Hyperpigmentation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Melanocytes and Their Diseases
Downloaded from http://perspectivesinmedicine.cshlp.org/ on October 2, 2021 - Published by Cold Spring Harbor Laboratory Press Melanocytes and Their Diseases Yuji Yamaguchi1 and Vincent J. Hearing2 1Medical, AbbVie GK, Mita, Tokyo 108-6302, Japan 2Laboratory of Cell Biology, National Cancer Institute, National Institutes of Health, Bethesda, Maryland 20892 Correspondence: [email protected] Human melanocytes are distributed not only in the epidermis and in hair follicles but also in mucosa, cochlea (ear), iris (eye), and mesencephalon (brain) among other tissues. Melano- cytes, which are derived from the neural crest, are unique in that they produce eu-/pheo- melanin pigments in unique membrane-bound organelles termed melanosomes, which can be divided into four stages depending on their degree of maturation. Pigmentation production is determined by three distinct elements: enzymes involved in melanin synthesis, proteins required for melanosome structure, and proteins required for their trafficking and distribution. Many genes are involved in regulating pigmentation at various levels, and mutations in many of them cause pigmentary disorders, which can be classified into three types: hyperpigmen- tation (including melasma), hypopigmentation (including oculocutaneous albinism [OCA]), and mixed hyper-/hypopigmentation (including dyschromatosis symmetrica hereditaria). We briefly review vitiligo as a representative of an acquired hypopigmentation disorder. igments that determine human skin colors somes can be divided into four stages depend- Pinclude melanin, hemoglobin (red), hemo- ing on their degree of maturation. Early mela- siderin (brown), carotene (yellow), and bilin nosomes, especially stage I melanosomes, are (yellow). Among those, melanins play key roles similar to lysosomes whereas late melanosomes in determining human skin (and hair) pigmen- contain a structured matrix and highly dense tation. -

Frequency of Different Types of Facial Melanoses Referring to the Department of Dermatology and Venereology, Nepal Medical Colle
Amatya et al. BMC Dermatology (2020) 20:4 https://doi.org/10.1186/s12895-020-00100-3 RESEARCH ARTICLE Open Access Frequency of different types of facial melanoses referring to the Department of Dermatology and Venereology, Nepal Medical College and Teaching Hospital in 2019, and assessment of their effect on health-related quality of life Bibush Amatya* , Anil Kumar Jha and Shristi Shrestha Abstract Background: Abnormalities of facial pigmentation, or facial melanoses, are a common presenting complaint in Nepal and are the result of a diverse range of conditions. Objectives: The objective of this study was to determine the frequency, underlying cause and impact on quality of life of facial pigmentary disorders among patients visiting the Department of Dermatology and Venereology, Nepal Medical College and Teaching Hospital (NMCTH) over the course of one year. Methods: This was a cross-sectional study conducted at the Department of Dermatology and Venereology, NMCT H. We recruited patients with facial melanoses above 16 years of age who presented to the outpatient department. Clinical and demographic data were collected and all the enrolled participants completed the validated Nepali version of the Dermatology Life Quality Index (DLQI). Results: Between January 5, 2019 to January 4, 2020, a total of 485 patients were recruited in the study. The most common diagnoses were melasma (166 patients) and post acne hyperpigmentation (71 patients). Quality of life impairment was highest in patients having melasma with steroid induced rosacea-like dermatitis (DLQI = 13.54 ± 1.30), while it was lowest in participants with ephelides (2.45 ± 1.23). Conclusion: Facial melanoses are a common presenting complaint and lead to substantial impacts on quality of life. -

Melasma on the Nape of the Neck in a Man
Letters to the Editor 181 Melasma on the Nape of the Neck in a Man Ann A. Lonsdale-Eccles and J. A. A. Langtry Sunderland Royal Hospital, Kayll Road, Sunderland SR4 7TP, UK. E-mail: [email protected] Accepted July 19, 2004. Sir, sunlight and photosensitizing agents may be more We report a 47-year-old man with light brown macular relevant. pigmentation on the nape of his neck (Fig. 1). It was The differential diagnosis for pigmentation at this site asymptomatic and had developed gradually over 2 years. includes Riehl’s melanosis, Berloque dermatitis and He worked outdoors as a pipe fitter on an oilrig module; poikiloderma of Civatte. Riehl’s melanosis typically however, he denied exposure at this site because he involves the face with a brownish-grey pigmentation; always wore a shirt with a collar that covered the biopsy might be expected to show interface change and affected area. However, on further questioning it liquefaction basal cell degeneration with a moderate transpired that he spent most of the day with his head lymphohistiocytic infiltrate, melanophages and pigmen- bent forward. This reproducibly exposed the area of tary incontinence in the upper dermis. It is usually pigmentation with a sharp cut off inferiorly at the level associated with cosmetic use and may be considered of his collar. He used various shampoos, aftershaves and synonymous with pigmented allergic contact dermatitis shower gels, but none was applied directly to that area. of the face (6, 7). Berloque dermatitis is considered to be His skin was otherwise normal and there was no family caused by a photoirritant reaction to bergapentin; it history of abnormal pigmentation. -

An Unusual Presentation of a Unilateral Asymptomatic Riehl's
ts & C por a e se R S l Michael, Med Rep Case Stud 2018, 3:1 t a u c d i i DOI: 10.4172/2572-5130.1000152 d e s e M + Medical Reports and Case Studies ISSN: 2572-5130 Case Report Open Access An Unusual Presentation of a Unilateral Asymptomatic Riehl’s Melanosis in a 45 Year Old Male Chan Kam Tim Michael* Department of Dermatology, Hong Kong Academy of Medicine, Hong Kong *Corresponding author: Chan Kam Tim Michael, Department of Dermatology, Hong Kong Academy of Medicine, Hong Kong, Tel: +85221282129; E-mail: [email protected] Received Date: Feb 12, 2018; Accepted Date: Mar 12, 2018; Published Date: Mar 21, 2018 Copyright: © 2018 Michael CKT. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Introduction but of post-inflammatory hyperpigmentation, Acquired unilateral Nevus (Hori’s Nevus), Riehl’s melanosis, Drug-induced Pigmented contact dermatitis (PCD), also known as Riehl’s hyperpigmentation, Lichenoid dermatitis; as well as Melasma and melanosis, is a rare facial hyperpigmentation usually secondary to Ochronosis. cosmetics. There are few documented reports in the literature, and many cases without proven diagnosis may have been treated with pigment lasers, especially in beauty parlour settings. We report a case referred from a private practitioner who has a special interest in dermatology. The patient was diagnosed subsequently as having Riehl’s melanosis and treated with non-tyrosinase inhibitor bleaching agents, sun avoidance and mandatory abstinence from over-the-counter cosmetic products. -
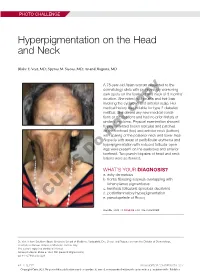
Hyperpigmentation on the Head and Neck
PHOTO CHALLENGE Hyperpigmentation on the Head and Neck Blake E. Vest, MD; Spyros M. Siscos, MD; Anand Rajpara, MD A 78-year-old Asian woman presented to the dermatology clinic with progressively worsening dark spots on the forehead and neck of 3 months’ duration. She noted mild pruritis and hair loss involving the eyebrows and anterior scalp. Her medical history was notable for type 2 diabetes mellitus. She deniedcopy any new medical condi- tions or medications and had no prior history of similar symptoms. Physical examination showed hyperpigmented brown macules and patches on the forehead (top) and anterior neck (bottom) withnot sparing of the posterior neck and lower face. Alopecia with areas of perifollicular erythema and hyperpigmentation with reduced follicular open- ings were present on the eyebrows and anterior Doforehead. Two punch biopsies of head and neck lesions were performed. WHAT’S YOUR DIAGNOSIS? a. ashy dermatosis b. frontal fibrosing alopecia overlapping with lichen planus pigmentosus c. keratosis follicularis spinulosa decalvans d. postinflammatory hyperpigmentation CUTIS e. pseudopelade of Brocq PLEASE TURN TO PAGE E3 FOR THE DIAGNOSIS Dr. Vest is from Southern Illinois University School of Medicine, Springfield. Drs. Siscos and Rajpara are from the Division of Dermatology, University of Kansas School of Medicine, Kansas City. The authors report no conflict of interest. Correspondence: Blake E. Vest, MD ([email protected]). doi:10.12788/cutis.0226 E2 I CUTIS® WWW.MDEDGE.COM/DERMATOLOGY Copyright Cutis 2021. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. PHOTO CHALLENGE DISCUSSION THE DIAGNOSIS: Frontal Fibrosing Alopecia Overlapping With Lichen Planus Pigmentosus icroscopic examination revealed focal dermal of the skin have been reported, including the entire pigmentation, papillary fibrosis, and epidermal scalp, eyebrows, and eyelashes. -

Pigmented Contact Dermatitis and Chemical Depigmentation
18_319_334* 05.11.2005 10:30 Uhr Seite 319 Chapter 18 Pigmented Contact Dermatitis 18 and Chemical Depigmentation Hideo Nakayama Contents ca, often occurs without showing any positive mani- 18.1 Hyperpigmentation Associated festations of dermatitis such as marked erythema, with Contact Dermatitis . 319 vesiculation, swelling, papules, rough skin or scaling. 18.1.1 Classification . 319 Therefore, patients may complain only of a pigmen- 18.1.2 Pigmented Contact Dermatitis . 320 tary disorder, even though the disease is entirely the 18.1.2.1 History and Causative Agents . 320 result of allergic contact dermatitis. Hyperpigmenta- 18.1.2.2 Differential Diagnosis . 323 tion caused by incontinentia pigmenti histologica 18.1.2.3 Prevention and Treatment . 323 has often been called a lichenoid reaction, since the 18.1.3 Pigmented Cosmetic Dermatitis . 324 presence of basal liquefaction degeneration, the ac- 18.1.3.1 Signs . 324 cumulation of melanin pigment, and the mononucle- 18.1.3.2 Causative Allergens . 325 ar cell infiltrate in the upper dermis are very similar 18.1.3.3 Treatment . 326 to the histopathological manifestations of lichen pla- 18.1.4 Purpuric Dermatitis . 328 nus. However, compared with typical lichen planus, 18.1.5 “Dirty Neck” of Atopic Eczema . 329 hyperkeratosis is usually milder, hypergranulosis 18.2 Depigmentation from Contact and saw-tooth-shape acanthosis are lacking, hyaline with Chemicals . 330 bodies are hardly seen, and the band-like massive in- 18.2.1 Mechanism of Leukoderma filtration with lymphocytes and histiocytes is lack- due to Chemicals . 330 ing. 18.2.2 Contact Leukoderma Caused Mainly by Contact Sensitization . -

Table I. Genodermatoses with Known Gene Defects 92 Pulkkinen
92 Pulkkinen, Ringpfeil, and Uitto JAM ACAD DERMATOL JULY 2002 Table I. Genodermatoses with known gene defects Reference Disease Mutated gene* Affected protein/function No.† Epidermal fragility disorders DEB COL7A1 Type VII collagen 6 Junctional EB LAMA3, LAMB3, ␣3, 3, and ␥2 chains of laminin 5, 6 LAMC2, COL17A1 type XVII collagen EB with pyloric atresia ITGA6, ITGB4 ␣64 Integrin 6 EB with muscular dystrophy PLEC1 Plectin 6 EB simplex KRT5, KRT14 Keratins 5 and 14 46 Ectodermal dysplasia with skin fragility PKP1 Plakophilin 1 47 Hailey-Hailey disease ATP2C1 ATP-dependent calcium transporter 13 Keratinization disorders Epidermolytic hyperkeratosis KRT1, KRT10 Keratins 1 and 10 46 Ichthyosis hystrix KRT1 Keratin 1 48 Epidermolytic PPK KRT9 Keratin 9 46 Nonepidermolytic PPK KRT1, KRT16 Keratins 1 and 16 46 Ichthyosis bullosa of Siemens KRT2e Keratin 2e 46 Pachyonychia congenita, types 1 and 2 KRT6a, KRT6b, KRT16, Keratins 6a, 6b, 16, and 17 46 KRT17 White sponge naevus KRT4, KRT13 Keratins 4 and 13 46 X-linked recessive ichthyosis STS Steroid sulfatase 49 Lamellar ichthyosis TGM1 Transglutaminase 1 50 Mutilating keratoderma with ichthyosis LOR Loricrin 10 Vohwinkel’s syndrome GJB2 Connexin 26 12 PPK with deafness GJB2 Connexin 26 12 Erythrokeratodermia variabilis GJB3, GJB4 Connexins 31 and 30.3 12 Darier disease ATP2A2 ATP-dependent calcium 14 transporter Striate PPK DSP, DSG1 Desmoplakin, desmoglein 1 51, 52 Conradi-Hu¨nermann-Happle syndrome EBP Delta 8-delta 7 sterol isomerase 53 (emopamil binding protein) Mal de Meleda ARS SLURP-1 -

A Clinicoepidemiological Study of Facial Hypermelanosis Among Females of Reproductive Age Group
Our Dermatology Online Original Article A cclinicoepidemiologicallinicoepidemiological sstudytudy ooff ffacialacial hhypermelanosisypermelanosis aamongmong ffemalesemales ooff rreproductiveeproductive aagege ggrouproup Sameer Abrol1, Rohini Sharma2 1M.D. Medicine. GMC Jammu, Jammu and Kashmir, India, 2Assistant professor, Department of Dermatology, GMC Rajouri, Jammu and Kashmir, India Corresponding author: Dr. Rohini Sharma, E-mail: [email protected] ABSTRACT Background: Facial hypermelanosis has great psychological and aesthetic complications attached to it specially in females. A number of factors like genetic, environmental, systemic, work in consortium to give rise to various types of hypermelanosis. Women in the 15-49 years age group, which is the reproductive age group are influenced by various hormonal alterations along with external and systemic agents thus manifesting as various types of hypermelanosis. Aims and objectives: This study was undertaken to assess the clinical and epidemiological aspects of various types of facial hypermelanosis and various factors implicated. Material and methods: A total of 350 women in the age group of 15- 49 years were taken up for the study. A detailed clinical history, thorough examination was done in all patients. Relevant investigations were carried out. All the results were statistically analyzed and inferences were drawn. Results: A total of 350 women were taken up for study. Maximum patients (133,38%) were in the age group of 26 -35 years. Among various hypermelanosis, maximum women(128,36.5%) came with the complaint of melasma, 90(25.7%) women with post inflammatory hypermelanosis, 50(14.3%)females with periorbital hypermelanosis. In our study, melasma, post inflammatory hyperpigmentation due to acne, acanthosis nigricans formed a major share in the 15-49 years age group thus suggesting the role of hormonal alterations and rising PCOS. -

A Clinico-Epidemiological Study of Facial Dermatoses in Women
International Journal of Health and Clinical Research, 2021;4(11):198-206 e-ISSN: 2590-3241, p-ISSN: 2590-325X ____________________________________________________________________________________________________________________________________________ Original Research Article A clinico-epidemiological study of facial dermatoses in women Dilip Chandra Chintada1, Kiran KanthVudayana1, Anand Kumar Vaggu2*, Jami Vijaya Sree3 1Assistant Professor, Department of Dermatology, Venereology and Leprosy, Great Eastern Medical School and Hospital, Ragolu, Srikakulam, Andhra Pradesh, India 2Associate Professor, Department of Dermatology, Venereology and Leprosy, Great Eastern Medical School and Hospital Ragolu, Srikakulam, Andhra Pradesh, India 3Professor and HOD,Department of Dermatology, Venereology and Leprosy, Great Eastern Medical School and Hospital Ragolu, Srikakulam, Andhra Pradesh, India Received: 19-03-2021 / Revised: 10-05-2021 / Accepted: 04-06-2021 Abstract Background: The face is the most prominent part of the body. Facial blemishes and disorders directly reflect on patients' physical appearance, cosmesis, and self-image. They may contribute to dysmorphism and even lead to depressive illness in susceptible individuals, especially women. Therefore, it is essential for the early identification and management of facial skin disorders. Aims: To study the clinical pattern and epidemiological determinants of facial dermatoses among females above ten years. Materials and Methods:This cross-sectional study was conducted in a rural tertiary hospital from January 2019 to December 2019 among 500 female patients with Facial Dermatoses with their consent. Investigations, including the skin scrapings for potassium hydroxide mount, woods lamp examination, skin biopsy, and relevant investigations, wherever required, were done. Females above the age of 10 years with facial dermatoses were included with due consent/ assent. Patients with drug reactions and sexually transmitted infections (STIs) were excluded. -

General Dermatology): Validation for Skin of Color Through a Delphi Expert Consensus
Report International Dermoscopy Society criteria for non-neoplastic dermatoses (general dermatology): validation for skin of color through a Delphi expert consensus Enzo Errichetti1, MD, Balachandra S. Ankad2, MD, Abhijeet K. Jha3, MD, Sidharth Sonthalia4, MD, Bengu N. Akay5, MD, Roberto Bakos6, MD, Yasmeen J. Bhat7, MD, Manal Bosseila8, MD, Ralph Braun9, MD, Horacio Cabo10, MD, Emilia N. Cohen Sabban10, MD, Manas Chatterjee11, MD, Maryam Daneshpazhooh12, MD, Deepak Jakhar13, MD, Feroze Kaliyadan14, MD, Awatef Kelati15, MD, Vinay Keshavamurthy16, MD, Shekhar Neema17, MD, Ahmed Sadek18, MD, Gabriel Salerni19, MD, David L. Swanson20, MD, Trilokraj Tejasvi21, MD, Richard Usatine22, MD and Aimilios Lallas23, MD 1Institute of Dermatology, “Santa Maria Abstract della Misericordia” University Hospital, Background The International Dermoscopy Society (IDS) recently released a set of five 2 Udine, Italy, Department of Dermatology, basic dermoscopic parameters (vessels, scales, follicular findings, “other structures,” and Venereology and Leprosy, SN Medical specific clues) encompassing a total of 31 subitems to standardize the use of dermoscopy College, Bagalkot, Karnataka, India, 3Department of Dermatology & STD, Patna in non-neoplastic dermatoses, yet they have been developed taking into account Medical College & Hospital, Patna, India, Caucasian/Asian skin, with consequent possible limitations if used in dark skin. 4 Skinnocence, Skin Clinic & Research Objectives To validate the abovementioned criteria for the use in dark-skinned patients 5 Center, Gurugram, India, Department of (phototypes IV–VI) through an expert consensus. Dermatology, School of Medicine, Ankara Methods The two-round Delphi method was adopted, with an iterative process consisting University, Ankara, Turkey, 6Department of Dermatology, Hospital de Clınicas de Porto of two rounds of email questionnaires. -

Contact Dermatitis: a Great Imitator
CID-07389; No of Pages 17 Clinics in Dermatology (xxxx) xx,xxx Contact dermatitis: a great imitator Ömer Faruk Elmas,MDa,⁎, Necmettin Akdeniz,MDb, Mustafa Atasoy,MDc, Ayse Serap Karadag,MDb aDepartment of Dermatology, Faculty of Medicine, Ahi Evran University, Kırşehir, Turkey bDepartment of Dermatology, Faculty of Medicine, Istanbul Medeniyet University, Istanbul, Turkey cDepartment of Dermatology, Kayseri City Hospital, Health Science University, Kayseri, Turkey Abstract Contact dermatitis (CD) refers to a group of cutaneous diseases caused by contact with allergens or irritants. It is characterized by different stages of an eczematous eruption and has the ability to mimic a wide variety of dermatologic conditions, including inflammatory dermatitis, infectious conditions, cutaneous lymphoma, drug eruptions, and nutritional deficiencies. Irritant CD and allergic CD are the two main presen- tations of the disease. The diagnosis is based on a detailed history, physical examination, and patch testing, if necessary. Knowing the conditions mimicked by CD should improve the accuracy of the diagnosis. Avoid- ing the causative substances and taking preventive measures are necessary for the treatment. © 2019 Elsevier Inc. All rights reserved. Introduction Epidemiology Contact dermatitis (CD) describes a group of skin diseases CD can be seen at any age, and its estimated prevalence caused by contact allergens or irritant substances. CD is ranges from 1.7% to 6.3% in various published studies.3 It is characterized by an eczematous eruption and can imitate many more common in urban areas, with the incidence being higher dermatologic conditions.1,2 Irritant contact dermatitis (ICD) in women and the elderly.3 Many studies, however, suggest and allergic contact dermatitis (ACD) are considered as the that sex and age cannot be considered as independent risk two subgroups of the entity. -
Dermoscopy in General Dermatology (Non-Neoplastic Dermatoses) of Skin
Clinical report Eur J Dermatol 2020; 30(6): 688-98 Enzo ERRICHETTI1 Dermoscopy in general dermatology Balachandra Suryakant ANKAD2 Sidharth SONTHALIA3 (non-neoplastic dermatoses) of skin of colour: Abhijeet Kumar JHA4 a comparative retrospective study by the Vinay KESHAVAMURTHY5 Athanassios KYRGIDIS6 International Dermoscopy Society Shekhar NEEMA7 Manas CHATTERJEE8 Feroze KALIYADAN9 Background: Dermoscopy has been shown to be a useful supportive Sunil DOGRA5 Soumil KHARE10 tool to assist the diagnosis of several non-neoplastic dermatoses (i.e. Awatef KELATI11 inflammatory, infiltrative and infectious skin diseases), yet data on skin Bengu Nisa AKAY12 of colour is still limited. Objectives: To characterize dermoscopic fea- Horacio CABO13 tures of non-neoplastic dermatoses in dark-skinned patients in order Yasmeen Jabeen BHAT14 to identify possible clues that may facilitate the differential diagno- Manal BOSSEILA15 Atula GUPTA16 sis of clinically similar conditions. Materials & Methods: Members of Pragya NAIR17 the International Dermoscopy Society were invited to submit cases of Sakshi GAIKWAD2 any non-neoplastic dermatosis developing in patients with Fitzpatrick Puravoor JAYASREE18 Phototypes V-VI whose diagnosis had been confirmed by the corre- 13 Emilia Noemi Cohen SABBAN sponding gold standard diagnostic test. A standardized assessment of Giuseppe STINCO1 Zoe APALLA19 the dermoscopic images and a comparative analysis according to clinical Iris ZALAUDEK20 presentation were performed. Seven clinical categories were identified: Aimilios LALLAS21 (I) papulosquamous dermatoses; (II) facial hyperpigmented dermatoses; (III) extra-facial hyperpigmented dermatoses; (IV) hypopigmented der- 1 Institute of Dermatology, “Santa Maria matoses; (V) granulomatous dermatoses; (VI) sclerotic dermatoses; and della Misericordia University Hospital, Udine, Italy (VII) facial inflammatory dermatoses. Results: A total of 653 patients 2 Department of Dermatology, Venereology (541 and 112 with Phototype V and VI, respectively) were recruited and Leprosy, SN Medical College, for the analysis.