Comparative Study of Red Blood Cell Morphology in Peripheral Smear and Automated Cell Counter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

20 Hemolytic Anemias Due to Abnormal Red Cell Enzymes
Hemolytic Anemias Due to Abnormal Red Cell Enzymes MODULE Hematology and Blood Bank Technique 20 HEMOLYTIC ANEMIAS DUE TO Notes ABNORMAL RED CELL ENZYMES 20.1 INTRODUCTION The main metabolic substrate for the RBCs is glucose. It is metabolized by two pathways: approximately 90% of the glucose is metabolized through the Embden Meyerhoff (glycolytic) pathway and the rest by the hexose monophosphate (HMP) pathway. In the Embden Meyerhoff (glycolytic) pathway glucose is metabolized to lactate through a series of enzymatic steps. Each molecule of glucose gives rise to 2 molecules of ATP. The ATP provides energy to maintain red cell volume, shape and flexibility. An ATP dependent pump in the red cell membrane actively keeps sodium out of the cell and potassium inside. The red cell has the enzymes that are needed for the glycolytic pathway. These enzymes help break down glucose to generate ATP which is the source of energy. About 10% of the glucose is diverted to the Hexose Monophosphate shunt pathway and this is essential for protection of red cells from oxidative stress. This pathway is necessary for the generation of NADPH which then reduces oxidized glutathione (GSSG) to reduced glutathione (GSH). GSH prevents the accumulation of H2O2 and the oxidation of hemoglobin to methemoglobin. When the level of GSH falls, H2O2 accumulates in the cell and oxidizes the hemoglobin to methemoglobin which becomes denatured and precipitates as Heinz bodies. These inclusions are rigid and attached to the red cell membrane and make the red cell susceptible to hemolysis. The NADPH required in this pathway is generated by the enzyme Glucose 6 phosphate dehydrogenase (G6PD). -

SEED Haematology Sysmex Educational Enhancement and Development October 2012
SEED Haematology Sysmex Educational Enhancement and Development October 2012 The red blood cell indices The full blood count has been used in conjunction with the traditional red The complete blood count (CBC) is central to clinical deci- cell indices in order to narrow down the possible causes sion making. This makes it one of the commonest laboratory of anaemia in an individual patient. investigations performed worldwide. Whilst the definition of what constitutes an CBC is influenced by the number Impedance technology and type of parameters measured by different haematology The RBC, HCT and MCV are all closely interrelated as they analysers, the traditional red cell indices that are widely are derived from information obtained from the passage used to classify anaemias are common to all. of cells through the aperture of the impedance channel of an automated haematology analyser. The impedance The laboratory approach to anaemia technology is based on the principle that an electrical field, Anaemia is an extremely common global healthcare prob- created between two electrodes of opposite charge, can lem. However, anaemia is merely a symptom which can be used to count and determine the size of cells. Blood result from a multitude of causes. Effective treatment is cells are poor conductors of electricity. The diluent in which only possible if the underlying cause is correctly identified. they are suspended as they pass through the aperture To this end, several classification systems have been devis- during counting is an isotonic solution which is a good ed. The most useful and widely used classification system conductor of electricity. -

The Widespread Application of Red Cell Survival Sive Red
CLINICAL DETERMINATION OF THE SITES OF RED CELL SEQUESTRATION IN HEMOLYTIC ANEMIAS1 By JAMES H. JANDL, MORTIMER S. GREENBERG, ROBERT H. YONEMOTO, AND WILLIAM B. CASTLE (From the Thorndike Memorial Laboratory and Second and Fourth (Harvard), Medical Services Boston City Hospital, and the Department of Medicine, Harvard Medical School, Boston, Mass.) (Submitted for publication January 30, 1956; accepted April 3, 1956) The widespread application of red cell survival greater than that of other tissues even when cor- techniques has revealed the importance of exces- rection was made for the Cr5l activity of the re- sive red cell destruction in the pathologic physi- sidual red cells. Moreover, the radioactivity of ology of many of the anemias. An increasing ar- the packed red cells removed from the spleen ex- ray of in vitro methods for detecting red cell or ceeded that of a comparable sample of packed red serum abnormalities has provided insight into the cells from the peripheral blood. In order to in- in vivo mechanisms underlying some of these proc- vestigate the possibility that Cr51-labelled red cell esses. In certain disease states the presence of deposition could be determined by measuring body visible or physically measurable alterations of the surface radioactivity, several questions required red cells has permitted detection of the sites and exploration: 1) Are the emanations of Cr5 suit- to some extent of the mechanisms of sequestration able for external body scanning at safe dosage of these cells. Such valuable observations have levels? 2) Does the site of tissue deposition of been made upon pathologic material from patients Cr65 following the intravenous injection of Cr51- with congenital hemolytic anemia (1-5) and labelled red cells necessarily indicate the site of sickle cell anemia (1, 5-7). -

Immunohematology JOURNAL of BLOOD GROUP SEROLOGY and EDUCATION
Immunohematology JOURNAL OF BLOOD GROUP SEROLOGY AND EDUCATION VOLUME 17, NUMBER 1, 2001 From the publishers of Immunohematology A Comprehensive Laboratory Manual Immunohematology Methods and Procedures Featuring— • Over 100 methods— just about every method used in a reference lab. • Eleven chapters discussing problems faced by blood group serologists and the procedures and methods that can be used to solve them. • An extra set of the methods to use at the bench, printed on durable waterproof paper. • See business reply order card enclosed in this issue or order on the Web at redcross.org/immunohematology Now available from Montgomery Scientific Publications APPLIED BLOOD GROUP SEROLOGY, 4th EDITION by Peter D. Issitt and David J. Anstee A totally revised, mostly rewritten, fully up-to-date edition of one of the most popular books about the blood groups and blood transfusion ever published. I 46 chapters, an increase of 16 over the third edition 1 ″× ″ • 1,208 plus xxiv 8 /2 11 pages, hardbound, fully indexed, over 1,500 entries I 260 tables and 112 figures, an increase of more than 60% over the third edition • Over 13,500 references, more than 5,000 are papers written since 1985 Prices; each includes shipping: USA $125.00; Canada/International $130.00 (surface mail); International $170.00 (air mail). ALL ORDERS MUST BE PREPAID (Check or Credit Card) in U.S. DOLLARS International orders by check drawn on a bank in the USA or by credit card please. Order from: Montgomery Scientific Publications, P.O. Box 2704, Durham, NC 27715, U.S.A. Credit card orders accepted by fax at (919) 489-1235 (No phone orders, please.) We accept VISA,MasterCard, and Discover Card. -

RBC Morphology Normal RBC Morphology
Dr.Iman Daham , BSci., MSc., PhD. Assist. Prof., Department of Internal and Preventive Medicine College of Veterinary Medicine, University of Mosul, Mosul, Iraq https://orcid.org/0000-0002-0947-7169 https://www.researchgate.net/profile/Iman Daham Clinical Pathology | Part I | 4th year 2019 RBC Morphology Normal RBC Morphology: Clinical Pathology | RBC Morphology | Dr. Iman Daham Page | 1 RED BLOOD CELL MORPHOLOGY Abnormal erythrocyte morphology is found in pathological states that may be : - abnormalities in size (anisocytosis). - In shape (poikilocytosis). -In hemoglobin content or the presence of inclusion bodies in erythrocyte. Hypochromic: A descriptive term applied to a red blood cell with a decreased concentration of hemoglobin. Normochromic: A descriptive term applied to a red blood cell with a normal concentration of hemoglobin. Normocytic: A descriptive term applied to normal size of RBC Macrocytic: A descriptive term applied to a larger than normal red blood cell. I-Variation in erythrocyte size (anisocytosis) 1-Microcytosis: Morphology: - Decrease in the red cell size. Red cells are smaller than ± 7µm in diameter. The nucleus of a small lymphocyte (± 8,µm) is a useful guide to the size of a red blood cell. Found in: - Iron deficiency anemia. - Thalassaemia. - Sideroblastic anemia. - Lead poisoning. - Anemia of chronic disease. Comment: Most erythrocytes presented in the picture are microcytes (compare with the small lymphocyte). The degree of hemoglobinization is sufficient. Normal platelets and single ovalocytes are present. Staining: MGG Magnification: x 1000 1. microcyte 2. normocyte 2-Macrocytosis: Morphology: Increase in the size of a red cell. Red cells are larger than 9µm in diameter. May be round or oval in shape, the diagnostic significance being different. -

Red Cell Agglutination in Non-Humans
Chapter 9 The Immune System: Red Cell Agglutination in Non-Humans Fred W. Quimby1 and Nancy V. Ridenour2 Cornell Veterinary College1 and Ithaca High School2 Ithaca, New York 14853 Fred is a Professor of Pathology at Cornell Medical and Cornell Veterinary Colleges. He received both V.M.D. and Ph.D. degrees from the University of Pennsylvania and later completed a post doctoral fellowship in Hematology at Tufts–New England Medical Center Hospital. Major research interests include immune system disorders of dogs and primates. He is a diplomate in the American College of Laboratory Animal Medicine, a member of the American Association of Veterinary Immunologists, and Executive Secretary of the World Veterinary Association Committee on Animal Welfare. He is the recipient of the Bernard F. Trum and Johnson and Johnson Focus Giving Awards and has authored more than 100 papers and is the editor of two books. Nancy is a biology teacher at Ithaca High School and instructor of Honors and Advanced Placement Biology courses. She received both B.S. and M.A.T. degrees from Cornell University. She has been actively involved in curriculum development including the production of a 70-exercise laboratory manual for Honors Biology. Involved in teacher education, Nancy has participated in all four semesters of the Cornell Institute for Biology Teachers. A recipient of the Bertha Bartholomew and Sigma Xi Awards and elected to the Committee on Biology Teacher Inservice Programs (National Research Council) and co-chairperson for “Prologue to Action, Life Sciences Education and Science Literacy” (sponsored by the U.S.P.H.S.). -

ISBT Science Series
Science Series INTRODUCTION TO BLOOD TRANSFUSION: FROM DONOR TO RECIPIENT rstar @pikisupe Join the conversation on social media with the hashtag #IntrotoBloodTransfusion ISBT Science Series Volume 15 Supplement 1 December 2020 Special issue: Introduction to Blood Transfusion: From Donor to Recipient CONTENTS Volume 15, Number S1, December 2020 Special issue: Introduction to Blood Transfusion: From Donor to Recipient List of contributors………………………………………………………………………….. ............................................................................................. 1 First Edition • Introduction .......................................................................................................................................................................................... 3 Second Edition • Introduction .......................................................................................................................................................................................... 4 • Preface ................................................................................................................................................................................................... 5 Abbreviations ........................................................................................................................................................................................... 6 Glossary ...................................................................................................................................................................................... -
Direct Antiglobulin (“Coombs”) Test-Negative Autoimmune Hemolytic Anemia: a Review
YBCMD-01786; No. of pages: 9; 4C: Blood Cells, Molecules and Diseases xxx (2013) xxx–xxx Contents lists available at ScienceDirect Blood Cells, Molecules and Diseases journal homepage: www.elsevier.com/locate/bcmd Direct antiglobulin (“Coombs”) test-negative autoimmune hemolytic anemia: A review George B. Segel a,b, Marshall A. Lichtman b,⁎ a Department of Pediatrics, University of Rochester Medical Center, 601 Elmwood Avenue, Rochester, NY 14642-0001, USA b Department of Medicine, 601 Elmwood Avenue, Rochester, NY 14642-0001, USA article info abstract Article history: We have reviewed the literature to identify and characterize reports of warm-antibody type, autoimmune hemo- Submitted 5 December 2013 lytic anemia in which the standard direct antiglobulin reaction was negative but a confirmatory test indicated Available online xxxx that the red cells were opsonized with antibody. Three principal reasons account for the absence of a positive direct antiglobulin test in these cases: a) IgG sensitization below the threshold of detection by the commercial (Communicated by M. Lichtman, M.D., antiglobulin reagent, b) low affinity IgG, removed by preparatory washes not conducted at 4 °C or at low ionic 5December2013) strength, and c) red cell sensitization by IgA alone, or rarely (monomeric) IgM alone, but not accompanied by fi Keywords: complement xation, and thus not detectable by a commercial antiglobulin reagent that contains anti-IgG and Autoimmune hemolytic anemia anti-C3. In cases in which the phenotype is compatible with warm-antibody type, -
Immunohematology JOURNAL of BLOOD GROUP SEROLOGY and EDUCATION
Immunohematology JOURNAL OF BLOOD GROUP SEROLOGY AND EDUCATION VOLUME 18, NUMBER 1, 2002 From the publishers of Immunohematology A Comprehensive Laboratory Manual Immunohematology Methods and Procedures Featuring— •Over 100 methods— just about every method used in a reference lab. • Eleven chapters discussing problems faced by blood group serologists and the procedures and methods that can be used to solve them. • An extra set of the methods to use at the bench, printed on durable waterproof paper. • See business reply order card enclosed in this issue or order on the Web at redcross.org/immunohematology Immunohematology JOURNAL OF BLOOD GROUP SEROLOGY AND EDUCATION VOLUME 18, NUMBER 1, 2002 CONTENTS 1 A review of the Knops blood group: separating fact from fallacy J.M. MOULDS 9 A gel microtyping system for diagnosis of paroxysmal nocturnal hemoglobinuria B. ZUPANSKA, B. BOGDANIK, AND H. PYL 13 Antibody screening in 37°C saline. Is it safe to omit it using the indirect antiglobulin (gel) test? J. DURAN AND M. FIGUEIREDO 16 Autoanti-D in a patient after cladribine treatment for lymphoplasmocytic lymphoma J. CID, V. BELTRAN, L. ESCODA, E. ELIES, AND C. MARTIN-VEGA 19 Warm autoimmune hemolytic anemia with mimicking anti-c and -E specificities H.-Y. HSIEH, D. MORONEY, D. NAUMANN, J. HATA, N. VOSNIDOU, R. KESSINGER, N. SHAHAB, N. HAKAMI, AND D. SMITH 23 COMMUNICATIONS Letters to the Editors Anti-cE (Rh27), a rarely occurring antibody G. LODI, D. RESCA, R. REVERBERI, AND M. GOVONI September 11 D. LONG Letter From the Editors Thoughts on September 11 24 24 ANNOUNCEMENTS ADVERTISEMENTS 26 INSTRUCTIONS FOR AUTHORS EDITOR-IN-CHIEF MANAGING EDITOR Delores Mallory, MT(ASCP)SBB Mary H. -
Assessment of Red Blood Cell Parameters and Peripheral Smear at Different Temperatures in Case of Cold Agglutination Disease
[Downloaded free from http://www.amhsr.org] Case Report Assessment of Red Blood Cell Parameters and Peripheral Smear at Different Temperatures in Case of Cold Agglutination Disease Gupta V Department of Pathology, UP Rural Institute of Medical Science and Research, Saifai, Etawah, Uttar Pradesh, India Address for correspondence: Abstract Dr. Vivek Gupta, Department of Pathology, UP Rural Cold agglutination disease (CAD) is characterized by an auto‑antibody which is able Institute of Medical Science and to agglutinate red blood cells (RBCs) at temperatures lower than that of the body, and Research, Saifai, Etawah ‑ 206 301, subsequently to activate the complement system responsible for lysis of RBCs. Patients show Uttar Pradesh, India. hemolytic anemia of varying degrees of severity, which arise or worsen upon exposure to E‑mail: [email protected] low temperatures. We describe a case who presented with fever and symptoms of asthenia. His investigations yielded bizarre RBC parameters which led to suspicion of a rare CAD, which was confirmed on reviewing RBC parameters, peripheral smear and direct Coomb’s test at different temperatures. Hence, we suggest assessment of bizarre RBC parameters and peripheral smear can help in laboratory testing and diagnosis of CAD. It should also not pose embarrassment in laboratory testing to the pathologist for making an early and accurate diagnosis, thus emphasizing the need for an early treatment of CAD. Keywords: Cold agglutination disease, Peripheral smear, Red blood cell parameters Introduction cell destruction by macrophages in the liver. Patients show hemolytic anemia of varying degrees of severity, as well as Cold agglutinins were first described by Landsteiner in episodes of hemoglobinuria and acrocyanosis, which arise or 1903.[1] Their pathological action against red blood cells (RBCs) worsen upon exposure to low temperatures. -
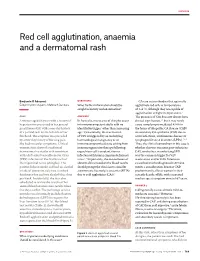
Red Cell Agglutination, Anaemia and a Dermatomal Rash
CLINICAL Red cell agglutination, anaemia and a dermatomal rash Benjamin O Adeyemi, QUESTION 2 CAs are autoantibodies that optimally Edeghonghon Olayemi, Mahinath Bandara What further information should be agglutinate red cells at temperatures sought in history and examination? of 3–4 °C, although they are capable of agglutination at higher temperatures.4 CASE ANSWER 1 The presence of CAs does not always have A woman aged 68 years with a history of In Australia, most cases of shingles occur clinical significance,3,5 but it may rarely hypertension presented to her general in immunocompetent adults with no cause complement-mediated AIHA in practitioner (GP) with a one-day history identifiable trigger1 other than increasing the forms of idiopathic CA disease (CAD) of a painful rash on the left side of her age.2 Occasionally, the reactivation or secondary CA syndrome (CAS) due to forehead. The eruption was preceded of VZV is triggered by an underlying acute infections, autoimmune disease or by a two-day history of burning pain. haematological malignancy or an lymphoproliferative disorders (LPDs).3,5,6 She had no ocular symptoms. Clinical immunocompromised state arising from Thus, the clinical conundrum in this case is examination showed a unilateral immunosuppressive therapy following whether this was transient post-infectious dermatomal vesicular rash consistent organ/stem cell transplantation or CAS, or whether an underlying LPD with a left-sided varicella-zoster virus infection with human immunodeficiency was the common trigger for VZV (VZV) infection of the first branch of virus.1,2 Importantly, the constellation of reactivation and/or CAS. Infectious the trigeminal nerve (shingles). -

Coeliac Disease, Vasculitis, and Cryoglobulinaemia
Gut: first published as 10.1136/gut.13.2.112 on 1 February 1972. Downloaded from Gut, 1972, 13, 112-123 Coeliac disease, vasculitis, and cryoglobulinaemia WILLIAM F. DOE, D. EVANS, J. R. HOBBS, AND C. C. BOOTH From the Departments of Medicine, Morbid Anatomy, and Chemical Pathology, Royal Postgraduate Medical School, London SUMMARY Four patients are described with the association of adult coeliac disease, vasculitis, and cryoglobulinaemia. In each patient the cryoglobulinaemia was of the mixed type consisting of more than one immunoglobulin class. It is suggested that the mixed cryoglobulins represent circulating immune complexes and that their deposition in small vessels causes the vasculitis. This is supported by immunofluorescent studies of skin biopsies from one of these patients. The significance of these findings in the four adult coeliac patients is discussed. There is increasing evidence implicating immune SERUM C3 LEVELS mechanisms in the pathogenesis of coeliac disease Serum C3 levels were measured by a Mancini plate (Taylor, Truelove, Thomson, and Wright, 1961; technique using goat antihuman C3 (Hyland Rubin, Fauci, Sleisenger, and Jefferies, 1965; Ketz, Laboratories). The levels in 20 healthy control Kantor, and Herskovic, 1968; Hobbs and Hepner, subjects ranged from 100 to 200 mg/100 ml. 1968; Booth, 1970; Soltoft, 1970). In recent years we have seen four patients with adult coeliac disease, HAEMOLYTIC COMPLEMENT vasculitis, and a mixed Such an cryoglobulinaemia. Total haemolytic complement was measured by the http://gut.bmj.com/ association prompts further speculation on the method of Mayer, Croft, and Gray (1948). Crossed immunological mystery of coeliac disease. This immunoelectrophoresis (Laurell, 1965) was used for paper describes the clinical, biochemical, and the detection of degradation products of com- immunological features of the four patients with this plement (C3) in fresh serum from two patients hitherto unreported association.