The Work Horse of Skull Base Surgery: Orbitozygomatic Approach
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Results Description of the SKULLS. the Overall Size of Both Skulls Was Considered to Be Within Normal Limits for Their Ethnic
Ossification Defects and Craniofacial Morphology In Incomplete Forms of Mandibulofacial Dysostosis A Description of Two Dry Skulls ERIK DAHL, D.D.S., DR. ODONT. ARNE BJORK, D.D.S., ODONT. DR. Copenhagen, Denmark The morphology of two East Indian dry skulls exhibiting anomalies which were suggested to represent incomplete forms of mandibulofacial dysostosis is described. Obvious although minor ossification anomalies were found localized to the temporal, sphenoid, the zygomatic, the maxillary and the mandibular bones. The observations substantiate the concept of the regional and bilateral nature of this malformation syndrome. Bilateral orbital deviations, hypoplasia of the malar bones, and incomplete zygomatic arches appear to be hard tissue aberrations which may be helpful in exami- nation for subclinical carrier status. Changes in mandibular morphology seem to be less distinguishing features in incomplete or abortive types of mandibulofacial dysostosis. KEY WORDS craniofacial problems, mandible, mandibulofacial dysostosis, maxilla, sphenoid bone, temporal bone, zygomatic bone Mandibulofacial dysostosis (MFD) often roentgencephalometric examinations were results in the development of a characteristic made of the skulls, and tomograms were ob- facial disfigurement with considerable simi- tained of the internal and middle ear. Com- larity between affected individuals. However, parisons were made with normal adult skulls the symptoms may vary highly in respect to and with an adult skull exhibiting the char- type and degree, and both incomplete and acteristics of MFD. All of the skulls were from abortive forms of the syndrome have been the same ethnic group. ' reported in the literature (Franceschetti and Klein, 1949; Moss et al., 1964; Rogers, 1964). Results In previous papers, we have shown the DEsCRIPTION OF THE SKULLS. -

A Description of the Geological Context, Discrete Traits, and Linear Morphometrics of the Middle Pleistocene Hominin from Dali, Shaanxi Province, China
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 150:141–157 (2013) A Description of the Geological Context, Discrete Traits, and Linear Morphometrics of the Middle Pleistocene Hominin from Dali, Shaanxi Province, China Xinzhi Wu1 and Sheela Athreya2* 1Laboratory for Human Evolution, Institute of Vertebrate Paleontology and Paleoanthropology, Chinese Academy of Sciences, Beijing 100044, China 2Department of Anthropology, Texas A&M University, College Station, TX 77843 KEY WORDS Homo heidelbergensis; Homo erectus; Asia ABSTRACT In 1978, a nearly complete hominin Afro/European Middle Pleistocene Homo and align it fossil cranium was recovered from loess deposits at the with Asian H. erectus.Atthesametime,itdisplaysa site of Dali in Shaanxi Province, northwestern China. more derived morphology of the supraorbital torus and It was subsequently briefly described in both English supratoral sulcus and a thinner tympanic plate than and Chinese publications. Here we present a compre- H. erectus, a relatively long upper (lambda-inion) occi- hensive univariate and nonmetric description of the pital plane with a clear separation of inion and opis- specimen and provide comparisons with key Middle thocranion, and an absolute and relative increase in Pleistocene Homo erectus and non-erectus hominins brain size, all of which align it with African and Euro- from Eurasia and Africa. In both respects we find pean Middle Pleistocene Homo. Finally, traits such as affinities with Chinese H. erectus as well as African the form of the frontal keel and the relatively short, and European Middle Pleistocene hominins typically broad midface align Dali specifically with other referred to as Homo heidelbergensis.Specifically,the Chinese specimens from the Middle Pleistocene Dali specimen possesses a low cranial height, relatively and Late Pleistocene, including H. -

Introduction to the Skeletal System and the Axial Skeleton 155
chapter Introduction to the 7 Skeletal System and the Axial Skeleton CHAPTER OVERVIEW OBJECTIVES 7.1 Introduction to the Skeletal System ……………… 153 1. Describe the gross anatomy and structure of a long 7.2 Bone Structure ………………………………………… 154 bone 7.3 Bone Histology ………………………………………… 155 2. Describe and compare the underlying histology of spongy and compact bone. 7.4 The Human Skeleton: Axial and Appendicular Divisions …………………………………………………… 156 3. List the five general shapes of bones. 7.5 Bone Classification and Markings ………………… 157 4. Describe and compare the different kinds of bone markings visible on the skeleton. 7.6 Axial Skeleton …………………………………………… 159 7.6a Cranium 5. Identify the components of the axial skeleton: cranial, 7.6b Facial facial, hyoid, vertebra, ribs and sternum. 7.6c Hyoid Bone 7.6d Vertebral Column 7.6e Thoracic Cage 7.1 Introduction to the Skeletal System The skeletal system serves to support the body’s soft tissues and to protect the body’s soft internal organs. Another important function that the bones have is to store materials such as calcium, phosphorus and lipids. Additionally, blood cells are synthesized in the red bone marrow to be released into the bloodstream. Bones serve as levers for the muscular system, working with them to produce movement and maintain posture. The human body contains 2 major kinds of bone tissue: compact and spongy. Compact bone (dense bone) is found on the outer surface of bones and serves as a place to absorb most of the stress on the bones. Spongy bone (cancellous tissue) is found on the inside of the compact bone layer. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

Topographical Anatomy and Morphometry of the Temporal Bone of the Macaque
Folia Morphol. Vol. 68, No. 1, pp. 13–22 Copyright © 2009 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and morphometry of the temporal bone of the macaque J. Wysocki 1Clinic of Otolaryngology and Rehabilitation, II Medical Faculty, Warsaw Medical University, Poland, Kajetany, Nadarzyn, Poland 2Laboratory of Clinical Anatomy of the Head and Neck, Institute of Physiology and Pathology of Hearing, Poland, Kajetany, Nadarzyn, Poland [Received 7 July 2008; Accepted 10 October 2008] Based on the dissections of 24 bones of 12 macaques (Macaca mulatta), a systematic anatomical description was made and measurements of the cho- sen size parameters of the temporal bone as well as the skull were taken. Although there is a small mastoid process, the general arrangement of the macaque’s temporal bone structures is very close to that which is observed in humans. The main differences are a different model of pneumatisation and the presence of subarcuate fossa, which possesses considerable dimensions. The main air space in the middle ear is the mesotympanum, but there are also additional air cells: the epitympanic recess containing the head of malleus and body of incus, the mastoid cavity, and several air spaces on the floor of the tympanic cavity. The vicinity of the carotid canal is also very well pneuma- tised and the walls of the canal are very thin. The semicircular canals are relatively small, very regular in shape, and characterized by almost the same dimensions. The bony walls of the labyrinth are relatively thin. -

Factors Influencing the Articular Eminence of the Temporomandibular Joint (Review)
EXPERIMENTAL AND THERAPEUTIC MEDICINE 22: 1084, 2021 Factors influencing the articular eminence of the temporomandibular joint (Review) MARIA JUSTINA ROXANA VÎRLAN1, DIANA LORETA PĂUN2, ELENA NICOLETA BORDEA3, ANGELO PELLEGRINI3, ARSENIE DAN SPÎNU4, ROXANA VICTORIA IVAȘCU5, VICTOR NIMIGEAN5 and VANDA ROXANA NIMIGEAN1 1Discipline of Oral Rehabilitation, Faculty of Dental Medicine; 2Discipline of Endocrinology, Faculty of Medicine; 3Department of Specific Disciplines, Faculty of Midwifery and Nursing;4 Discipline of Urology, ‘Dr Carol Davila’ Central Military Emergency University Hospital, Faculty of Medicine; 5Discipline of Anatomy, Faculty of Dental Medicine, ‘Carol Davila’ University of Medicine and Pharmacy, 020021 Bucharest, Romania Received April 28, 2021; Accepted May 28, 2021 DOI: 10.3892/etm.2021.10518 Abstract. The temporomandibular joint (TMJ), the most 4. Factors influencing the inclination of the articular eminence complex and evolved joint in humans, presents two articular 5. Biological sex surfaces: the condyle of the mandible and the articular eminence 6. Age (AE) of the temporal bone. AE is the anterior root of the zygo‑ 7. Edentulism matic process of the temporal bone and has an anterior and 8. Conclusions a posterior slope, the latter being also known as the articular surface. AE is utterly important in the biomechanics of the TMJ, as the mandibular condyle slides along the posterior slope 1. Introduction of the AE while the mandible moves. The aim of this review was to assess significant factors influencing the inclination of The temporomandibular joint (TMJ), the most complex and the AE, especially modifications caused by aging, biological evolved joint in humans, is defined by the paired joints that sex or edentulism. -
The Axial Skeleton Visual Worksheet
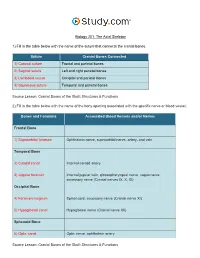
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

The Temporomandibular Joint: Pneumatic Temporal Cells Open Into the Articular and Extradural Spaces C
CORE Metadata, citation and similar papers at core.ac.uk Provided by Via Medica Journals Folia Morphol. Vol. 78, No. 3, pp. 630–636 DOI: 10.5603/FM.a2018.0111 O R I G I N A L A R T I C L E Copyright © 2019 Via Medica ISSN 0015–5659 journals.viamedica.pl The temporomandibular joint: pneumatic temporal cells open into the articular and extradural spaces C. Bichir, M.C. Rusu, A.D. Vrapciu, N. Măru “Carol Davila” University of Medicine and Pharmacy of Bucharest, Romania [Received: 1 October 2018; Accepted: 22 November 2018] The pneumatisation of the articular tubercle (PAT) of the temporal squama is a rare condition that modifies the barrier between the temporomandibular joint (TMJ) space and the middle cranial fossa. During a routine examination of the cone-beam computed tomography (CBCT) files of patients who were scanned for dental medical purposes, we identified a case with multiple rare anatomic variations. First, the petrous apex was bilaterally pneumatised. Moreover, bilateral and multilocular PAT were observed, while on one side it was further found that the pneumatic cells were equally dehiscent towards the extradural space and the superior joint space. To the best of our knowledge, such dehiscence has not pre- viously been reported. The two temporomastoid pneumatisations were extended with occipital pneumatisations of the lateral masses and occipital condyles, the latter being an extremely rare evidence. The internal dehiscence of the mandibular canal in the right ramus of the mandible was also noted. Additionally, double mental foramen and impacted third molars were found on the left side. -

Orbital Meningiomas Meningiomas Orbitários Carlos Eduardo Da Silva, M.D
31 Revisão Orbital Meningiomas Meningiomas Orbitários Carlos Eduardo da Silva, M.D. 1 Paulo Eduardo Freitas, M.D. Ph.D.2 Alicia Del Carmem Becerra Romero, M.D.3 Tâmen Moyses Pereyra4 Vicente Faraon Fonseca4 Willian Alves Martins4 Márcio Aloisio Bezerra Cavalcanti Rockenbach4 Fáberson João Mocelin Oliveira4 ABSTRACT RESUMO Orbital meningiomas usually invade the orbit as an extension Meningeomas orbitários invadem a órbita, na maioria dos ca- of the sphenoid wing meningiomas, clinoidal meningiomas, sos, como uma extensão de meningeomas da asa do esfenóide, cavernous sinus meningiomas and tuberculum sella tumors. meningeomas do seio cavernoso, meningeomas da clinóide e They also arise into the orbit originating from the optic sheath do tubérculo da sela. Eles também podem ser originados do or as ectopical lesions. The authors present a review of clini- revestimento dural do nervo óptico ou como lesões ectópicas cal aspects and surgical treatment of the orbital meningio- intraorbitais. Os autores apresentam uma revisão dos aspectos mas. Material and methods: The authors present a literature clínicos e cirúrgicos dos meningeomas orbitários. Material e review of the anatomical, clinical, and surgical aspects of métodos: Os autores apresentam uma revisão da literatura dos the orbital meningiomas, add illustrative cases, pointing aspectos anatômicos, clínicos e cirúrgicos dos meningeomas their principal concerns about the treatment of such tumors. orbitários, com casos ilustrativos, apresentando suas principais Results: Exophthalmos and unilateral visual loss are the most preocupações no manejo destes tumores. Resultados: Exoftal- common features of the orbital meningiomas. There are two mia e perda visual unilateral são os achados mais frequentes important surgical routes to approach such tumors, which are nos meningeomas orbitários. -
Axial Skeleton 214 7.7 Development of the Axial Skeleton 214
SKELETAL SYSTEM OUTLINE 7.1 Skull 175 7.1a Views of the Skull and Landmark Features 176 7.1b Sutures 183 7.1c Bones of the Cranium 185 7 7.1d Bones of the Face 194 7.1e Nasal Complex 198 7.1f Paranasal Sinuses 199 7.1g Orbital Complex 200 Axial 7.1h Bones Associated with the Skull 201 7.2 Sex Differences in the Skull 201 7.3 Aging of the Skull 201 Skeleton 7.4 Vertebral Column 204 7.4a Divisions of the Vertebral Column 204 7.4b Spinal Curvatures 205 7.4c Vertebral Anatomy 206 7.5 Thoracic Cage 212 7.5a Sternum 213 7.5b Ribs 213 7.6 Aging of the Axial Skeleton 214 7.7 Development of the Axial Skeleton 214 MODULE 5: SKELETAL SYSTEM mck78097_ch07_173-219.indd 173 2/14/11 4:58 PM 174 Chapter Seven Axial Skeleton he bones of the skeleton form an internal framework to support The skeletal system is divided into two parts: the axial skele- T soft tissues, protect vital organs, bear the body’s weight, and ton and the appendicular skeleton. The axial skeleton is composed help us move. Without a bony skeleton, we would collapse into a of the bones along the central axis of the body, which we com- formless mass. Typically, there are 206 bones in an adult skeleton, monly divide into three regions—the skull, the vertebral column, although this number varies in some individuals. A larger number of and the thoracic cage (figure 7.1). The appendicular skeleton bones appear to be present at birth, but the total number decreases consists of the bones of the appendages (upper and lower limbs), with growth and maturity as some separate bones fuse. -

Topographical Anatomy and Measurements of Selected Parameters of the Rat Temporal Bone
Folia Morphol. Vol. 67, No. 2, pp. 111–119 Copyright © 2008 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and measurements of selected parameters of the rat temporal bone J. Wysocki Clinic of Otolaryngology, Medical Faculty No. 2, Medical University of Warsaw, Kajetany, Poland Institute of Physiology and Pathology of Hearing, Warsaw, Poland [Received 22 October 2008; Accepted 22 November 2008] On the basis of dissection of 24 bones of 12 black rats a systematic anatomical description was made and measurements of selected size parameters of the tem- poral bone were taken. Besides the main air space in the middle ear, the tym- panic bulla, there are also additional air cells, namely the anterior and posterior epitympanic recesses, containing the head of the malleus and the body of the incus. On the side of the epitympanic recesses the following are easily accessi- ble: the malleus head and the core of the incus, the superior and lateral semicir- cular canals and the facial nerve. On the side of the ventral tympanic bulla it is easy access to both windows and the cochlea. The semicircular canals are rela- tively large, the lateral canal being the largest and the posterior the smallest. The length of the spiral canal of the cochlea does not exceed 11 mm. It is worth mentioning that both the vertical and horizontal dimensions of the scala vestibuli and scala tympani do not even exceed 0.7 mm in the basal turn, and are signif- icantly decreased to tenths of a millimetre in further turns.