What Is Trigeminal Neuralgia? Trigeminal Neuralgia (TN) Is a Problem with Your Trigeminal Nerve That Causes Severe Facial Pain
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

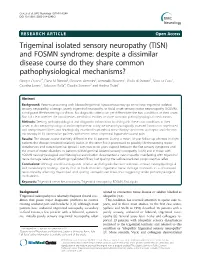
Hereditary Hypertrophic Neuropathy Combining Features of Tic Douloureux, Charcot- Marie-Tooth Disease, and Deafness
Hereditary hypertrophic neuropathy combining features of tic douloureux, Charcot- Marie-Tooth disease, and deafness Hereditary hypertrophic sensorimotor poly- neuropathy combining the features of Charcot- Marie-Tooth disease, trigeminal neuralgia, and Robert P. Cruse, D.O. deafness occurred through four generations of John P. Conomy, M.D. a family originating in Haywood County, North Asa J. Wilbourn, M.D. Carolina. Fourteen individuals had pes cavus, Maurice R. Hanson, M.D. distal muscle atrophy, depressed or absent mus- cle stretch reflexes, cutaneous sensory deficits, Department of Neurology and defective proprioception. Six family mem- bers had recurrent, lancinating, trigeminal pain, and seven were deaf. The family was brought under scrutiny when the propositus, a 60-year-old woman, was examined for treat- ment of tic douloureux. Neurologic informa- tion was ultimately obtained regarding 52 family members. No history of consanguinity could be ascertained within this kinship. The genealogy of the family we studied is presented in Figure 1. In addition to clinical neurologic examinations, electromyographic and nerve conduction stud- ies were obtained on those individuals indicated in the genealogy diagram. Audiometric studies were obtained when there was clinical indication of defective hearing. Quantitative cutaneous sensory testing was obtained in the propositus. 107 Downloaded from www.ccjm.org on October 1, 2021. For personal use only. All other uses require permission. 108 Cleveland Clinic Quarterly Vol. 44, No. 3 ' • CMT a TIC Deaf CMT He Examined MS f Died O Not Affected 0 D led before age onset (O Multiple normal d1 ond j si be. -1—i Two Marriages —Indicates number of slbs. -

Sciatica and Chronic Pain
Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh 123 Sciatica and Chronic Pain Robert W. Baloh Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh, MD Department of Neurology University of California, Los Angeles Los Angeles, CA, USA ISBN 978-3-319-93903-2 ISBN 978-3-319-93904-9 (eBook) https://doi.org/10.1007/978-3-319-93904-9 Library of Congress Control Number: 2018952076 © Springer International Publishing AG, part of Springer Nature 2019 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. -

Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies
17_Lupski 3/30/06 1:47 PM Page 243 NeuroMolecular Medicine Copyright © 2006 Humana Press Inc. All rights of any nature whatsoever reserved. ISSN0895-8696/06/08:243–254/$30.00 doi: 10.1385/NMM:8:1:243 REVIEW ARTICLE Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies Kinga Szigeti,1 Eva Nelis,2,3 and James R. Lupski*,1,4 1Departments of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX; 2Molecular Genetics, Flanders Interuniversity Institute for Biotechnology, Institute Born-Bunge, University of Antwerp, Antwerpen, Belgium; 3Laboratory of Neurogenetics, Institute Born-Borge, University of Antwerp, Antwerpen, Belgium; and 4Pediatrics, Baylor College of Medicine, and Texas Children Hospital, Houston, TX 77030 Received January 10, 2006; Revised January 13, 2006; Accepted January 13, 2006 Abstract DNAdiagnostics plays an important role in the characterization and management of patients manifesting inherited peripheral neuropathies. We describe the clinical integration of molecular diagnostics with medical history, physical examination, and electrophysiological studies. Mole- cular testing can help establish a secure diagnosis, enable genetic counseling regarding recurrence risk, potentially provide prognostic information, and in the near future may be important for the choice of therapies. doi: 10.1385/NMM:8:1:243 Index Entries:Molecular diagnostics; Charcot-Marie-Tooth disease; CMT; hereditary neuropathy with liability to pressure palsies; HNPP; Dejerine-Sottas neuropathy; DSN; congenital hypomyelinating neuropathy; CHN; CMT1A duplication; HNPP deletion. Introduction genetic testing, one needs to be familiar with the diagnostic tests available, choose the appropriate Molecular genetic diagnosis has become an inte- patients for testing, and utilize the diagnostic tools gral part of the evaluation of patients with hered- in a logical fashion to optimize the use of resources. -

ICD9 & ICD10 Neuromuscular Codes
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES ICD-9-CM ICD-10-CM Focal Neuropathy Mononeuropathy G56.00 Carpal tunnel syndrome, unspecified Carpal tunnel syndrome 354.00 G56.00 upper limb Other lesions of median nerve, Other median nerve lesion 354.10 G56.10 unspecified upper limb Lesion of ulnar nerve, unspecified Lesion of ulnar nerve 354.20 G56.20 upper limb Lesion of radial nerve, unspecified Lesion of radial nerve 354.30 G56.30 upper limb Lesion of sciatic nerve, unspecified Sciatic nerve lesion (Piriformis syndrome) 355.00 G57.00 lower limb Meralgia paresthetica, unspecified Meralgia paresthetica 355.10 G57.10 lower limb Lesion of lateral popiteal nerve, Peroneal nerve (lesion of lateral popiteal nerve) 355.30 G57.30 unspecified lower limb Tarsal tunnel syndrome, unspecified Tarsal tunnel syndrome 355.50 G57.50 lower limb Plexus Brachial plexus lesion 353.00 Brachial plexus disorders G54.0 Brachial neuralgia (or radiculitis NOS) 723.40 Radiculopathy, cervical region M54.12 Radiculopathy, cervicothoracic region M54.13 Thoracic outlet syndrome (Thoracic root Thoracic root disorders, not elsewhere 353.00 G54.3 lesions, not elsewhere classified) classified Lumbosacral plexus lesion 353.10 Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy 353.50 Neuralgic amyotrophy G54.5 Root Cervical radiculopathy (Intervertebral disc Cervical disc disorder with myelopathy, 722.71 M50.00 disorder with myelopathy, cervical region) unspecified cervical region Lumbosacral root lesions (Degeneration of Other intervertebral disc degeneration, -

Diagnosing and Treating Trigeminal Neuralgia in General Dentistry
general practice feature Chasing Pain Diagnosing and Treating Trigeminal Neuralgia in General Dentistry by Steven Olmos, DDS, DABCP, DABCDSM, DABDSM, DAAPM, FAAOP, FAACP, FICCMO, FADI, FIAO As dentists, we know quite a bit about tooth and gum pain, but when it comes to chronic facial pain and neuropathic pain, our dental school education leaves us unprepared. The objective of this article is to explain the differences between men and women with chronic orofacial pain and the relationship to proper functional breathing, using a case study as demonstration. 34 JANUARY 2016 // dentaltown.com general practice feature the United States, nearly half research published in Chest 2015 demonstrates that of all adults lived with chronic respiratory-effort-related arousal may be the most pain in 2011. Of 353,000 adults likely cause (nasal obstruction or mouth breath- 11 aged 18 years or older who were ing). Rising C02 (hypercapnia) in a patient with a surveyed by Gallup-Health- sleep-breathing disorder (including mouth breath- ways, 47 percent reported having at least one of ing) specifically stimulates the superficial masseter three types of chronic pain: neck or back pain, muscles to contract.12 knee or leg pain, or recurring pain.2 Identifying the structural area of obstruction A study published in The Journal of the Amer- (Four Points of Obstruction; Fig. 1) of the air- ican Dental Association October 2015 stated: way will insure the most effective treatment for a “One in six patients visiting a general dentist had sleep-breathing disorder and effectively reduce the experienced orofacial pain during the last year. -

Occipital Neuralgia: a Literature Review of Current Treatments from Traditional Medicine to CAM Treatments
Occipital Neuralgia: A Literature Review of Current Treatments from Traditional Medicine to CAM Treatments By Nikole Benavides Faculty Advisor: Dr. Patrick Montgomery Graduation: April 2011 1 Abstract Objective. This article provides an overview of the current and upcoming treatments for people who suffer from the signs and symptoms of greater occipital neuralgia. Types of treatments will be analyzed and discussed, varying from traditional Western medicine to treatments from complementary and alternative health care. Methods. A PubMed search was performed using the key words listed in this abstract. Results. Twenty-nine references were used in this literature review. The current literature reveals abundant peer reviewed research on medications used to treat this malady, but relatively little on the CAM approach. Conclusion. Occipital Neuralgia has become one of the more complicated headaches to diagnose. The symptoms often mimic those of other headaches and can occur post-trauma or due to other contributing factors. There are a variety of treatments that involve surgery or blocking of the greater occipital nerve. As people continue to seek more natural treatments, the need for alternative treatments is on the rise. Key Words. Occipital Neuralgia; Headache; Alternative Treatments; Acupuncture; Chiropractic; Nutrition 2 Introduction Occipital neuralgia is a type of headache that describes the irritation of the greater occipital nerve and the signs and symptoms associated with it. It is a difficult headache to diagnose due to the variety of signs and symptoms it presents with. It can be due to a post-traumatic event, degenerative changes, congenital anomalies, or other factors (10). The patterns of occipital neuralgia mimic those of other headaches. -
Trigeminal Isolated Sensory Neuropathy (TISN) and FOSMN
Cruccu et al. BMC Neurology (2014) 14:248 DOI 10.1186/s12883-014-0248-2 RESEARCH ARTICLE Open Access Trigeminal isolated sensory neuropathy (TISN) and FOSMN syndrome: despite a dissimilar disease course do they share common pathophysiological mechanisms? Giorgio Cruccu1*, Elena M Pennisi2, Giovanni Antonini3, Antonella Biasiotta1, Giulia di Stefano1, Silvia La Cesa1, Caterina Leone1, Salvatore Raffa4, Claudia Sommer5 and Andrea Truini1 Abstract Background: Patients presenting with bilateral trigeminal hypoesthesia may go on to have trigeminal isolated sensory neuropathy, a benign, purely trigeminal neuropathy, or facial-onset sensory motor neuronopathy (FOSMN), a malignant life-threatening condition. No diagnostic criteria can yet differentiate the two conditions at their onset. Nor is it clear whether the two diseases are distinct entities or share common pathophysiological mechanisms. Methods: Seeking pathophysiological and diagnostic information to distinguish these two conditions at their onset, in this neurophysiological and morphometric study we neurophysiologically assessed function in myelinated and unmyelinated fibres and histologically examined supraorbital nerve biopsy specimens with optic and electron microscopy in 13 consecutive patients with recent onset trigeminal hypoesthesia and pain. Results: The disease course distinctly differed in the 13 patients. During a mean 10 year follow-up whereas in eight patients the disease remained relatively stable, in the other five it progressed to possibly life-threatening motor disturbances and extra-trigeminal spread. From two to six years elapsed between the first sensory symptoms and the onset of motor disorders. In patients with trigeminal isolated sensory neuropathy (TISN) and in those with FOSMN neurophysiological and histological examination documented a neuronopathy manifesting with trigeminal nerve damage selectively affecting myelinated fibres, but sparing the Ia-fibre-mediated proprioceptive reflex. -

Occipital Neuralgia - Types of Headache/Migraine | American Migraine
Occipital Neuralgia - Types of Headache/Migraine | American Migraine ... http://www.americanmigrainefoundation.org/occipital-neuralgia/?print=y Occipital Neuralgia - Symptoms, Diagnosis, and Treatment Key Points: 1. Occipital neuralgia may be a cause of head pain originating in the occipital region (back of the head). 2. Pain is episodic, brief, severe, and shock-like. It originates from the occipital region and radiates along the course of the occipital nerves. 3. Attacks may be triggered by routine activities such as brushing the hair, moving the neck, or resting the head on a pillow. 4. Antiepileptic medications, tricyclic anti-depressants, and nerve blocks may be used for treatment. Introduction: Occipital neuralgia (ON) is a relatively rare primary headache disorder (primary headache disorders are not symptoms of or caused by another condition) affecting around 3.2/100,000 people per year.1 The term “neuralgia” refers to pain in the distribution of a nerve, in this case the occipital nerves. The greater, lesser, and third occipital nerves originate from the upper cervical nerve roots, course up the neck muscles, and exit near the base of the skull. These pure sensory nerves provide sensation to the back of the head, up to the top of the head, and behind the ears. The cause of ON is unknown; however, entrapment and irritation of the nerves have been proposed. Pain secondary to trauma such as whiplash injuries, inflammation, and compression of the occipital nerves by arteries or tumors have all been hypothesized, but no consensus has been reached. 1,2 ON may be provoked (triggered) simply by touching the affected region. -

Trigeminal Nerve Block
Trigeminal Nerve Block Why use this treatment? This procedure is used for trigeminal neuralgia, described by many patients as one of the most painful afflictions known. TN sufferers experience sudden attacks of pain that are typically brief, but severe. TN pain occurs on only one side, involving the upper, middle and/or lower portions of the face. Attacks may come on without warning or be triggered by specific light stimulation in the affected area of the face. Common triggers include touch, talking, eating, drinking, chewing, tooth brushing, hair combing, water from a shower and even kissing. There are a number of causes for trigeminal neuralgia, including pressure from blood vessels on the trigeminal nerve, multiple sclerosis, brain tumors, or injury to the nerve from head trauma, dental or sinus trauma or from failed procedures that were intended to treat the neuralgia. TN pain after traumatic injury is usually constant aching or burning, but can also get worse with exposure to wind or cold. How does a trigeminal nerve block work? A trigeminal nerve block delivers steroids and/or local anesthetic directly into the space around the trigeminal nerve root. The area is bathed in the medicine. The injection is given to reduce inflammation and provide pain relief for several days to several months. How is the procedure done? You will be placed on an x-ray table and your skin will be cleansed and prepared. This procedure is performed under local anesthetic with light IV sedation. A needle is inserted into the skin beside the mouth, and directed through an opening at the base of the skull. -

Brain Structure and Function Related to Headache
Review Cephalalgia 0(0) 1–26 ! International Headache Society 2018 Brain structure and function related Reprints and permissions: sagepub.co.uk/journalsPermissions.nav to headache: Brainstem structure and DOI: 10.1177/0333102418784698 function in headache journals.sagepub.com/home/cep Marta Vila-Pueyo1 , Jan Hoffmann2 , Marcela Romero-Reyes3 and Simon Akerman3 Abstract Objective: To review and discuss the literature relevant to the role of brainstem structure and function in headache. Background: Primary headache disorders, such as migraine and cluster headache, are considered disorders of the brain. As well as head-related pain, these headache disorders are also associated with other neurological symptoms, such as those related to sensory, homeostatic, autonomic, cognitive and affective processing that can all occur before, during or even after headache has ceased. Many imaging studies demonstrate activation in brainstem areas that appear specifically associated with headache disorders, especially migraine, which may be related to the mechanisms of many of these symptoms. This is further supported by preclinical studies, which demonstrate that modulation of specific brainstem nuclei alters sensory processing relevant to these symptoms, including headache, cranial autonomic responses and homeostatic mechanisms. Review focus: This review will specifically focus on the role of brainstem structures relevant to primary headaches, including medullary, pontine, and midbrain, and describe their functional role and how they relate to mechanisms -

Neuropathic Orofacial Pain the Brochure Is Provided Compliments Of
Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 1 Neuropathic orofacial paiN The brochure is provided compliments of This brochure in intended for informational purposes only and should be considered a replacement for a professional treatment for a health care professional. To locate knowledgeable and experienced expert in orofacial pain, contact: The American Academy of Orofacial Pain 174 S. New York Ave. POB 478 Oceanville, NJ 08231 P: 609-504-1311 E: [email protected] W: www.aaop.org To locate knowledgeable and experienced expert in Trigeminal Neuralgia, contact: Trigeminal Neuralgia Association 2801 SW Archer Road Gainesville, FL 32608 P: 352-376-9955 E: [email protected] W: www.tna-support.org Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 3 coNteNts 1-Neuropathic orofacial paiN 4-GettiNG help/What to expect 6-commoN Neuropathic orofacial paiN DisorDers aND their treatmeNt 6 - triGem iNal NeuralGia 8 - pre-triGem iNal NeuralGia 9 - atypical oDoNtalGia (phaNtom tooth paiN) 10 - chroNic reGioNal paiN syNDrome 12 - iN coNclusioN Neuropathic_Pain_Brochure_Neuropathic_Pain_Brochure 6/9/2010 11:41 AM Page 4 Neuropathic orofacial paiN Of the many pains that can effect the head and neck, perhaps the most confusing and difficult to diagnose are a group of maladies called Neuropathic Orofacial Pain Disorders. These neuropathic pain disorders are often chronic and arise from the brain and nerves of the head, face and neck. If you have experienced the frustration of having a toothache or face pain and, after seeing many doctors, still don't know where the pain is coming from, Brain you may be suffering from a neuropathic pain Spinal Cord disorder. -

Clinical Anatomy of the Trigeminal Nerve
Clinical Anatomy of Trigeminal through the superior orbital fissure Nerve and courses within the lateral wall of the cavernous sinus on its way The trigeminal nerve is the fifth of to the trigeminal ganglion. the twelve cranial nerves. Often Ophthalmic Nerve is formed by the referred to as "the great sensory union of the frontal nerve, nerve of the head and neck", it is nasociliary nerve, and lacrimal named for its three major sensory nerve. Branches of the ophthalmic branches. The ophthalmic nerve nerve convey sensory information (V1), maxillary nerve (V2), and from the skin of the forehead, mandibular nerve (V3) are literally upper eyelids, and lateral aspects "three twins" carrying information of the nose. about light touch, temperature, • The maxillary nerve (V2) pain, and proprioception from the enters the middle cranial fossa face and scalp to the brainstem. through foramen rotundum and may or may not pass through the • The three branches converge on cavernous sinus en route to the the trigeminal ganglion (also called trigeminal ganglion. Branches of the semilunar ganglion or the maxillary nerve convey sensory gasserian ganglion), which contains information from the lower eyelids, the cell bodies of incoming sensory zygomae, and upper lip. It is nerve fibers. The trigeminal formed by the union of the ganglion is analogous to the dorsal zygomatic nerve and infraorbital root ganglia of the spinal cord, nerve. which contain the cell bodies of • The mandibular nerve (V3) incoming sensory fibers from the enters the middle cranial fossa rest of the body. through foramen ovale, coursing • From the trigeminal ganglion, a directly into the trigeminal single large sensory root enters the ganglion.