These recommendations concur with those of ACOG Practice Bulletin #128 and Committee Opinion #557.1,2 The purpose of this article is to remind clinicians that Pap testing, as a form of tissue sampling, can be an important part of the workup of abnormal bleeding, and can be performed even if the patient is not due for her next screening test if there is clinical concern for cancer. Due to confusion amongst clinicians that has come to our attention, we wish to highlight the distinction between recommendations for diagnosis of cervical abnormalities including cancer amongst women with abnormal bleeding and recommendations for screening for cervical cancer amongst asymptomatic women. Screening guidelines recommend Pap testing at 3 year intervals for women ages 21-29, and Pap and HPV co-testing at 5 year intervals between the ages of 30-65 (with continued Pap testing at 3 year intervals as an option). These evidence- based guidelines are designed to maximize the detection of pre-cancer and minimize colposcopies. In addition, clinical practice guidelines no longer support routine pelvic examinations for cancer screening in asymptomatic women as this has not been shown to prevent cancer deaths.3,4,5 Consequently, physicians now perform fewer pelvic exams. -

The Woman with Postmenopausal Bleeding
THEME Gynaecological malignancies The woman with postmenopausal bleeding Alison H Brand MD, FRCS(C), FRANZCOG, CGO, BACKGROUND is a certified gynaecological Postmenopausal bleeding is a common complaint from women seen in general practice. oncologist, Westmead Hospital, New South Wales. OBJECTIVE [email protected]. This article outlines a general approach to such patients and discusses the diagnostic possibilities and their edu.au management. DISCUSSION The most common cause of postmenopausal bleeding is atrophic vaginitis or endometritis. However, as 10% of women with postmenopausal bleeding will be found to have endometrial cancer, all patients must be properly assessed to rule out the diagnosis of malignancy. Most women with endometrial cancer will be diagnosed with early stage disease when the prognosis is excellent as postmenopausal bleeding is an early warning sign that leads women to seek medical advice. Postmenopausal bleeding (PMB) is defined as bleeding • cancer of the uterus, cervix, or vagina (Table 1). that occurs after 1 year of amenorrhea in a woman Endometrial or vaginal atrophy is the most common cause who is not receiving hormone therapy (HT). Women of PMB but more sinister causes of the bleeding such on continuous progesterone and oestrogen hormone as carcinoma must first be ruled out. Patients at risk for therapy can expect to have irregular vaginal bleeding, endometrial cancer are those who are obese, diabetic and/ especially for the first 6 months. This bleeding should or hypertensive, nulliparous, on exogenous oestrogens cease after 1 year. Women on oestrogen and cyclical (including tamoxifen) or those who experience late progesterone should have a regular withdrawal bleeding menopause1 (Table 2). -

Ten Patient Stories Illustrating the Extraordinarily Diverse Clinical Features of Patients with Thrombotic Thrombocytopenic Purpura and Severe ADAMTS13 Deficiency
Journal of Clinical Apheresis 27:302–311 (2012) Ten Patient Stories Illustrating the Extraordinarily Diverse Clinical Features of Patients With Thrombotic Thrombocytopenic Purpura and Severe ADAMTS13 Deficiency James N. George,* Qiaofang Chen, Cassie C. Deford, and Zayd Al-Nouri Department of Biostatistics and Epidemiology, College of Public Health, Department of Medicine, College of Medicine, The University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma Patients with thrombotic thrombocytopenic purpura (TTP) and severe ADAMTS13 deficiency are often consid- ered to have typical clinical features. However, our experience is that there is extraordinary diversity of the pre- senting features and the clinical courses of these patients. This diversity is illustrated by descriptions of 10 patients. The patients illustrate that ADAMTS13 activity may be normal initially but severely deficient in subse- quent episodes. Patients with established diagnoses of systemic infection as the cause of their clinical features may have undetectable ADAMTS13 activity. Patients may have a prolonged prodrome of mild symptoms with only microangiopathic hemolytic anemia and thrombocytopenia or they may have the sudden onset of critical ill- ness with multiple organ involvement. Patients may die rapidly or recover rapidly; they may require minimal treatment or extensive and prolonged treatment. Patients may have acute and severe neurologic abnormalities before microangiopathic hemolytic anemia and thrombocytopenia occur. Patients may have concurrent TTP and systemic lupus erythematosus. Patients may have hereditary ADAMTS13 deficiency as the etiology of their TTP rather than acquired autoimmune ADAMTS13 deficiency. These patients’ stories illustrate the clinical spectrum of TTP with ADAMTS13 deficiency and emphasize the difficulties of clinical diagnosis. J. Clin.