Nigeria Update to the IMB Nigeria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The World Bank Implementation Status & Results
The World Bank Report No: ISR4370 Implementation Status & Results Nigeria THIRD NATIONAL FADAMA DEVELOPMENT PROJECT (FADAMA III) (P096572) Operation Name: THIRD NATIONAL FADAMA DEVELOPMENT PROJECT Project Stage: Implementation Seq.No: 7 Status: ARCHIVED Archive Date: (FADAMA III) (P096572) Country: Nigeria Approval FY: 2009 Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Specific Investment Loan Implementing Agency(ies): National Fadama Coordination Office(NFCO) Key Dates Public Disclosure Copy Board Approval Date 01-Jul-2008 Original Closing Date 31-Dec-2013 Planned Mid Term Review Date 07-Nov-2011 Last Archived ISR Date 11-Feb-2011 Effectiveness Date 23-Mar-2009 Revised Closing Date 31-Dec-2013 Actual Mid Term Review Date Project Development Objectives Component(s) Component Name Component Cost Capacity Building, Local Government, and Communications and Information Support 87.50 Small-Scale Community-owned Infrastructure 75.00 Advisory Services and Input Support 39.50 Support to the ADPs and Adaptive Research 36.50 Asset Acquisition 150.00 Project Administration, Monitoring and Evaluation 58.80 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Satisfactory Satisfactory Overall Implementation Progress (IP) Satisfactory Satisfactory Overall Risk Rating Low Low Implementation Status Overview As at August 19, 2011, disbursement status of the project stands at 46.87%. All the states have disbursed to most of the FCAs/FUGs except Jigawa and Edo where disbursement was delayed for political reasons. The savings in FUEF accounts has increased to a total ofN66,133,814.76. 75% of the SFCOs have federated their FCAs up to the state level while FCAs in 8 states have only been federated up to the Local Government levels. -

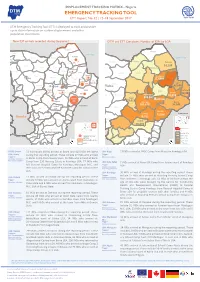
IOM Nigeria DTM Emergency Tracking Tool (ETT) Report No.78 (1-7
DISPLACEMENT TRACKING MATRIX - Nigeria DTM Nigeria EMERGENCY TRACKING TOOL (ETT) DTM Emergency Tracking Tool (ETT) is deployed to track and provide up-to-date information on sudden displacement and other population movements ETT Report: No. 78 1 – 7 August 2018 Movements New Arrival Screening by Nutri�on Partners Chad Niger Abadam Arrivals: Children (6-59 months) Lake Chad screened for malnutri�on 5,317 individuals 588 Mobbar Kukawa MUAC category of screened children 71 Departures: 72 Green: 329 Yellow: 115 Red: 144 Guzamala 28 1,177 individuals 770 Gubio Within the period of 1 – 7 August 2018, a total of 6,494 movements were Monguno Nganzai recorded, including 5,317 arrivals and 1,177 departures at loca�ons in 360 827 Marte Askira/Uba, Bama, Chibok, Damboa, Demsa, Dikwa, Fufore, Girei, Gombi, Magumeri Ngala 174 157 Kala/Balge Guzamala, Gwoza, Hawul, Hong, Kala/Balge, Konduga, Kukawa, Madagali, Mafa, Mafa Magumeri, Maiduguri, Maiha, Mayo-Belwa, Michika, Mobbar, Monguno, Jere Dikwa 9 366 11 Borno 12 Mubi-North, Mubi-South, Ngala, Nganzai, Numan, Yola-North and Yola-South Maiduguri Kaga Bama Local Government Areas (LGAs) of Adamawa and Borno States. Konduga 51 928 Assessments iden�fied the following main triggers of movements: ongoing Gwoza conflict (45%), poor living condi�ons (24%), voluntary reloca�on (9%), improved 532 security (7%), military opera�ons (6%), involuntary reloca�on (4%), fear of Damboa 7 a�acks/communal clashes (4%), and farming ac�vi�es (1%). 20 Madagali Biu Chibok Askira/Uba 179 Number of individuals by movement triggers -

Surviving Works: Context in Verre Arts Part One, Chapter One: the Verre
Surviving Works: context in Verre arts Part One, Chapter One: The Verre Tim Chappel, Richard Fardon and Klaus Piepel Special Issue Vestiges: Traces of Record Vol 7 (1) (2021) ISSN: 2058-1963 http://www.vestiges-journal.info Preface and Acknowledgements (HTML | PDF) PART ONE CONTEXT Chapter 1 The Verre (HTML | PDF) Chapter 2 Documenting the early colonial assemblage – 1900s to 1910s (HTML | PDF) Chapter 3 Documenting the early post-colonial assemblage – 1960s to 1970s (HTML | PDF) Interleaf ‘Brass Work of Adamawa’: a display cabinet in the Jos Museum – 1967 (HTML | PDF) PART TWO ARTS Chapter 4 Brass skeuomorphs: thinking about originals and copies (HTML | PDF) Chapter 5 Towards a catalogue raisonnée 5.1 Percussion (HTML | PDF) 5.2 Personal Ornaments (HTML | PDF) 5.3 Initiation helmets and crooks (HTML | PDF) 5.4 Hoes and daggers (HTML | PDF) 5.5 Prestige skeuomorphs (HTML | PDF) 5.6 Anthropomorphic figures (HTML | PDF) Chapter 6 Conclusion: late works ̶ Verre brasscasting in context (HTML | PDF) APPENDICES Appendix 1 The Verre collection in the Jos and Lagos Museums in Nigeria (HTML | PDF) Appendix 2 Chappel’s Verre vendors (HTML | PDF) Appendix 3 A glossary of Verre terms for objects, their uses and descriptions (HTML | PDF) Appendix 4 Leo Frobenius’s unpublished Verre ethnological notes and part inventory (HTML | PDF) Bibliography (HTML | PDF) This work is copyright to the authors released under a Creative Commons attribution license. PART ONE CONTEXT Chapter 1 The Verre Predominantly living in the Benue Valley of eastern middle-belt Nigeria, the Verre are one of that populous country’s numerous micro-minorities. -

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

Lessons from Colombia for Curtailing the Boko Haram Insurgency in Nigeria
Lessons From Colombia For Curtailing The Boko Haram Insurgency In Nigeria BY AFEIKHENA JEROME igeria is a highly complex and ethnically diverse country, with over 400 ethnic groups. This diversity is played out in the way the country is bifurcated along the lines of reli- Ngion, language, culture, ethnicity and regional identity. The population of about 178.5 million people in 2014 is made up of Christians and Muslims in equal measures of about 50 percent each, but including many who embrace traditional religions as well. The country has continued to experience serious and violent ethno-communal conflicts since independence in 1960, including the bloody and deadly thirty month fratricidal Civil War (also known as the Nigerian-Biafran war, 1967-70) when the eastern region of Biafra declared its seces- sion and which claimed more than one million lives. The most prominent of these conflicts recently pitch Muslims against Christians in a dangerous convergence of religion, ethnicity and politics. The first and most dramatic eruption in a series of recent religious disturbances was the Maitatsine uprising in Kano in December 1980, in which about 4,177 died. While the exact number of conflicts in Nigeria is unknown, because of a lack of reliable sta- tistical data, it is estimated that about 40 percent of all conflicts have taken place since the coun- try’s return to civilian rule in 1999.1 The increasing wave of violent conflicts across Nigeria under the current democratic regime is no doubt partly a direct consequence of the activities of ethno- communal groups seeking self-determination in their “homelands,” and of their surrogate ethnic militias that have assumed prominence since the last quarter of 2000. -
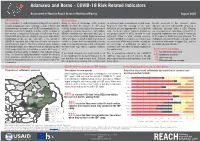
Adamawa and Borno - COVID-19 Risk Related Indicators
Adamawa and Borno - COVID-19 Risk Related Indicators Assessment of Hard-to-Reach Areas in Northeast Nigeria August 2020 Introduction Methodology The continuation of conflict in Northeast Nigeria has created a Using its Area of Knowledge (AoK) method, on settlement-wide circumstances in H2R areas. Results presented in this factsheet, unless complex humanitarian crisis, rendering sections of Borno and REACH monitors the situation in H2R areas Responses from KIs reporting on the same otherwise specified, represent the proportion of Adamawa states as hard to reach (H2R) for humanitarian actors. remotely through monthly multisector interviews in settlement are then aggregated to the settlement settlements assessed within a LGA. Findings Previous assessments illustrate how the conflict continues to accessible Local Government Area (LGA) capitals. level. The most common response provided by are only reported on LGAs where at least 5% of have severe consequences for people in H2R areas. People REACH interviews key informants (KIs) who 1) the greatest number of KIs is reported for each populated settlements and at least 5 settlements living in H2R areas, who are already facing severe and extreme are recently arrived internally displaced persons settlement. When no most common response in the respective LGA have been assessed. The humanitarian needs, are also vulnerable to the spread of (IDPs) who have left a H2R settlement in the last 3 could be identified, the response is considered as findings presented are indicative of broader trends COVID-19, especially due to the lack of health care services months, or 2) have been in contact with someone ‘no consensus’. While included in the calculations, in assessed settlements in August 2020, and are and information sources. -
ETT Report-No.32.V2
DISPLACEMENT TRACKING MATRIX - Nigeria DTM Nigeria EMERGENCY TRACKING TOOL ETT Report: No. 32 | 12–18 September 2017 IOM OIM DTM Emergency Tracking Tool (ETT) is deployed to track and provide up-to-date information on sudden displacement and other population movements New IDP arrivals recorded during the period DTM and ETT Cumulative Number of IDPs by LGA Abadam Abadam Yusufari Lake Chad Kukawa Yusufari Yunusari Mobbar Lake Chad± Nguru Karasuwa Niger Machina Yunusari Mobbar Abadam Kukawa Lake Chad Bade Guzamala 79 Nguru Karasuwa Kukawa Bursari 14,105 Geidam Gubio Bade Bade Guzamala Monguno Mobbar Nganzai Jakusko Bursari 6240 Marte Geidam Gubio Bade Guzamala Ngala Tarmua Monguno Magumeri Nganzai Jakusko Yobe 122,844 Marte 43 Gubio Monguno Jere Dikwa 7 Mafa Kala/BalgeYobe Ngala Maiduguri M.C. 122 Tarmua Nganzai Nangere Fune Damaturu Jigawa Magumeri 42,686 Borno 18 Yobe Marte Potiskum Ngala Kaga Konduga Bama Jere Mafa Kala/Balge Magumeri Dikwa 17 30 73 Yobe 49,480 Fika Gujba Nangere Fune Damaturu Maiduguri Mafa 74,858 Jere Dikwa Gwoza Potiskum Kaga Borno308,807 Kala-Balge MaiduBornoguri Damboa 799 19,619 KondugaKonduga Bama Gulani Cameroon Kag1a05,678 56,748 Chibok Konduga Fika Gujba Bama Biu 11 Madagali Askira/Uba Gwoza Michika Damboa Cameroon Kwaya Kusar 73,966Gwoza Hawul Damboa Bauchi Gombe Bayo Mubi North 76,795 Hong Gulani Shani Chibok Gombi Mubi South Madagali Biu Biu 16,378Chibok Maiha Askira/Uba Askira-Uba Inaccessible area Guyuk Song Michika Shelleng IDP severity Kwaya KusarKwaya Kusar Hawul Adamawa Hawul Less t han 10,788 Bauchi Gombe Bayo Mubi North Lamurde Number of new Bayo 10,788 - 25,813 HongAdamawa Numan Girei arrivals Shani Cameroon 25,813 - 56,749 Demsa Inaccessible area Shani Gombi Mubi South Yola South 56,749 - 122,770 Yola North Gombe 0 15 30 60 Km 122,770 Above Fufore LGAChad Adamawa Plateau Mayo-Belwa Shelleng Maiha Guyuk Song STATE: Borno 73 individuals (INDs) arrived at Bama and 129 INDs le� Bama LGA: Kaga 17 INDs arrived at NYSC Camp from Musari in Konduga LGA. -

How Boko Haram Became the Islamic State's West Africa
HOW BOKO HARAM BECAME THE ISLAMIC STATE’S WEST AFRICA PROVINCE J. Peter Pham ven before it burst into the headlines with its brazen April 2014 abduction of nearly three hundred schoolgirls from the town of Chibok in Nigeria’s northeast- Eern Borno State, sparking an unprecedented amount of social media communica- tion in the process, the Nigerian militant group Boko Haram had already distinguished itself as one of the fastest evolving of its kind, undergoing several major transformations in just over half a decade. In a very short period of time, the group went from being a small militant band focused on localized concerns and using relatively low levels of violence to a significant terrorist organization with a clearer jihadist ideology to a major insurgency seizing and holding large swathes of territory that was dubbed “the most deadly terrorist group in the world” by the Institute for Economics and Peace, based on the sheer number of deaths it caused in 2014.1 More recently, Boko Haram underwent another evolution with its early 2015 pledge of allegiance to the Islamic State and its subsequent rebranding as the “Islamic State West Africa Province” (ISWAP). The ideological, rhetorical, and operational choices made by Boko shifted consider- ably in each of these iterations, as did its tactics. Indeed the nexus between these three elements—ideology, rhetoric, and operations—is the key to correctly interpreting Boko Haram’s strategic objectives at each stage in its evolution, and to eventually countering its pursuit of these goals. Boko Haram 1.0 The emergence of the militant group that would become known as Boko Haram cannot be understood without reference to the social, religious, economic, and political milieu of J. -

FEWS NET Special Report: a Famine Likely Occurred in Bama LGA and May Be Ongoing in Inaccessible Areas of Borno State
December 13, 2016 A Famine likely occurred in Bama LGA and may be ongoing in inaccessible areas of Borno State This report summarizes an IPC-compatible analysis of Local Government Areas (LGAs) and select IDP concentrations in Borno State, Nigeria. The conclusions of this report have been endorsed by the IPC’s Emergency Review Committee. This analysis follows a July 2016 multi-agency alert, which warned of Famine, and builds off of the October 2016 Cadre Harmonisé analysis, which concluded that additional, more detailed analysis of Borno was needed given the elevated risk of Famine. KEY MESSAGES A Famine likely occurred in Bama and Banki towns during 2016, and in surrounding rural areas where conditions are likely to have been similar, or worse. Although this conclusion cannot be fully verified, a preponderance of the available evidence, including a representative mortality survey, suggests that Famine (IPC Phase 5) occurred in Bama LGA during 2016, when the vast majority of the LGA’s remaining population was concentrated in Bama Town and Banki Town. Analysis indicates that at least 2,000 Famine-related deaths may have occurred in Bama LGA between January and September, many of them young children. Famine may have also occurred in other parts of Borno State that were inaccessible during 2016, but not enough data is available to make this determination. While assistance has improved conditions in accessible areas of Borno State, a Famine may be ongoing in inaccessible areas where conditions could be similar to those observed in Bama LGA earlier this year. Significant assistance in Bama Town (since July) and in Banki Town (since August/September) has contributed to a reduction in mortality and the prevalence of acute malnutrition, though these improvements are tenuous and depend on the continued delivery of assistance. -

Rainfall and the Length of the Growing Season in Nigeria
INTERNATIONAL JOURNAL OF CLIMATOLOGY Int. J. Climatol. 24: 467–479 (2004) Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/joc.1012 RAINFALL AND THE LENGTH OF THE GROWING SEASON IN NIGERIA T. O. ODEKUNLE* Department of Geography, Obafemi Awolowo University, Ile-Ife, Nigeria Received 15 May 2003 Revised 8 December 2003 Accepted 16 December 2003 ABSTRACT This study examines the length of the growing season in Nigeria using the daily rainfall data of Ikeja, Ondo, Ilorin, Kaduna and Kano. The data were collected from the archives of the Nigerian Meteorological Services, Oshodi, Lagos. The length of the growing season was determined using the cumulative percentage mean rainfall and daily rainfall probability methods. Although rainfall in Ikeja, Ondo, Ilorin, Kaduna, and Kano appears to commence around the end of the second dekad of March, middle of the third dekad of March, mid April, end of the first dekad of May, and early June respectively, its distribution characteristics at the respective stations remain inadequate for crop germination, establishment, and development till the end of the second dekad of May, early third dekad of May, mid third dekad of May, end of May, and end of the first dekad of July respectively. Also, rainfall at the various stations appears to retreat starting from the early third dekad of October, early third dekad of October, end of the first dekad of October, end of September, and early second dekad of September respectively, but its distribution characteristics only remain adequate for crop development at the respective stations till around the end of the second dekad of October, end of the second dekad of October, middle of the first dekad of October, early October, and middle of the first dekad of September respectively. -

Chibok Girls/ #Bringbackourgirls/ Stolen
TRANSFORMING FEMALE ABDUCTION VICTIMS TO MENTORS USING SURVIVOR CENTERED APPROACH: DISCUSSING "CHIBOK GIRLS/ #BRINGBACKOURGIRLS/ STOLEN DAUGHTERS" AS A CASE STUDY by ENEKOLE ATABO A THESIS Presented to the Conflict and Dispute Resolution Program and the Graduate School of the University of Oregon in partial fulfillment of the requirements for the degree of Master of Science June 2019 THESIS APPROVAL PAGE Student: Enekole Atabo Title: Transforming Female Abduction Victims to Mentors using Survivor Centered Approach: Discussing "Chibok Girls/ #BringBackOurGirls/ Stolen Daughters" as a case study This thesis has been accepted and approved in partial fulfillment of the requirements for the Master of Science degree in the Conflict and Dispute Resolution Program by: Prof. Merle Weiner Chairperson Prof. Ibrahim Gassama Member Dr. Christina O’Bryan Member and Janet Woodruff-Borden Vice Provost and Dean of the Graduate School Original approval signatures are on file with the University of Oregon Graduate School. Degree awarded June 2019 ii © 2019 Enekole Atabo iii THESIS ABSTRACT Enekole Atabo Master of Science Conflict and Dispute Resolution June 2019 Title: Transforming Female Abduction Victims to Mentors using Survivor Centered Approach: Discussing "Chibok Girls/ #BringBackOurGirls/ Stolen Daughters" as a case study Generally, women and girls are discriminated against based on gender, education, religion, or culture. Some of these characteristics are either ascribed or achieved. Life chances or the ability to improve one’s quality of life depends on the intersectionality of the different forms of oppression. Education which is one important means to improve life chances has often been targeted by religious and cultural ideology to the extent that girls are severely punished for defying restrictions on women’s education. -

Nigeria's Boko Haram
Nigeria’s Boko Haram: Frequently Asked Questions Lauren Ploch Blanchard Specialist in African Affairs March 29, 2016 Congressional Research Service 7-5700 www.crs.gov R43558 Nigeria’s Boko Haram: Frequently Asked Questions Summary Boko Haram, a violent Nigerian Islamist movement, has grown increasingly active and deadly in its attacks against state and civilian targets in recent years, drawing on a narrative of victimization and vengeance for state abuses to elicit recruits and sympathizers. The group’s April 2014 abduction of almost 300 schoolgirls drew particular international attention, including from the Obama Administration and Members of Congress. Its high death toll and its pledge of allegiance to the Islamic State (IS, also known as ISIL or ISIS) in March 2015 have further raised the concern of U.S. policy makers. The group has sought to rebrand itself as the Islamic State’s West Africa Province (ISWAP), though it remains more popularly known by its original nickname. The State Department has named several individuals linked to Boko Haram, including its leader, Abubakar Shekau, as Specially Designated Global Terrorists, and the group was designated as a Foreign Terrorist Organization (FTO) by the State Department in November 2013. More than 15,000 people are estimated to have been killed by Boko Haram, including more than 6,000 in 2015 alone, making it one of world’s deadliest terrorist groups. By U.N. estimates, roughly 2.8 million people have been displaced by Boko Haram-related violence in the Lake Chad Basin region, where approximately 5.6 million are in need of emergency food aid.