The Trigeminal and Facial Nerves the Facial and Blink
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
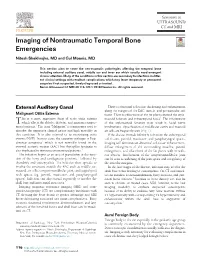
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD This section aims to cover the non-traumatic pathologies affecting the temporal bone including external auditory canal, middle ear and inner ear which usually need emergent clinical attention. Many of the conditions in this section are secondary to infections in differ- ent clinical settings with resultant complications which may leave temporary or permanent sequelae if not suspected, timely diagnosed or treated. Semin Ultrasound CT MRI 40:116-124 © 2018 Elsevier Inc. All rights reserved. External Auditory Canal There is abnormal soft tissue thickening and enhancement along the margins of the EAC, auricle, and periauricular soft Malignant Otitis Externa tissue. There is effacement of the fat planes around the stylo- his is a more aggressive form of acute otitis externa mastoid foramen and infratemporal fossa5. The involvement T which affects the elderly, diabetic, and immunocompro- of the stylomastoid foramen may result in facial nerve mised patients.1 The term “Malignant” is a misnomer used to involvement. Opacification of middle ear cavity and mastoid describe the aggressive clinical nature and high mortality in air cells are frequently seen (Fig. 1). this condition. It is also referred to as necrotizing otitis If the disease extends inferiorly to involve the subtemporal externa (NOE). In most cases, the causative pathogen is Pseu- soft tissues, parotid, masticator, and parapharyngeal spaces, domonas aeruginosa2 which is not normally found in the imaging will demonstrate abnormal soft tissue enhancement, external acoustic meatus (EAC) but Aspergillus fumigatus is diffuse enlargement of the surrounding muscles, parotid also implicated in immunocompromised patients.3 enlargement, and effacement of the fat planes with or with- The infection begins as an area of granulation at the junc- out abscess. -

Pharnygeal Arch Set - Motor USMLE, Limited Edition > Neuroscience > Neuroscience
CNs 5, 7, 9, 10 - Pharnygeal Arch Set - Motor USMLE, Limited Edition > Neuroscience > Neuroscience PHARYNGEAL ARCH SET, CNS 5, 7, 9, 10 • They are derived from the pharyngeal (aka branchial) arches • They have special motor and autonomic motor functions CRANIAL NERVES EXIT FROM THE BRAINSTEM CN 5, the trigeminal nerve exits the mid/lower pons.* CN 7, the facial nerve exits the pontomedullary junction.* CN 9, the glossopharyngeal nerve exits the lateral medulla.* CN 10, the vagus nerve exits the lateral medulla.* CRANIAL NERVE NUCLEI AT BRAINSTEM LEVELS Midbrain • The motor trigeminal nucleus of CN 5. Nerve Path: • The motor division of the trigeminal nerve passes laterally to enter cerebellopontine angle cistern. Pons • The facial nucleus of CN 7. • The superior salivatory nucleus of CN 7. Nerve Path: • CN 7 sweeps over the abducens nucleus as it exits the brainstem laterally in an internal genu, which generates a small bump in the floor of the fourth ventricle: the facial colliculus • Fibers emanate from the superior salivatory nucleus, as well. Medulla • The dorsal motor nucleus of the vagus, CN 10 • The inferior salivatory nucleus, CN 9 1 / 3 • The nucleus ambiguus, CNs 9 and 10. Nerve Paths: • CNs 9 and 10 exit the medulla laterally through the post-olivary sulcus to enter the cerebellomedullary cistern. THE TRIGEMINAL NERVE, CN 5  • The motor division of the trigeminal nerve innervates the muscles of mastication • It passes ventrolaterally through the cerebellopontine angle cistern and exits through foramen ovale as part of the mandibular division (CN 5[3]). Clinical Correlation - Trigeminal Neuropathy THE FACIAL NERVE, CN 7  • The facial nucleus innervates the muscles of facial expression • It spans from the lower pons to the pontomedullary junction. -

Facial Nerve Paralysis Due to Chronic Otitis Media: Prognosis in Restoration of Facial Function After Surgical Intervention
http://dx.doi.org/10.3349/ymj.2012.53.3.642 Original Article pISSN: 0513-5796, eISSN: 1976-2437 Yonsei Med J 53(3):642-648, 2012 Facial Nerve Paralysis due to Chronic Otitis Media: Prognosis in Restoration of Facial Function after Surgical Intervention Jin Kim,1* Gu-Hyun Jung,1* See-Young Park,1 and Won Sang Lee2 1Department of Otorhinolaryngology, Inje University College of Medicine, Goyang; 2Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. Received: December 21, 2010 Purpose: Facial paralysis is an uncommon but significant complication of chronic Revised: June 16, 2011 otitis media (COM). Surgical eradication of the disease is the most viable way to Accepted: July 6, 2011 overcome facial paralysis therefrom. In an effort to guide treatment of this rare Corresponding author: Dr. Won-Sang Lee, complication, we analyzed the prognosis of facial function after surgical treatment. Department of Otorhinolaryngology, Materials and Methods: A total of 3435 patients with COM, who underwent Yonsei University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, various otologic surgeries throughout a period of 20 years, were analyzed retro- Seoul 120-752, Korea. spectively. Forty six patients (1.33%) had facial nerve paralysis caused by COM. Tel: 82-2-2228-3606, Fax: 82-2-393-0580 We analyzed prognostic factors including delay of surgery, the extent of disease, E-mail: [email protected] presence or absence of cholesteatoma and the type of surgery affecting surgical outcomes. Results: Surgical intervention had a good effect on the restoration of *Jin Kim and Gu-Hyun Jung contributed equally to this work. -

Palatal Injection Does Not Block the Superior Alveolar Nerve Trunks: Correcting an Error Regarding the Innervation of the Maxillary Teeth
Open Access Review Article DOI: 10.7759/cureus.2120 Palatal Injection does not Block the Superior Alveolar Nerve Trunks: Correcting an Error Regarding the Innervation of the Maxillary Teeth Joe Iwanaga 1 , R. Shane Tubbs 2 1. Seattle Science Foundation 2. Neurosurgery, Seattle Science Foundation Corresponding author: Joe Iwanaga, [email protected] Abstract The superior alveolar nerves course lateral to the maxillary sinus and the greater palatine nerve travels through the hard palate. This difficult three-dimensional anatomy has led some dentists and oral surgeons to a critical misunderstanding in developing the anterior and middle superior alveolar (AMSA) nerve block and the palatal approach anterior superior alveolar (P-ASA) nerve block. In this review, the anatomy of the posterior, middle and anterior superior alveolar nerves, greater palatine nerve, and nasopalatine nerve are revisited in order to clarify the anatomy of these blocks so that the perpetuated anatomical misunderstanding is rectified. We conclude that the AMSA and P-ASA nerve blockades, as currently described, are not based on accurate anatomy. Categories: Anesthesiology, Medical Education, Other Keywords: anatomy, innervation, local anesthesia, maxillary nerve, nerve block, tooth Introduction And Background Anesthetic blockade of the posterior superior alveolar (PSA) branch of the maxillary nerve has played an important role in the endodontic treatment of irreversible acute pulpitis of the upper molar teeth except for the mesiobuccal root of the first molar tooth [1, 2]. This procedure requires precise anatomical knowledge of the pterygopalatine fossa and related structures in order to avoid unnecessary complications and to make the blockade most effective. The infraorbital nerve gives rise to middle superior alveolar (MSA) and anterior superior alveolar (ASA) branches. -

The Impact of Misdiagnosing Bell's Palsy As Acute Stroke
ORIGINAL RESEARCH ClinicalClinical Medicine Medicine 2019 2017 Vol Vol 19, 17, No No 5: 6:494–8 494–8 T h e i m p a c t o f m i s d i a g n o s i n g B e l l ’ s p a l s y a s a c u t e s t r o k e Authors: I s u r u I n d u r u w a , A N e g i n H o l l a n d , B R o s a l i n d G r e g o r y C a n d K a y v a n K h a d j o o i D Idiopathic Bell’s palsy can lead to a serious and, sometimes For many clinicians, acute stroke remains a concerning permanently, disfiguring and emotionally challenging facial diagnosis in patients presenting with facial palsy, but there are palsy. Early diagnosis and treatment with corticosteroids are key characteristics which facilitate differentiation of the two important, as they significantly improve recovery rates. Bell’s conditions, often without the need for further investigations. Our palsy is a benign condition that should be diagnosed and study aimed to explore whether clinicians could diagnose Bell’s ABSTRACT managed in primary care. Patients who self-present to the palsy in patients presenting with facial palsy at initial assessment emergency department should be managed and discharged and, if not, how often they sought a specialist opinion, as well as to without needing admission. -

Cranial Nerve Palsy
Cranial Nerve Palsy What is a cranial nerve? Cranial nerves are nerves that lead directly from the brain to parts of our head, face, and trunk. There are 12 pairs of cranial nerves and some are involved in special senses (sight, smell, hearing, taste, feeling) while others control muscles and glands. Which cranial nerves pertain to the eyes? The second cranial nerve is called the optic nerve. It sends visual information from the eye to the brain. The third cranial nerve is called the oculomotor nerve. It is involved with eye movement, eyelid movement, and the function of the pupil and lens inside the eye. The fourth cranial nerve is called the trochlear nerve and the sixth cranial nerve is called the abducens nerve. They each innervate an eye muscle involved in eye movement. The fifth cranial nerve is called the trigeminal nerve. It provides facial touch sensation (including sensation on the eye). What is a cranial nerve palsy? A palsy is a lack of function of a nerve. A cranial nerve palsy may cause a complete or partial weakness or paralysis of the areas served by the affected nerve. In the case of a cranial nerve that has multiple functions (such as the oculomotor nerve), it is possible for a palsy to affect all of the various functions or only some of the functions of that nerve. What are some causes of a cranial nerve palsy? A cranial nerve palsy can occur due to a variety of causes. It can be congenital (present at birth), traumatic, or due to blood vessel disease (hypertension, diabetes, strokes, aneurysms, etc). -

Maxillary Nerve-Mediated Postseptoplasty Nasal Allodynia: a Case Report
E CASE REPORT Maxillary Nerve-Mediated Postseptoplasty Nasal Allodynia: A Case Report Shikha Sharma, MD, PhD,* Wilson Ly, MD, PharmD,* and Xiaobing Yu, MD*† Endoscopic nasal septoplasty is a commonly performed otolaryngology procedure, not known to cause persistent postsurgical pain or hypersensitivity. Here, we discuss a unique case of persis- tent nasal pain that developed after a primary endoscopic septoplasty, which then progressed to marked mechanical and thermal allodynia following a revision septoplasty. Pain symptoms were found to be mediated by the maxillary division of the trigeminal nerve and resolved after percuta- neous radiofrequency ablation (RFA) of bilateral maxillary nerves. To the best of our knowledge, this is the first report of maxillary nerve–mediated nasal allodynia after septoplasty. (A&A Practice. 2020;14:e01356.) GLOSSARY CT = computed tomography; FR = foramen rotundum; HIPAA = Health Insurance Portability and Accountability Act; ION = infraorbital nerve; LPP = lateral pterygoid plate; MRI = magnetic reso- nance imaging; RFA = radiofrequency ablation; SPG = sphenopalatine ganglion; US = ultrasound ndoscopic nasal septoplasty is a common otolaryn- septoplasty for chronic nasal obstruction with resection of gology procedure with rare incidence of postsurgical the cartilage inferiorly and posteriorly in 2010. Before this Ecomplications. Minor complications include epistaxis, surgery, the patient only occasionally experienced mild septal hematoma, septal perforation, cerebrospinal fluid leak, headaches. However, his postoperative course was compli- and persistent obstruction.1 Numbness or hypoesthesia of the cated by significant pain requiring high-dose opioids. After anterior palate, secondary to injury to the nasopalatine nerve, discharge, patient continued to have persistent deep, “ach- has been reported, but is usually rare and temporary, resolv- ing” nasal pain which radiated toward bilateral forehead ing over weeks to months.2 Acute postoperative pain is also and incisors. -

Mandibular Fractures, Diagnostics, Postoperative Complications
Journal of Medical Sciences. March 23, 2020 - Volume 8 | Issue 13. Electronic-ISSN: 2345-0592 Medical Sciences 2020 Vol. 8 (13), p. 45-52 e-ISSN: 2345-0592 Medical Sciences Online issue Indexed in Index Copernicus Official website: www.medicsciences.com Mandibular fractures, diagnostics, postoperative complications Shahaf Givony1 1 Lithuanian University of Health Sciences. Academy of Medicine. Faculty of Odonthology. ABSTRACT Mandibular fractures usually happen among young males at the age of 16-30 years old. The mandible which has been rated as the second facial bone with the highest rate of injuries, tends to break much more often compared to any other bone of the cranium and represent up to 70% of the cases. This tendency to fracture may be explained by the protruded position, mobility and particular shape of it. The tendency for a mandibular fracture may also be explained by the common risk factors such as vehicle accidents and physical violence that are part of our daily life. There are many other risk factors according to the literature which differ between individuals due to the different socio-economic status, culture, technology and environment. Before the clinical examination of the fracture, it is obligatory to make sure that a clear airway path presents with no other fatal injuries. The examination may be supported by imaging methods which together will approve the diagnosis and method of treatment. Patients with a fracture of the mandible may suffer from post-operative complications which may occur after a short or long duration of the treatment. Those complications may be malocclusion, infections, trismus, damaged teeth and soft tissue, esthetic disfiguration, functional problems, pain and many more. -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -
Facial Nerve Disorders Cn7 (1)
FACIAL NERVE DISORDERS CN7 (1) Facial Nerve Disorders Last updated: January 18, 2020 FACIAL PALSY .......................................................................................................................................... 1 ETIOLOGY .............................................................................................................................................. 1 GUIDE TO LESION SITE LOCALIZATION ................................................................................................... 2 CLINICAL GRADING OF SEVERITY .......................................................................................................... 2 House-Brackmann grading scale ........................................................................................... 2 CLINICO-ANATOMICAL SYNDROMES ..................................................................................................... 2 Supranuclear (Central) Palsy ................................................................................................. 2 Nuclear Lesion ...................................................................................................................... 3 Cerebellopontine Angle Syndrome ....................................................................................... 3 Facial Canal Syndrome ......................................................................................................... 3 Stylomastoid Foramen Syndrome ........................................................................................ -

Neurophysiological Aspects of the Trigeminal Sensory System: an Update
Rev. Neurosci. 2018; 29(2): 115–123 Frederic Van der Cruyssen* and Constantinus Politis Neurophysiological aspects of the trigeminal sensory system: an update https://doi.org/10.1515/revneuro-2017-0044 Keywords: infraorbital; mandibular; neurophysiology; Received June 21, 2017; accepted July 20, 2017; previously published ophthalmic nerve; oral somatosensory functioning; online November 8, 2017 trigeminal sensory system. Abstract: The trigeminal system is one of the most complex cranial nerve systems of the human body. Research on it has vastly grown in recent years and concentrated more and more on molecular mechanisms and pathophysiology, Introduction but thorough reviews on this topic are lacking, certainly Knowledge about physiological aspects of the trigeminal on the normal physiology of the trigeminal sensory system. system today is largely based on animal models (Akerman Here we review the current literature on neurophysiology and Goadsby, 2015; Herta et al., 2017), cadaver studies of the trigeminal nerve from peripheral receptors up to its (Ezure et al., 2001; Williams et al., 2003) or extrapola- central projections toward the somatosensory cortex. We tions from peripheral nerve functioning. Human studies focus on the most recent scientific discoveries and describe are frequently limited to pathophysiology and lack proper historical relevant research to substantiate further. One study designs (Tanaka and Zhao, 2016; Goadsby et al., chapter on new insights of the pathophysiology of pain 2017). Neurophysiological research in this area is difficult at the level of the trigeminal system is added. A database due to the invasive character of most neurophysiological search of Medline, Embase and Cochrane was conducted tests, the small caliber of fibers, high density of receptors, with the search terms ‘animal study’, ‘neurophysiology’, cross-connections between different cranial nerves, dif- ‘trigeminal’, ‘oral’ and ‘sensory’. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists.