Cloderm® Cream (Clocortolone Pivalate 0.1%): a Moisturizing, Hydrating Formulation Enhances Epidermal Barrier Function
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(CD-P-PH/PHO) Report Classification/Justifica
COMMITTEE OF EXPERTS ON THE CLASSIFICATION OF MEDICINES AS REGARDS THEIR SUPPLY (CD-P-PH/PHO) Report classification/justification of medicines belonging to the ATC group D07A (Corticosteroids, Plain) Table of Contents Page INTRODUCTION 4 DISCLAIMER 6 GLOSSARY OF TERMS USED IN THIS DOCUMENT 7 ACTIVE SUBSTANCES Methylprednisolone (ATC: D07AA01) 8 Hydrocortisone (ATC: D07AA02) 9 Prednisolone (ATC: D07AA03) 11 Clobetasone (ATC: D07AB01) 13 Hydrocortisone butyrate (ATC: D07AB02) 16 Flumetasone (ATC: D07AB03) 18 Fluocortin (ATC: D07AB04) 21 Fluperolone (ATC: D07AB05) 22 Fluorometholone (ATC: D07AB06) 23 Fluprednidene (ATC: D07AB07) 24 Desonide (ATC: D07AB08) 25 Triamcinolone (ATC: D07AB09) 27 Alclometasone (ATC: D07AB10) 29 Hydrocortisone buteprate (ATC: D07AB11) 31 Dexamethasone (ATC: D07AB19) 32 Clocortolone (ATC: D07AB21) 34 Combinations of Corticosteroids (ATC: D07AB30) 35 Betamethasone (ATC: D07AC01) 36 Fluclorolone (ATC: D07AC02) 39 Desoximetasone (ATC: D07AC03) 40 Fluocinolone Acetonide (ATC: D07AC04) 43 Fluocortolone (ATC: D07AC05) 46 2 Diflucortolone (ATC: D07AC06) 47 Fludroxycortide (ATC: D07AC07) 50 Fluocinonide (ATC: D07AC08) 51 Budesonide (ATC: D07AC09) 54 Diflorasone (ATC: D07AC10) 55 Amcinonide (ATC: D07AC11) 56 Halometasone (ATC: D07AC12) 57 Mometasone (ATC: D07AC13) 58 Methylprednisolone Aceponate (ATC: D07AC14) 62 Beclometasone (ATC: D07AC15) 65 Hydrocortisone Aceponate (ATC: D07AC16) 68 Fluticasone (ATC: D07AC17) 69 Prednicarbate (ATC: D07AC18) 73 Difluprednate (ATC: D07AC19) 76 Ulobetasol (ATC: D07AC21) 77 Clobetasol (ATC: D07AD01) 78 Halcinonide (ATC: D07AD02) 81 LIST OF AUTHORS 82 3 INTRODUCTION The availability of medicines with or without a medical prescription has implications on patient safety, accessibility of medicines to patients and responsible management of healthcare expenditure. The decision on prescription status and related supply conditions is a core competency of national health authorities. -

Clinical Policy: Topical Agents: Corticosteroids
Clinical Policy: Topical Agents: Corticosteroids Reference Number: OH.PHAR.PPA.92 Effective Date: 01/01/2020 Revision Log Last Review Date: Line of Business: Medicaid See Important Reminder at the end of this policy for important regulatory and legal information. Description TOPICAL AGENTS: CORTICOSTEROIDS – LOW POTENCY NO PA REQUIRED “PREFERRED” PA REQUIRED “NON- PREFERRED” DESONIDE cream, ointment (generic of Desowen®) ALCLOMETASONE cream, ointment (generic of FLUOCINOLONE ACETONIDE 0.01% cream, solution Aclovate®) (generic of Synalar®) CAPEX® shampoo (fluocinolone acetonide) FLUOCINOLONE body oil, scalp oil (generic of Derma- DESONATE®gel (desonide) Smoothe/ FS®) DESONIDE lotion (generic of Desowen®) HYDROCORTISONE cream, lotion, ointment HYDROCORTISONE ACETATE WITH ALOE gel HYDROCORTISONE WITH UREA cream (generic of Carmol HC®) PANDEL® cream (hydrocortisone probutate) PEDIADERM HC® kit TOPICAL AGENTS: CORTICOSTEROIDS – MEDIUM POTENCY NO PA REQUIRED “PREFERRED” PA REQUIRED “NON--PREFERRED” BETAMETHASONE DIPROPIONATE-CALCIPOTRIENE BETAMETHASONE DIPROPIONATE lotion (generic of Ointment Diprolene®) BETAMETHASONE VALERATE cream, lotion (generic of CLOCORTOLONE PIVALATE (generic of Cloderm®) Valisone®) CORDRAN® tape (flurandrenolide) FLUTICASONE PROPIONATE cream, ointment (generic of DESOXIMETASONE cream, gel, ointment (generic of Cutivate®) Topicort®) MOMETASONE FUROATE cream, ointment, solution FLUOCINOLONE ACETONIDE 0.025% cream, ointment (generic of Elocon®) (generic of Synalar®) PREDNICARBATE cream (generic of Dermatop®) FLUTICASONE -

Steroids Topical
Steroids, Topical Therapeutic Class Review (TCR) September 18, 2020 No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, digital scanning, or via any information storage or retrieval system without the express written consent of Magellan Rx Management. All requests for permission should be mailed to: Magellan Rx Management Attention: Legal Department 6950 Columbia Gateway Drive Columbia, Maryland 21046 The materials contained herein represent the opinions of the collective authors and editors and should not be construed to be the official representation of any professional organization or group, any state Pharmacy and Therapeutics committee, any state Medicaid Agency, or any other clinical committee. This material is not intended to be relied upon as medical advice for specific medical cases and nothing contained herein should be relied upon by any patient, medical professional or layperson seeking information about a specific course of treatment for a specific medical condition. All readers of this material are responsible for independently obtaining medical advice and guidance from their own physician and/or other medical professional in regard to the best course of treatment for their specific medical condition. This publication, inclusive of all forms contained herein, is intended to be educational in nature and is intended to be used for informational purposes only. Send comments and suggestions to [email protected]. September -

Medication List
Medication List Walgreens Plus™ members receive discounts on thousands of generic and brand-name medications included on this Medication List, which is divided into two sections, “Value Priced” Medications and “Discounted” Medications*. The price for a medication identified as “Value-Priced” is listed below: Get savings up to 85% off Cash Prices • 30-day-supply drugs cost $5 (tier 1), $10 (tier 2) or $15 (tier 3) on Atorvastatin (generic Lipitor) and • 90-day-supply drugs cost $10 (tier 1), $20 (tier 2) or $30 (tier 3) Rosuvastatin (generic Crestor) †† The Discounted Medications section lists the discounts offered to Walgreens Plus members on other generic and brand-name medications not included in the Value-Priced Medication section. The price for a medication is based on its tier and whether it is a 30-day or 90-day supply†. There may be an additional cost for quanities greater than those listed. This discount prescription pricing applies only to Walgreen Plus members on prescriptions purchased in select Walgreens stores that are not billed to insurance and/or used in combination with other health or pharmacy benefit programs. For further details, see your pharmacist or Walgreens.com/Plus. VALUE GENERICS NAPROXEN 250MG TAB 2 60 180 Antifungal NAPROXEN 500MG TAB 2 60 180 Quantity NAPROXEN 375MG TAB 2 60 180 Drug Name Tier 30 90 NAPROXEN DR 500MG TAB 3 60 180 FLUCONAZOLE 150MG TAB 2 1 3 TERBINAFINE 250MG TAB 2 30 90 Asthma Quantity Antiviral Drug Name Tier 30 90 Quantity ALBUTEROL 0.083% INH SOLN 25X3ML 2 75 225 Drug Name Tier 30 90 AMINOPHYLLINE -

A New Robust Technique for Testing of Glucocorticosteroids in Dogs and Horses Terry E
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 2007 A new robust technique for testing of glucocorticosteroids in dogs and horses Terry E. Webster Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Veterinary Toxicology and Pharmacology Commons Recommended Citation Webster, Terry E., "A new robust technique for testing of glucocorticosteroids in dogs and horses" (2007). Retrospective Theses and Dissertations. 15029. https://lib.dr.iastate.edu/rtd/15029 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. A new robust technique for testing of glucocorticosteroids in dogs and horses by Terry E. Webster A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Major: Toxicology Program o f Study Committee: Walter G. Hyde, Major Professor Steve Ensley Thomas Isenhart Iowa State University Ames, Iowa 2007 Copyright © Terry Edward Webster, 2007. All rights reserved UMI Number: 1446027 Copyright 2007 by Webster, Terry E. All rights reserved. UMI Microform 1446027 Copyright 2007 by ProQuest Information and Learning Company. All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code. ProQuest Information and Learning Company 300 North Zeeb Road P.O. Box 1346 Ann Arbor, MI 48106-1346 ii DEDICATION I want to dedicate this project to my wife, Jackie, and my children, Shauna, Luke and Jake for their patience and understanding without which this project would not have been possible. -

A List of Medications That May Lower Your Patients' Costs
A list of medications that may lower your patients’ costs INTRODUCTION Catamaran utilizes a Pharmacy and Therapeutics Committee (P & T Committee), made up of practicing physicians, pharmacists, and nurses to help ensure that our formulary is medically sound and that it supports patient health. This committee reviews and evaluates medications on the formulary based on safety and efficacy to help maintain clinical integrity in all therapeutic categories. FORMULARY DESIGN There are numerous formulary designs that can be used by a pharmacy benefits administrator. Catamaran has chosen a formulary structure which is open and incentive based. Open Formulary: features co‐payments for medications that are preferred and non‐ preferred brands, plus lower co‐payments for generic drugs. Incentive Based: features different co‐payments for medications that are on or off the formulary. In this type of formulary, the patient cost structure may be two‐tier, three‐ tier, or four‐tier design. USING THIS FORMULARY REFERENCE GUIDE TO HELP CONTAIN COSTS Many benefit sponsors use the Catamaran formulary to help manage the overall cost of providing prescription drug benefits. This formulary offers a wide range of medications from which to choose. We realize that this formulary reference guide may not include every drug from every manufacturer. However, choosing a preferred drug when it is appropriate can provide access to the necessary medications to stay healthy, at a cost that is more affordable. KNOWING HOW THE FORMULARY INFORMATION IS ORGANIZED The following formulary reference guide is designed so that generic products are listed first in each drug category. The preferred brand name products are listed next, and non‐preferred brand products are listed last. -

Pre - PA Allowance Age 18 Years of Age Or Older Quantity 60 Grams Every 90 Days ______
DOXEPIN CREAM 5% (Prudoxin, Zonalon) Pre - PA Allowance Age 18 years of age or older Quantity 60 grams every 90 days _______________________________________________________________ Prior-Approval Requirements Age 18 years of age or older Diagnosis Patient must have the following: Moderate pruritus, due to atopic dermatitis (eczema) or lichen simplex chronicus AND the following: 1. Inadequate response, intolerance or contraindication to ONE medication in EACH of the following categories: a. Topical antihistamine (see Appendix I) b. High potency topical corticosteroid (see Appendix II) 2. Physician agrees to taper patient’s dose to the FDA recommended dose, and after tapered will only use for short-term pruritus relief (up to 8 days) a. Patients using over 60 grams of topical doxepin in 90 days be required to taper to 60 grams topical doxepin within 90 days Prior - Approval Limits Quantity 180 grams for 90 days Duration 3 months ___________________________________________________________________ Prior – Approval Renewal Requirements None (see appendix below) Doxepin 5% cream FEP Clinical Rationale DOXEPIN CREAM 5% (Prudoxin, Zonalon) APPENDIX I Drug Dosage Form Diphenhydramine Cream Phenyltoloxamine Lotion/ Cream Tripelennamine Cream Phendiamine Cream APPENDIX II Relative Potency of Selected Topical Corticosteroid Drug ProductsDosage Form Strength I. Very high potency Augmented betamethasone Ointment, Gel 0.05% dipropionate Clobetasol propionate Cream, Ointment 0.05% Diflorasone diacetate Ointment 0.05% Halobetasol propionate Cream, Ointment 0.05% II. High potency Amcinonide Cream, Lotion, 0.1% Augmented betamethasone Cream,Ointment Lotion 0.05% dipropionate Betamethasone Cream, Ointment 0.05% Betamethasonedipropionate valerate Ointment 0.1% Desoximetasone Cream, Ointment 0.25% Gel 0.05% Diflorasone diacetate Cream, Ointment 0.05% (emollient base) Fluocinonide Cream, Ointment, Gel 0.05% Halcinonide Cream, Ointment 0.1% Triamcinolone acetonide Cream, Ointment 0.5% III. -
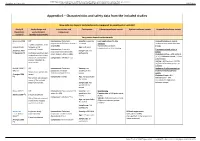
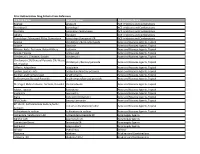
Appendix 6 – Characteristics and Safety Data from the Included Studies
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Open Appendix 6 – Characteristics and safety data from the included studies How safe are topical corticosteroids compared to emollient or vehicle? Study ID Study design and Intervention and Participants Cutaneous adverse events Systemic adverse events Unspecified adverse events (Systematic study duration comparator review*) (Quality assessment) Very potent topical corticosteroids Breneman 2003 RCT Intervention: Clobetasol Severity: moderate Local application site skin Unspecified adverse events (1) propionate 0.05% lotion (twice a to severe reactions Incidence comparable between 2 weeks treatment, then day) (n=96) No clinically significant groups. (unpublished) followed up for Age: ≥ 12 years telangiectasia or skin thinning additional 2 weeks Intervention: Clobetasol Treatment-related adverse (Feldman 2005 Sample size: 229 propionate 0.05% emollient events (2) Nankervis (3)) Cochrane risk of bias tool: participants cream (twice a day) (n=100) Clobetasol lotion = 4/96 patients randomisation described, (4.2%); Clobetasol cream = 1/100 allocation concealment Comparator: Vehicle (n=33) patients (1%) unclear, intention-to- Vehicle = 6/33 patients (18.2%) treat unclear. (Difference between groups: p= 0.0006a) Kimball 2008 (4) RCT Intervention: Clobetasol Severity: not Incidence of adverse events or (trial a) propionate emulsion specified in the treatment related adverse Duration not specified in formulation foam 0.05% review events (Frangos 2008 review Clobetasol foam = 8% (5)) Comparator: Vehicle Age: not specified in Risk of bias not assessed Vehicle foam = 10% the review in any of the included (no significant differences systematic reviews. -

(12) Patent Application Publication (10) Pub. No.: US 2008/0045488 A1 RODRGUEZ (43) Pub
US 20080045488A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2008/0045488 A1 RODRGUEZ (43) Pub. Date: Feb. 21, 2008 (54) PREVENTION OF OVARIAN CANCER BY Continuation-in-part of application No. 09/528,963, ADMINISTRATION OF PRODUCTS THAT filed on Mar. 21, 2000, now Pat. No. 6,765,002. INDUCE BIOLOGICAL EFFECTS IN THE Continuation-in-part of application No. 09/672,735, OVARIAN EPTHELIUM filed on Sep. 28, 2000, now Pat. No. 6.511,970. Continuation-in-part of application No. 09/532,340, (75) Inventor: Gustavo C. RODRIGUEZ, Durham, filed on Mar. 21, 2000, now abandoned. NC (US) Publication Classification Correspondence Address: JENNER & BLOCK, LLP (51) Int. Cl. ONE IBM PLAZA A6II 3/56 (2006.01) A 6LX 3/57 (2006.01) CHICAGO, IL 60611 (US) A6IP 35/00 (2006.01) (73) Assignee: New Life Pharmaceuticals Inc., Chi (52) U.S. Cl. ............................................ 514/171; 514/178 cago, IL (US) (57) ABSTRACT The present invention relates to compositions and methods (21) Appl. No.: 11/771,473 for preventing the development of epithelial ovarian cancer (22) Filed: Jun. 29, 2007 by administering compounds in an amount capable of regu lating TGF-B expression in the ovarian epithelium and/or Related U.S. Application Data capable of optimally altering expression of other Surrogate biomarkers identified by microarray technology. HRT and (63) Continuation of application No. 09/798,453, filed on OCP regimens comprising such compositions and methods Mar. 2, 2001. are disclosed. US 2008/0045488 A1 Feb. 21, 2008 PREVENTION OF OVARAN CANCER BY have been thought to increase ovarian cancer risk, whereas ADMINISTRATION OF PRODUCTS THAT INDUCE Some factors that Suppress ovulation have been thought to BIOLOGICAL EFFECTS IN THE OVARAN decrease risk. -

LGC Standards Pharmacopoeial Reference Standards 2014
LL CTS INKSP RODUTO A L P ITH W WEBSHO LGC Standards Pharmacopoeial reference standards 2014 FOR STANDARDS WITH CofA SEE OUR CATALOGUE: PHARMACEUTICAL IMPURITIES AND PRIMARY REFERENCE STANDARDS LGC Quality – ISO Guide 34 • GMP/GLP • ISO 9001 • ISO/IEC 17025 • ISO/IEC 17043 Pharmaceutical impurities Code Product CAS No. CS Price Unit Adiphenine Hydrochloride O LGC Standards N O MM1172.00 Adiphenine Hydrochloride 50-42-0 A 250mg HCl Pharmaceutical impurities and Adrenaline Tartrate OH H OH O OH primary reference standardsMM0614.00 2014 N OH Adrenaline Tartrate 51-42-3 A 500mg OH OH O OH OH H MM0614.02 L-Adrenaline 51-43-4 A 500mg OH N OH Imp. C (EP) as Hydrochloride: 1-(3,4-Di- O H OH MM0614.13 hydroxyphenyl)-2-(methylamino)ethanone 62-13-5 A 100mg N HCl Hydrochloride (Adrenalone Hydrochloride) OH (1R)-1-(3,4-Dihydroxyphenyl)-2- OH O S O MM0614.01 methylaminoethanesulphonic Acid H 78995-75-2 A 100mg OH N (Adrenaline -Sulphonate) OH Alanine NH2 MM0566.00 Alanine 56-41-7 A 500mg OH O Imp. A (Pharmeuropa): (2 S)-2-Aminobutanedioic Acid O NH 2 MM0567.00 OH (Aspartic Acid) 56-84-8 A 500mg OH O Albendazole O H MM0382.00 Albendazole N O 54965-21-8 A 500mg N H S N Imp. A (EP): 5-(Propylsulphanyl)-1H- H MM0382.01 N 80983-36-4 A 100mg NH2 benzimidazol-2-amine S N O H Imp. B (EP): Methyl [5-Propylsulphinyl)- N O MM0382.02 N 54029-12-8 A 100mg H 1H-benzimidazol-2-yl]carbamate S N O O H Imp. -
PA Drug Name Generic Name PA Summary Name Epaned Enalapril
Prior Authorization Drug Criteria Cross Reference PA Drug Name Generic Name PA Summary Name Epaned enalapril ACE Inhibitors and Combinations Perindopril perindopril ACE Inhibitors and Combinations Prestalia perindopril/amlodipine ACE Inhibitors and Combinations Qbrelis lisinopril ACE Inhibitors and Combinations Trandolapril/Verapamil ER by Greenstone trandolapril/verapamil ER ACE Inhibitors and Combinations Acanya clindamycin/benzoyl peroxide Acne and Rosacea Agents, Topical Aczone dapsone Acne and Rosacea Agents, Topical Altreno, Avita, Tretinoin, Retin-A Micro tretinoin Acne and Rosacea Agents, Topical Azelex, Finacea azelaic acid Acne and Rosacea Agents, Topical Clindamycin, Clindacin, Evoclin clindamycin Acne and Rosacea Agents, Topical Clindamycin 1%/Benzoyl Peroxide 5%, Neuac clindamycin/benzoyl peroxide Acne and Rosacea Agents, Topical Kit, Onexton Differin, Adapalene adapalene Acne and Rosacea Agents, Topical Epiduo, Epidue Forte adalpalene/benzoyl peroxide Acne and Rosacea Agents, Topical Ery Pad, erythromycin pad erythromycin Acne and Rosacea Agents, Topical Erythromycin/Benzoyl Peroxide erythromycin/benzoyl peroxide Acne and Rosacea Agents, Topical Metrogel, Metronidazole, Noritate, Rosadan metronidazole Acne and Rosacea Agents, Topical Fabior, Tazorac tazarotene Acne and Rosacea Agents, Topical Soolantra ivermectin Acne and Rosacea Agents, Topical Ziana tretinoin/clindamycin Acne and Rosacea Agents, Topical BPO Cloths benzoyl peroxide Acne and Rosacea Agents, Topical BP 10-1%, Sulfacetamide Sodium/Sulfur, sodium sulfacetamide/sulfur -

Pequot Health Care Steps Program* Updated Oct 2021 *Enrollment in Steps Program Varies on Health Plan Sponsor
Pequot Health Care - Pequot Pharmacuetical Network (PRxN) Pequot Health Care Steps Program* Updated Oct 2021 *Enrollment in Steps program varies on health plan sponsor. Member benefits and client contract will prevail. If you have que stions or need further assistance after consulting this table, call our Pharmacy Benefits number or the number on the back of your insurance card. Providers call 888-779-6638 for Authorization Form. Program effective 1-2014; Updated 9-2015, 10-2015, 1-2016, 3-2016, 10-2016, 01-2017, 04-2017, 7-2017, 02-2018, 04-2018, 05-2018, 08-2018, 11-2018, 4-2019, 6-2019, 9-2019, 12-2019, 4-2020, 6-2020, 10-2020, 1-2021, 7-2021, 10-2021 THERAPEUTIC DRUGS INCLUDED IN PROGRAM PREREQUISITE DRUGS CATEGORY (TARGET DRUGS) ALLERGY Previous use of one of the following generics either alone or as a Antihistamine Clarinex, Clarinex-D, Semprex, Xyzal component of a combination product: fexofenadine, levocetirizine, loratadine or cetirizine Acular and Acular LS (brand), Acuvail, Alocril, Alomide, Bepreve, Cromlon (brand), Elestat (brand), Emadine, Lastacraft, Optivar azelastine, cromolyn sodium, epinastine, ketotifen (rx-only), ketorolac Eye Drops (brand), Patanol (brand), Pazeo (brand and generic 0.7%), Pataday 0.4% and 0.5%, olopatadine 0.1% (brand and generic 0.2%), Zerviate (brand) Allergy Reaction AuviQ EpiPen Inhaled Nasal Beconase AQ, Dymista, Flunisolide, Nasonex, Omnaris, Qnasl, Previous use of the following generic: fluticasone nasal inhaler Steroids Rhinocort Aqua, Xhance, Zetonna ANTI-INFECTIVE Adoxa, Avidoxy, Doyxyxline