Peripheral Trigeminal Nerve Field Stimulation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Atypical & Idiopathic Facial Pain
ATYPICAL & IDIOPATHIC FACIAL PAIN Definition According to the International Association for the Study of Pain (IASP), chronic facial pain refers to symptoms which have been present for at least 6 months. ‘Atypical’ pain is a diagnosis of exclusion after other conditions have been considered and eliminated (i.e. it is idiopathic) and is characterized by chronic, constant pain in the absence of any apparent cause in the face or brain. Many information sources suggest that all ‘unexplained’ facial pains are termed Atypical Facial Pain but this is not the case. Categories of idiopathic facial pain conditions include Neuropathic Pain due to sensory nerve damage, Chronic Regional Pain Syndrome (CRPS) from sympathetic nerve damage and Atypical Facial Pain. Atypical odontalgia, or phantom tooth pain is a variation of atypical facial pain where intense discomfort is centered around a tooth or group of teeth with no obvious dental or oral disease. Epidemiology Atypical facial pain is more common in women than in men; most patients attending a facial pain clinic are women aged between 30 and 50 years. Although any area of the face can be involved, the most commonly affected area is the maxillary region. In the majority of patients there is no disease or other cause found. In a few patients the symptoms represent serious disease. In a small number of patients the pain may be one consequence of significant psychological or psychiatric disease. Clinical presentation Atypical facial pain is very variable in its presentation. Often it is characterized by continuous, daily pain of variable intensity. Typically, the pain is deep and poorly localized, is described as dull and aching, and does not waken the patient from sleep. -

Zeroing in on the Cause of Your Patient's Facial Pain
Feras Ghazal, DDS; Mohammed Ahmad, Zeroing in on the cause MD; Hussein Elrawy, DDS; Tamer Said, MD Department of Oral Health of your patient's facial pain (Drs. Ghazal and Elrawy) and Department of Family Medicine/Geriatrics (Drs. Ahmad and Said), The overlapping characteristics of facial pain can make it MetroHealth Medical Center, Cleveland, Ohio difficult to pinpoint the cause. This article, with a handy at-a-glance table, can help. [email protected] The authors reported no potential conflict of interest relevant to this article. acial pain is a common complaint: Up to 22% of adults PracticE in the United States experience orofacial pain during recommendationS F any 6-month period.1 Yet this type of pain can be dif- › Advise patients who have a ficult to diagnose due to the many structures of the face and temporomandibular mouth, pain referral patterns, and insufficient diagnostic tools. disorder that in addition to Specifically, extraoral facial pain can be the result of tem- taking their medication as poromandibular disorders, neuropathic disorders, vascular prescribed, they should limit disorders, or atypical causes, whereas facial pain stemming activities that require moving their jaw, modify their diet, from inside the mouth can have a dental or nondental cause and minimize stress; they (FIGURE). Overlapping characteristics can make it difficult to may require physical therapy distinguish these disorders. To help you to better diagnose and and therapeutic exercises. C manage facial pain, we describe the most common causes and underlying pathological processes. › Consider prescribing a tricyclic antidepressant for patients with persistent idiopathic facial pain. C Extraoral facial pain Extraoral pain refers to the pain that occurs on the face out- 2-15 Strength of recommendation (SoR) side of the oral cavity. -

Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic
anagem n M e ai n t P & f o M l e Journal of a d n i c r i u n o e J Pain Management & Medicine Tait et al., J Pain Manage Med 2017, 3:1 Review Article Open Access Chronic Orofacial Pain: Burning Mouth Syndrome and Other Neuropathic Disorders Raymond C Tait1, McKenzie Ferguson2 and Christopher M Herndon2 1Saint Louis University School of Medicine, St. Louis, USA 2Southern Illinois University Edwardsville School of Pharmacy, Edwardsville, USA *Corresponding author: RC Tait, Department of Psychiatry, Saint Louis University School of Medicine,1438 SouthGrand, Boulevard, St Louis, MO-63104, USA, Tel: 3149774817; Fax: 3149774879; E-mail: [email protected] Recevied date: October 4, 2016; Accepted date: January 17, 2017, Published date: January 30, 2017 Copyright: © 2017 Raymond C Tait, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Chronic orofacial pain is a symptom associated with a wide range of neuropathic, neurovascular, idiopathic, and myofascial conditions that affect a significant proportion of the population. While the collective impact of the subset of the orofacial pain disorders involving neurogenic and idiopathic mechanisms is substantial, some of these are relatively uncommon. Hence, patients with these disorders can be vulnerable to misdiagnosis, sometimes for years, increasing the symptom burden and delaying effective treatment. This manuscript first reviews the decision tree to be followed in diagnosing any neuropathic pain condition, as well as the levels of evidence needed to make a diagnosis with each of several levels of confidence: definite, probable, or possible. -

Trigeminal Nerve Block
Trigeminal Nerve Block Why use this treatment? This procedure is used for trigeminal neuralgia, described by many patients as one of the most painful afflictions known. TN sufferers experience sudden attacks of pain that are typically brief, but severe. TN pain occurs on only one side, involving the upper, middle and/or lower portions of the face. Attacks may come on without warning or be triggered by specific light stimulation in the affected area of the face. Common triggers include touch, talking, eating, drinking, chewing, tooth brushing, hair combing, water from a shower and even kissing. There are a number of causes for trigeminal neuralgia, including pressure from blood vessels on the trigeminal nerve, multiple sclerosis, brain tumors, or injury to the nerve from head trauma, dental or sinus trauma or from failed procedures that were intended to treat the neuralgia. TN pain after traumatic injury is usually constant aching or burning, but can also get worse with exposure to wind or cold. How does a trigeminal nerve block work? A trigeminal nerve block delivers steroids and/or local anesthetic directly into the space around the trigeminal nerve root. The area is bathed in the medicine. The injection is given to reduce inflammation and provide pain relief for several days to several months. How is the procedure done? You will be placed on an x-ray table and your skin will be cleansed and prepared. This procedure is performed under local anesthetic with light IV sedation. A needle is inserted into the skin beside the mouth, and directed through an opening at the base of the skull. -

Brain Structure and Function Related to Headache
Review Cephalalgia 0(0) 1–26 ! International Headache Society 2018 Brain structure and function related Reprints and permissions: sagepub.co.uk/journalsPermissions.nav to headache: Brainstem structure and DOI: 10.1177/0333102418784698 function in headache journals.sagepub.com/home/cep Marta Vila-Pueyo1 , Jan Hoffmann2 , Marcela Romero-Reyes3 and Simon Akerman3 Abstract Objective: To review and discuss the literature relevant to the role of brainstem structure and function in headache. Background: Primary headache disorders, such as migraine and cluster headache, are considered disorders of the brain. As well as head-related pain, these headache disorders are also associated with other neurological symptoms, such as those related to sensory, homeostatic, autonomic, cognitive and affective processing that can all occur before, during or even after headache has ceased. Many imaging studies demonstrate activation in brainstem areas that appear specifically associated with headache disorders, especially migraine, which may be related to the mechanisms of many of these symptoms. This is further supported by preclinical studies, which demonstrate that modulation of specific brainstem nuclei alters sensory processing relevant to these symptoms, including headache, cranial autonomic responses and homeostatic mechanisms. Review focus: This review will specifically focus on the role of brainstem structures relevant to primary headaches, including medullary, pontine, and midbrain, and describe their functional role and how they relate to mechanisms -

Clinical Anatomy of the Trigeminal Nerve
Clinical Anatomy of Trigeminal through the superior orbital fissure Nerve and courses within the lateral wall of the cavernous sinus on its way The trigeminal nerve is the fifth of to the trigeminal ganglion. the twelve cranial nerves. Often Ophthalmic Nerve is formed by the referred to as "the great sensory union of the frontal nerve, nerve of the head and neck", it is nasociliary nerve, and lacrimal named for its three major sensory nerve. Branches of the ophthalmic branches. The ophthalmic nerve nerve convey sensory information (V1), maxillary nerve (V2), and from the skin of the forehead, mandibular nerve (V3) are literally upper eyelids, and lateral aspects "three twins" carrying information of the nose. about light touch, temperature, • The maxillary nerve (V2) pain, and proprioception from the enters the middle cranial fossa face and scalp to the brainstem. through foramen rotundum and may or may not pass through the • The three branches converge on cavernous sinus en route to the the trigeminal ganglion (also called trigeminal ganglion. Branches of the semilunar ganglion or the maxillary nerve convey sensory gasserian ganglion), which contains information from the lower eyelids, the cell bodies of incoming sensory zygomae, and upper lip. It is nerve fibers. The trigeminal formed by the union of the ganglion is analogous to the dorsal zygomatic nerve and infraorbital root ganglia of the spinal cord, nerve. which contain the cell bodies of • The mandibular nerve (V3) incoming sensory fibers from the enters the middle cranial fossa rest of the body. through foramen ovale, coursing • From the trigeminal ganglion, a directly into the trigeminal single large sensory root enters the ganglion. -

A Review of the Mandibular and Maxillary Nerve Supplies and Their Clinical Relevance
AOB-2674; No. of Pages 12 a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 1 ) x x x – x x x Available online at www.sciencedirect.com journal homepage: http://www.elsevier.com/locate/aob Review A review of the mandibular and maxillary nerve supplies and their clinical relevance L.F. Rodella *, B. Buffoli, M. Labanca, R. Rezzani Division of Human Anatomy, Department of Biomedical Sciences and Biotechnologies, University of Brescia, V.le Europa 11, 25123 Brescia, Italy a r t i c l e i n f o a b s t r a c t Article history: Mandibular and maxillary nerve supplies are described in most anatomy textbooks. Accepted 20 September 2011 Nevertheless, several anatomical variations can be found and some of them are clinically relevant. Keywords: Several studies have described the anatomical variations of the branching pattern of the trigeminal nerve in great detail. The aim of this review is to collect data from the literature Mandibular nerve and gives a detailed description of the innervation of the mandible and maxilla. Maxillary nerve We carried out a search of studies published in PubMed up to 2011, including clinical, Anatomical variations anatomical and radiological studies. This paper gives an overview of the main anatomical variations of the maxillary and mandibular nerve supplies, describing the anatomical variations that should be considered by the clinicians to understand pathological situations better and to avoid complications associated with anaesthesia and surgical procedures. # 2011 Elsevier Ltd. -

Your Inner Fish
CHAPTER FIVE GETTING AHEAD It was two nights before my anatomy final and I was in the lab at around two in the morning, memorizing the cranial nerves. There are twelve cranial nerves, each branching to take bizarre twists and turns through the inside of the skull. To study them, we bisected the skull from forehead to chin and sawed open some of the bones of the cheek. So there I was, holding half of the head in each hand, tracing the twisted paths that the nerves take from our brains to the different muscles and sense organs inside. I was enraptured by two of the cranial nerves, the trigeminal and the facial. Their complicated pattern boiled down to something so simple, so outrageously easy that I saw the human head in a new way. That insight came from understanding the far simpler state of affairs in sharks. The elegance of my realization—though not its novelty; comparative anatomists had had it a century or more ago— and the pressure of the upcoming exam led me to forget where I was. At some point, I looked around. It was the middle of the night and I was alone in the lab. I also 108 happened to be surrounded by the bodies of twenty-five human beings under sheets. For the first and last time, I got the willies. I worked myself into such a lather that the hairs on the back of my neck rose, my feet did their job, and within a nanosecond I found myself at the bus stop, out of breath. -

Diagnosis and Treatment of Atypical Odontalgia: a Review of the Literature and Two Case Reports
Diagnosis and Treatment of Atypical Odontalgia: A Review of the Literature and Two Case Reports Abstract Aim: This report presents two cases diagnosed with atypical odontalgia (AO) and successfully treated with amitriptyline as well providing a review of the current literature on the subject. Results: The literature indicates the most important issue is an accurate differential diagnosis to distinguish between AO, pulpal pain, myofascial pain, and trigeminal neuralgia. Conclusion: Once the correct diagnosis is made the prognosis of AO is usually fair and the administration of tricyclic antidepressants often resolves symptoms. An effort should be made to avoid any unnecessary dental treatment that would only aggravate the problem. Keywords: Atypical odontalgia, AO, phantom tooth pain, differential diagnosis, treatment, amitriptyline, tricyclic antidepressants Citation: Melis M, Secci S. Diagnosis and Treatment of Atypical Odontalgia: A Review of the Literature and Two Case Reports. J Contemp Dent Pract 2007 March;(8)3:081-089. 1 The Journal of Contemporary Dental Practice, Volume 8, No. 3, March 1, 2007 Introduction Atypical odontalgia (AO) has been defined by signs are present, and anesthetic block of the Merskey1 as “severe throbbing pain in the tooth involved tooth provides equivocal results.2,9,18-20,26 without major pathology.” In fact the primary The pain also stops during sleep.9,18-20 symptom is pain, usually located in a tooth or a tooth site,2-9 that may spread with time involving The pathophysiology of AO is not clear, the entire maxilla or the mandible.2,4,6-10 The yet idiopathic,6,20,27-28 psychogenic,20,29-31 and pain is frequently continuous and persistent , neuropathic3,19-20,32 hypotheses have been but fluctuating in intensity4-5,7,11 with no signs of suggested. -
Lecture 6: Cranial Nerves
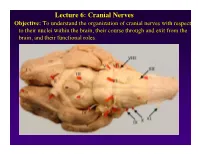
Lecture 6: Cranial Nerves Objective: To understand the organization of cranial nerves with respect to their nuclei within the brain, their course through and exit from the brain, and their functional roles. Olfactory Eye Muscles 3, 4 &6 Cranial Nerves 1-7 I overview Table, Page 49 II Lecture notes Cranial Nerves and their Functions V Trigeminal VII Facial VIII IX X XII XI Cranial Nerves 8-12 Overview sternocephalic I. Factors Responsible for the Complex Internal Organization of the Brain Stem-> leads to altered location of cranial nerve nuclei in adult brain stem 1. Development of the Fourth Ventricle a. Medulla and Pons develop ventral to the 4th ventricle cerebellum b. Alar plate is displaced lateral to basal plate 4 Medulla Developing Neural Tube 2. Cranial nerve nuclei form discontinuous columns Rostral 12 SE Page 48 Notes 3. Some cranial nerve nuclei migrate from their primitive embryonic positions (e.g., nuclei of V and VII) Facial N. Factors responsible for the complex internal organization of the brainstem: 4) Special senses develop in association with the brain stem. Nuclei of special senses 5) Development of the cerebellum and its connections Cerebellum II. Cranial Nerve Nuclei: Nucleus = column of neuron cell bodies. Efferent nuclei are composed of cell bodies of alpha or gamma motor neurons (SE) or preganglionic parasympathetic neurons (VE). III. Motor Efferent Nuclei (Basal Plate Derivatives): 1. SE (Somatic Efferent) Nuclei: SE neurons form two longitudinally oriented but discontinuous columns of cell bodies in the brain stem. Neurons that comprise these columns are responsible for innervating all of the skeletal musculature of the head. -

Therapeutic Potential of Stellate Ganglion Block in Orofacial Pain: a Mini Review
pISSN 2383-9309❚eISSN 2383-9317 Review Article J Dent Anesth Pain Med 2016;16(3):159-163❚http://dx.doi.org/10.17245/jdapm.2016.16.3.159 Therapeutic potential of stellate ganglion block in orofacial pain: a mini review Younghoon Jeon Department of Anesthesiology and Pain Medicine, School of Dentistry, Kyungpook National University, Daegu, Korea Orofacial pain is a common complaint of patients that causes distress and compromises the quality of life. It has many etiologies including trauma, interventional procedures, nerve injury, varicella-zoster (shingles), tumor, and vascular and idiopathic factors. It has been demonstrated that the sympathetic nervous system is usually involved in various orofacial pain disorders such as postherpetic neuralgia, complex regional pain syndromes, and atypical facial pain. The stellate sympathetic ganglion innervates the head, neck, and upper extremity. In this review article, the effect of stellate ganglion block and its mechanism of action in orofacial pain disorders are discussed. Keywords: Head; Orofacial; Pain; Stellate ganglion block; Sympathetic Nervous System. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. INTRODUCTION upper extremity. Stellate ganglion block (SGB) can dilate blood vessels in the head, neck, and upper extremities, resulting in an increased blood supply [6,7]. Preclinical Orofacial pain is a common complaint of patients that and clinical studies recently revealed that SGB induces causes distress and compromises the quality of life. -

Persistent Idiopathic Facial Pain
Chronic/ Persistent idiopathic facial pain Joanna M Zakrzewska MD Consultant / Honorary Professor Division of Diagnostic, Surgical and Medical Sciences Eastman Dental Hospital UCLH NHS Foundation Trust 256 Gray's Inn Road London WC1X 8LD UK Corresponding author Joanna M Zakrzewska Division of Diagnostic, Surgical and Medical Sciences Eastman Dental Hospital UCLH NHS Foundation Trust 256 Gray's Inn Road London WC1X 8LD [email protected] Tel. 020 3456 1195 Fax 020 3456 1105 1 Key words: facial pain, persistent idiopathic facial pain , cognitive behaviour therapy, antidepressants Synopsis Persistent or chronic idiopathic facial pain, often called atypical facial pain, is often used as a diagnosis of exclusion. It is a chronic pain in a non anatomically distributed area of the face and mouth which can be episodic or continuous and described as a nagging dull pain which at times is severe. It is associated with other chronic pain conditions, psychological abnormalities and significant life events. Investigations are all normal and early treatment can prevent chronicity. A multidisciplinary biopsychosocial approach with the use of antidepressants and cognitive behaviour therapy provides the best chance of pain relief and improved quality of life. Key points: 1. Persistent idiopathic facial pain is a poorly localised often continuous nagging pain of the face for which no cause as yet has been identified. 2. Patients are often over investigated in their quest to obtain a diagnosis and current conventional investigations are all normal. 3. Systematic reviews highlight the paucity of randomised controlled trials of high quality with a combination of antidepressant and cognitive behaviour therapy providing the best pain relief and decreased interference with life.