1 INTRODUCTION the Information Contained in the Umpqua Health Alliance (UHA) Formulary and Its Appendices Is Provided for the Co
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Photoaging & Skin Damage
Use_for_Revised_OFC_Only_2006_PhotoagingSkinDamage 5/21/13 9:11 AM Page 2 PEORIA (309) 674-7546 MORTON (309) 263-7546 GALESBURG (309) 344-5777 PERU (815) 224-7400 NORMAL (309) 268-9980 CLINTON, IA (563) 242-3571 DAVENPORT, IA (563) 344-7546 SoderstromSkinInstitute.comsoderstromskininstitute.com FROMFrom YOUR Your DERMATOLOGISTDermatologist [email protected]@skinnews.com PHOTOAGING & SKIN DAMAGE Before You Worship The Sun Who’s At Risk? Today, many researchers and dermatologists Skin types that burn easily and tan rarely are believe that wrinkling and aging changes of the skin much more susceptible to the ravages of the sun on the are much more related to sun damage than to age! skin than are those that tan easily, rather than burn. Many of the signs of skin damage from the sun are Light complected, blue-eyed, red-haired people such as pictured on these pages. The decrease in the ozone Swedish, Irish, and English, are usually more suscep- layer, increasing the sun’s intensity, and the increasing tible to photo damage, and their skin shows the signs sun exposure among our population – through work, of photo damage earlier in life and in a more pro- sports, sunbathing and tanning parlors – have taken a nounced manner. Dark complexions give more protec- tremendous toll on our skin. Sun damage to the skin tion from light and the sun. ranks with other serious health dangers of smoking, alcohol, and increased cholesterol, and is being seen in younger and younger people. NO TAN IS A SAFE TAN! Table of Contents Sun Damage .............................................Pg. 1 Skin Cancer..........................................Pgs. 2-3 Mohs Micrographic Surgery ......................Pg. -

(12) United States Patent (10) Patent N0.: US 8,343,962 B2 Kisak Et Al
US008343962B2 (12) United States Patent (10) Patent N0.: US 8,343,962 B2 Kisak et al. (45) Date of Patent: *Jan. 1, 2013 (54) TOPICAL FORMULATION (58) Field of Classi?cation Search ............. .. 514/226.5, 514/334, 420, 557, 567 (75) Inventors: Edward T. Kisak, San Diego, CA (US); See application ?le fOr Complete Search history. John M. NeWsam, La Jolla, CA (US); _ Dominic King-Smith, San Diego, CA (56) References C‘ted (US); Pankaj Karande, Troy, NY (US); Samir Mitragotri, Goleta, CA (US) US' PATENT DOCUMENTS 5,602,183 A 2/1997 Martin et al. (73) Assignee: NuvoResearchOntano (CA) Inc., Mississagua, 6,328,979 2B1 12/2001 Yamashita et a1. 7,001,592 B1 2/2006 Traynor et a1. ( * ) Notice: Subject to any disclaimer, the term of this 7,795,309 B2 9/2010 Kisak eta1~ patent is extended or adjusted under 35 2002/0064524 A1 5/2002 Cevc U.S.C. 154(b) by 212 days. FOREIGN PATENT DOCUMENTS This patent is subject to a terminal dis- W0 WO 2005/009510 2/2005 claimer- OTHER PUBLICATIONS (21) APPI' NO‘, 12/848,792 International Search Report issued on Aug. 8, 2008 in application No. PCT/lB2007/0l983 (corresponding to US 7,795,309). _ Notice ofAlloWance issued on Apr. 29, 2010 by the Examiner in US. (22) Med Aug- 2’ 2010 Appl. No. 12/281,561 (US 7,795,309). _ _ _ Of?ce Action issued on Dec. 30, 2009 by the Examiner in US. Appl. (65) Prior Publication Data No, 12/281,561 (Us 7,795,309), Us 2011/0028460 A1 Feb‘ 3’ 2011 Primary Examiner * Raymond Henley, 111 Related U 5 Application Data (74) Attorney, Agent, or Firm * Foley & Lardner LLP (63) Continuation-in-part of application No. -

Late Stent Thrombosis After Paclitaxel-Eluting Stent Placement in a Patient with Essential Thrombocytosis
558 Türk Kardiyol Dern Arş - Arch Turk Soc Cardiol 2010;38(8):558-560 Late stent thrombosis after paclitaxel-eluting stent placement in a patient with essential thrombocytosis Esansiyel trombositozlu bir hastada paklitaksel salınımlı stent yerleştirme sonrası gelişen geç stent trombozu Telat Keleş, M.D., Nihal Akar Bayram, M.D., Tahir Durmaz, M.D., Engin Bozkurt, M.D. Department of Cardiology, Ankara Atatürk Education and Research Hospital, Ankara We report on a case of late stent thrombosis after drug- Bu yazıda, esansiyel trombositozlu bir hastada ilaç sa- eluting stent placement in a patient with essential throm- lınımlı stent yerleştirme sonrası gelişen geç stent trom- bocytosis. A 51-year-old male patient with a three-month bozu sunuldu. Üç ay önce sol ön inen artere paklitak- history of paclitaxel-eluting stent placement to the left sel salınımlı stent yerleştirilen 51 yaşındaki erkek hasta anterior descending artery presented with a complaint şiddetli retrosternal göğüs ağrısı yakınmasıyla başvur- of severe retrosternal chest pain. A high platelet count du. İki ay öncesinde hastanın trombosit sayımı yüksek (1,063,000/mm3) was detected two months prior to (1063000/mm3) bulunmuş ve durumu esansiyel trombo- presentation, which was interpreted as essential throm- sitoz olarak yorumlanmıştı. Hasta standart ikili antitrom- bocytosis. He was on standard dual antiplatelet therapy bosit tedavi (aspirin ve klopidogrel) görmekteydi. Elekt- (aspirin and clopidogrel). The electrocardiogram showed rokardiyografide V1-V6 derivasyonlarında ST-segment ST-segment elevation in leads V1-V6. Emergent coro- yükselmesi izlendi. Acil koroner anjiyografide paklitaksel nary angiography revealed thrombotic total occlusion salınımlı stent yerinde trombotik tam tıkanıklık gözlendi. at the location of the paclitaxel-eluting stent. -

(CD-P-PH/PHO) Report Classification/Justifica
COMMITTEE OF EXPERTS ON THE CLASSIFICATION OF MEDICINES AS REGARDS THEIR SUPPLY (CD-P-PH/PHO) Report classification/justification of medicines belonging to the ATC group D07A (Corticosteroids, Plain) Table of Contents Page INTRODUCTION 4 DISCLAIMER 6 GLOSSARY OF TERMS USED IN THIS DOCUMENT 7 ACTIVE SUBSTANCES Methylprednisolone (ATC: D07AA01) 8 Hydrocortisone (ATC: D07AA02) 9 Prednisolone (ATC: D07AA03) 11 Clobetasone (ATC: D07AB01) 13 Hydrocortisone butyrate (ATC: D07AB02) 16 Flumetasone (ATC: D07AB03) 18 Fluocortin (ATC: D07AB04) 21 Fluperolone (ATC: D07AB05) 22 Fluorometholone (ATC: D07AB06) 23 Fluprednidene (ATC: D07AB07) 24 Desonide (ATC: D07AB08) 25 Triamcinolone (ATC: D07AB09) 27 Alclometasone (ATC: D07AB10) 29 Hydrocortisone buteprate (ATC: D07AB11) 31 Dexamethasone (ATC: D07AB19) 32 Clocortolone (ATC: D07AB21) 34 Combinations of Corticosteroids (ATC: D07AB30) 35 Betamethasone (ATC: D07AC01) 36 Fluclorolone (ATC: D07AC02) 39 Desoximetasone (ATC: D07AC03) 40 Fluocinolone Acetonide (ATC: D07AC04) 43 Fluocortolone (ATC: D07AC05) 46 2 Diflucortolone (ATC: D07AC06) 47 Fludroxycortide (ATC: D07AC07) 50 Fluocinonide (ATC: D07AC08) 51 Budesonide (ATC: D07AC09) 54 Diflorasone (ATC: D07AC10) 55 Amcinonide (ATC: D07AC11) 56 Halometasone (ATC: D07AC12) 57 Mometasone (ATC: D07AC13) 58 Methylprednisolone Aceponate (ATC: D07AC14) 62 Beclometasone (ATC: D07AC15) 65 Hydrocortisone Aceponate (ATC: D07AC16) 68 Fluticasone (ATC: D07AC17) 69 Prednicarbate (ATC: D07AC18) 73 Difluprednate (ATC: D07AC19) 76 Ulobetasol (ATC: D07AC21) 77 Clobetasol (ATC: D07AD01) 78 Halcinonide (ATC: D07AD02) 81 LIST OF AUTHORS 82 3 INTRODUCTION The availability of medicines with or without a medical prescription has implications on patient safety, accessibility of medicines to patients and responsible management of healthcare expenditure. The decision on prescription status and related supply conditions is a core competency of national health authorities. -

May 2020 for Health Professionals Who Care for Cancer Patients
Systemic Therapy Update Volume 23 Issue 5 May 2020 For Health Professionals Who Care for Cancer Patients Inside This Issue: Editor’s Choice Benefit Drug List New Programs: Neoadjuvant Carboplatin for Triple-Negative New: BRLACTWAC, UGUPAPA, Pegaspargase (LKNOS, Breast Cancer (BRLACTWAC) | Apalutamide for Non- LYNOS), Bevacizumab (Pediatric), IGEV (Pediatric) | Metastatic Castration-Resistant Prostate Cancer (UGUPAPA) Deleted: GIGAVEOCAP, GIGAVEOF, SMAJIFN Drug Update NEW Protocols, PPPOs and Patient Handouts Pharmacare Update – Anticoagulants | Patient Assistance BR: BRLACTWAC | GU: UGUPAPA Programs REVISED Protocols, PPPOs and Patient Handouts Drug Shortages BR: BRAJAC, BRAJACT, BRAJACTG, BRAJACTT, BRAJACTTG, New: Alemtuzumab, Anagrelide | Updated: Hydroxyurea BRAJACTW, BRAJDAC, BRAJFEC, BRAJFECD, BRAJFECDT, Cancer Drug Manual© BRAVAC, BRLAACD, BRLAACDT, BRLATACG, BRLATWAC | New: Abemaciclib, Lurbinectedin | Revised: Apalutamide, GI: GIPGEMABR | GU: UGUPABI, UGUPENZ | LK: ULKBLIN, Durvalumab, Panitumumab, Pembrolizumab ULKMDSA | SA: SAIME | SC: SCDRUGRX | SM: USMAVDAB, ST Update Editorial Board USMAVDT, USMAVTRA, USMAVVC, USMAVVEM Membership Update Resources and Contact Information Editor’s Choice New Programs Effective 01 May 2020, the BC Cancer Provincial Systemic Therapy Program has approved the following new treatment programs. The full details of these programs can be found on the BC Cancer website in the Chemotherapy Protocols section. Breast Neoadjuvant Carboplatin for Locally Advanced, Triple-Negative Breast Cancer (BRLACTWAC) — The Provincial Systemic Therapy Program has approved the addition of carboplatin to the standard taxane- anthracycline neoadjuvant chemotherapy regimens, for patients with stage II and higher triple-negative breast cancer. This regimen consists of carboplatin (given every 3 weeks) in combination with weekly paclitaxel, followed by doxorubicin-cyclophosphamide (AC given every 2 or 3 weeks). Filgrastim support is available for the dose-dense AC option. -

A New Robust Technique for Testing of Glucocorticosteroids in Dogs and Horses Terry E
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 2007 A new robust technique for testing of glucocorticosteroids in dogs and horses Terry E. Webster Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Veterinary Toxicology and Pharmacology Commons Recommended Citation Webster, Terry E., "A new robust technique for testing of glucocorticosteroids in dogs and horses" (2007). Retrospective Theses and Dissertations. 15029. https://lib.dr.iastate.edu/rtd/15029 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. A new robust technique for testing of glucocorticosteroids in dogs and horses by Terry E. Webster A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Major: Toxicology Program o f Study Committee: Walter G. Hyde, Major Professor Steve Ensley Thomas Isenhart Iowa State University Ames, Iowa 2007 Copyright © Terry Edward Webster, 2007. All rights reserved UMI Number: 1446027 Copyright 2007 by Webster, Terry E. All rights reserved. UMI Microform 1446027 Copyright 2007 by ProQuest Information and Learning Company. All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code. ProQuest Information and Learning Company 300 North Zeeb Road P.O. Box 1346 Ann Arbor, MI 48106-1346 ii DEDICATION I want to dedicate this project to my wife, Jackie, and my children, Shauna, Luke and Jake for their patience and understanding without which this project would not have been possible. -

BC Cancer Benefit Drug List September 2021
Page 1 of 65 BC Cancer Benefit Drug List September 2021 DEFINITIONS Class I Reimbursed for active cancer or approved treatment or approved indication only. Reimbursed for approved indications only. Completion of the BC Cancer Compassionate Access Program Application (formerly Undesignated Indication Form) is necessary to Restricted Funding (R) provide the appropriate clinical information for each patient. NOTES 1. BC Cancer will reimburse, to the Communities Oncology Network hospital pharmacy, the actual acquisition cost of a Benefit Drug, up to the maximum price as determined by BC Cancer, based on the current brand and contract price. Please contact the OSCAR Hotline at 1-888-355-0355 if more information is required. 2. Not Otherwise Specified (NOS) code only applicable to Class I drugs where indicated. 3. Intrahepatic use of chemotherapy drugs is not reimbursable unless specified. 4. For queries regarding other indications not specified, please contact the BC Cancer Compassionate Access Program Office at 604.877.6000 x 6277 or [email protected] DOSAGE TUMOUR PROTOCOL DRUG APPROVED INDICATIONS CLASS NOTES FORM SITE CODES Therapy for Metastatic Castration-Sensitive Prostate Cancer using abiraterone tablet Genitourinary UGUMCSPABI* R Abiraterone and Prednisone Palliative Therapy for Metastatic Castration Resistant Prostate Cancer abiraterone tablet Genitourinary UGUPABI R Using Abiraterone and prednisone acitretin capsule Lymphoma reversal of early dysplastic and neoplastic stem changes LYNOS I first-line treatment of epidermal -

Xagrid, INN-Anagrelide
SCIENTIFIC DISCUSSION 1. Introduction Anagrelide hydrochloride monohydrate is a novel imidazoquinazoline originally developed as an inhibitor of platelet aggregation but subsequently found to have value as a platelet-lowering agent for the treatment of patients suffering from Essential thrombocythaemia (ET). ET is one of a number of chronic myeloproliferative disorders characterised by an elevated platelet count due to an autonomous clonal proliferation of bone marrow megakaryocytes. The underlying cause of this proliferation is unknown. Platelet function is generally normal and the cells are able to undergo aggregation and to participate in the haemostatic process in a more or less normal manner. The diagnosis is one of exclusion of reactive causes and other myeloproliferative disorders (MPDs) according to internationally agreed criteria of the Polycythaemia Vera Study Group (PVSG). The main criterion is a sustained platelet level of >600 x 109/L for more than two months. It is estimated that the prevalence of ET in the European Union (EU) is 2-3 per 10,000 persons. ET is a condition that may affect anyone at any stage of life from childhood although the median age of presentation is 60 years. Literature and clinical experience indicate a preponderance of female patients between the ages of 25 and 50 years. Up to two thirds of patients with ET are asymptomatic and a significant number of patients are now being diagnosed as an incidental consequence of the analysis of full blood counts for other health reasons. Generally, the older patient is more likely to be symptomatic at presentation, although younger patients may present with major complications. -

ER Guide to Bleeding Disorders
Bleeding disorders ER guide to bleeding disorders 1 Table of contents 4 General Guidelines 4–5 national Hemophilia Foundation guidelines 5–10 Treatment options 10 HemopHilia a Name:__________________________________________________________________________________________________ 10–11 national Hemophilia Foundation guidelines Address:________________________________________________________________________________________________ 12 dosage chart Phone:__________________________________________________________________________________________________ 14–15 Treatment products 16 HemopHilia B In case of emergency, contact: ______________________________________________________________________________ 16 national Hemophilia Foundation guidelines Relation to patient:________________________________________________________________________________________ 17 dosage chart 18 Treatment products 19 HemopHilia a or B with inHiBiTors Diagnosis: Hemophilia A: Mild Moderate Severe 20 national Hemophilia Foundation guidelines Inhibitors Inhibitors Bethesda units (if known) ____________________________________ 21 Treatment products Hemophilia B: Mild Moderate Severe 22–23 Von willeBrand disease Inhibitors Inhibitors Bethesda units (if known) ____________________________________ 23–24 national Hemophilia Foundation guidelines von Willebrand disease: Type 1 Type 2 Type 3 Platelet type 25 Treatment products 27 Bibliography Preferred product:_________________________________________________________________________________________ Dose for life-threatening -

Pre - PA Allowance Age 18 Years of Age Or Older Quantity 60 Grams Every 90 Days ______
DOXEPIN CREAM 5% (Prudoxin, Zonalon) Pre - PA Allowance Age 18 years of age or older Quantity 60 grams every 90 days _______________________________________________________________ Prior-Approval Requirements Age 18 years of age or older Diagnosis Patient must have the following: Moderate pruritus, due to atopic dermatitis (eczema) or lichen simplex chronicus AND the following: 1. Inadequate response, intolerance or contraindication to ONE medication in EACH of the following categories: a. Topical antihistamine (see Appendix I) b. High potency topical corticosteroid (see Appendix II) 2. Physician agrees to taper patient’s dose to the FDA recommended dose, and after tapered will only use for short-term pruritus relief (up to 8 days) a. Patients using over 60 grams of topical doxepin in 90 days be required to taper to 60 grams topical doxepin within 90 days Prior - Approval Limits Quantity 180 grams for 90 days Duration 3 months ___________________________________________________________________ Prior – Approval Renewal Requirements None (see appendix below) Doxepin 5% cream FEP Clinical Rationale DOXEPIN CREAM 5% (Prudoxin, Zonalon) APPENDIX I Drug Dosage Form Diphenhydramine Cream Phenyltoloxamine Lotion/ Cream Tripelennamine Cream Phendiamine Cream APPENDIX II Relative Potency of Selected Topical Corticosteroid Drug ProductsDosage Form Strength I. Very high potency Augmented betamethasone Ointment, Gel 0.05% dipropionate Clobetasol propionate Cream, Ointment 0.05% Diflorasone diacetate Ointment 0.05% Halobetasol propionate Cream, Ointment 0.05% II. High potency Amcinonide Cream, Lotion, 0.1% Augmented betamethasone Cream,Ointment Lotion 0.05% dipropionate Betamethasone Cream, Ointment 0.05% Betamethasonedipropionate valerate Ointment 0.1% Desoximetasone Cream, Ointment 0.25% Gel 0.05% Diflorasone diacetate Cream, Ointment 0.05% (emollient base) Fluocinonide Cream, Ointment, Gel 0.05% Halcinonide Cream, Ointment 0.1% Triamcinolone acetonide Cream, Ointment 0.5% III. -

Cloderm® Cream (Clocortolone Pivalate 0.1%): a Moisturizing, Hydrating Formulation Enhances Epidermal Barrier Function
CLINICAL INSIGHTS SUPPORTED BY PROMIUS PHARMA 2013, No. 2 Cloderm® Cream (clocortolone pivalate 0.1%): A Moisturizing, Hydrating Formulation Enhances Epidermal Barrier Function Leon Kircik, MD, FAAD It has been shown that application of some topical corti- DermResearch, PLLC, costeroids can increase TEWL and potentially contribute to Physicians Skin Care, PLLC, epidermal barrier dysfunction.6,7 In mice, application of topical Indiana University Medical Center, Indianapolis, IN, corticosteroids induced progressive increases in TEWL and a Mount Sinai Medical Center, New York, NY reduction in intercellular lipids in the SC.7 It is now well known The stratum corneum (SC) is a dynamic structure marked that even short-term use of topical corticosteroids can com- by multiple complex interactions and feedback loops.1-4 Self- promise epidermal barrier function and SC integrity by inhibit- repair of the permeability barrier has been documented; i.e., the ing epidermal lipid synthesis.8 However, certain formulations of SC can quickly adapt and initiate natural physiologic recovery. topical corticosteroids have been shown to improve skin hydra- Dysfunction of the SC is associated with specific disease states, tion and reduce TEWL.9,10 Perhaps the beneficial or detrimental perhaps most notably atopic dermatitis (AD), but also rosacea, effects of a given topical corticosteroid on TEWL have less to do psoriasis, and other inflammatory cutaneous disorders. More with the corticosteroid itself than with the vehicle in which it precisely, researchers and clinicians believe that AD may be is delivered.11 Thus, treatment becomes an act of balancing the driven in part by poor epidermal barrier function, perhaps as negative effects of the corticosteroid molecule itself on epider- a result of impairments in the permeability, immune response, mal barrier versus the positive impact of the vehicle that deliv- and antimicrobial barriers. -
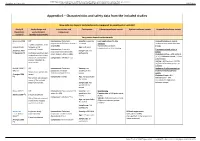
Appendix 6 – Characteristics and Safety Data from the Included Studies
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Open Appendix 6 – Characteristics and safety data from the included studies How safe are topical corticosteroids compared to emollient or vehicle? Study ID Study design and Intervention and Participants Cutaneous adverse events Systemic adverse events Unspecified adverse events (Systematic study duration comparator review*) (Quality assessment) Very potent topical corticosteroids Breneman 2003 RCT Intervention: Clobetasol Severity: moderate Local application site skin Unspecified adverse events (1) propionate 0.05% lotion (twice a to severe reactions Incidence comparable between 2 weeks treatment, then day) (n=96) No clinically significant groups. (unpublished) followed up for Age: ≥ 12 years telangiectasia or skin thinning additional 2 weeks Intervention: Clobetasol Treatment-related adverse (Feldman 2005 Sample size: 229 propionate 0.05% emollient events (2) Nankervis (3)) Cochrane risk of bias tool: participants cream (twice a day) (n=100) Clobetasol lotion = 4/96 patients randomisation described, (4.2%); Clobetasol cream = 1/100 allocation concealment Comparator: Vehicle (n=33) patients (1%) unclear, intention-to- Vehicle = 6/33 patients (18.2%) treat unclear. (Difference between groups: p= 0.0006a) Kimball 2008 (4) RCT Intervention: Clobetasol Severity: not Incidence of adverse events or (trial a) propionate emulsion specified in the treatment related adverse Duration not specified in formulation foam 0.05% review events (Frangos 2008 review Clobetasol foam = 8% (5)) Comparator: Vehicle Age: not specified in Risk of bias not assessed Vehicle foam = 10% the review in any of the included (no significant differences systematic reviews.