XERGIC 1. Product Name 2. Qualitative and Quantitative
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Application A603 Supporting Document 3 FOOD TECHNOLOGY
Application A603 Supporting Document 3 FOOD TECHNOLOGY REPORT Summary The Applicant, Golding Handcrafts, claims that there is a technical need to extend the use of the red food colouring erythrosine in Australia and New Zealand from preserved cherries to food colouring preparations used to colour icing and other cake decorations for the technological purpose of achieving colour enhancement. This has been substantiated with claims that food colourings preparations containing erythrosine possess superior colouring characteristics to alternative red food colourings including colour strength, longevity, lack of bleeding and quality of the finished product. Consequently this allow for a greater range of colouring effects to be achieved including wider ranges of pinks, lavenders, violets, royal blue and true black. The Applicant notes that commercial products are currently available for this purpose in the United States of America (USA) and seeks to import and sell these colourings preparations for cake icing and related products for use in Australia and New Zealand. The merit of using erythrosine is strongly supported by some companies, in particular, AmericolorTM Corporation and CK Products, two of the largest companies who use erythrosine in products for cake decorating purposes. They have advised the Applicant that the purpose of adding erythrosine to food is to achieve a precise visual effect and unique shades which are unattainable by using any other food colours. The colour hue and intensity is directly affected by the amounts of erythrosine added and the proposed amounts are consistent in achieving the intended result – to colour the food. Colour combinations are individually weighed and added to the mix for each single recipe so that a consistent final effect is obtained. -

Artificial Food Colours and Children Why We Want to Limit and Label Foods Containing the ‘Southampton Six’ Food Colours on the UK Market Post-Brexit
Artificial food colours and children Why we want to limit and label foods containing the ‘Southampton Six’ food colours on the UK market post-Brexit November 2020 FIRST STEPS NUTRITIONArtificial food coloursTRUST and children: page Artificial food colours and children: Why we want to limit and label foods containing the‘Southampton Six’ food colours on the UK market post-Brexit November 2020 Published by First Steps Nutrition Trust. A PDF of this resource is available on the First Steps Nutrition Trust website. www.firststepsnutrition.org The text of this resource, can be reproduced in other materials provided that the materials promote public health and make no profit, and an acknowledgement is made to First Steps Nutrition Trust. This resource is provided for information only and individual advice on diet and health should always be sought from appropriate health professionals. First Steps Nutrition Trust Studio 3.04 The Food Exchange New Covent Garden Market London SW8 5EL Registered charity number: 1146408 First Steps Nutrition Trust is a charity which provides evidence-based and independent information and support for good nutrition from pre-conception to five years of age. For more information, see our website: www.firststepsnutrition.org Acknowledgements This report was written by Rachael Wall and Dr Helen Crawley. We would like to thank Annie Seeley, Sarah Weston, Erik Millstone and Anna Rosier for their help and support with this report. Artificial food colours and children: page 1 Contents Page Executive summary 3 Recommendations -

Regulatory Information Sheet
Regulatory Information Sheet Approved Drug Colourants Listed by the European Union Colour Index Colour E Number Alternate Names Number Allura Red AC (a) E129 16035 FD&C Red #40 Aluminum*** E173 77000 -- Amaranth*** (a) E123 16185 Delisted FD&C Red #2 Annatto*** E160b 75120 Bixin, norbixin Anthocyanins (a) E163 -- -- Beetroot Red E162 -- Betanin Beta APO-8´-Carotenal E160e 40820 -- Brilliant Black BN (a) E151 28440 Black BN Brilliant Blue FCF (a) E133 42090 FD&C Blue #1 Brown HT (a) E155 20285 -- Calcium Carbonate E170 77220 -- Canthaxanthin* E161g 40850 -- Caramel,-Plain E150a -- -- Caramel,-Caustic Sulphite E150b -- -- Caramel,-Ammonia E150c -- -- Caramel, Sulphite Ammonia E150d -- -- Carmine (a) E120 75470 Carminic Acid, Cochineal Carmoisine (a) E122 14720 Azorubine Carotenes E160a 40800 / 75130 -- Chlorophylls/Chlorophyllins E140 75810 / 75815 -- Copper Complexes of E141 75815 -- Chlorophylls/Chlorophyllins(a) Curcumin (a) E100 75300 Turmeric Erythrosine*** (a) E127 45430 FD&C Red #3 Gold*** E175 77480 -- Green S (a) E142 44090 Acid Brilliant Green BS Indigotine (a) E132 73015 FD&C Blue #2, Indigo Carmine 77491 / 77492 / Iron Oxides & Hydroxides E172 Iron Oxide Red, Yellow, Black 77499 Litholrubine BK*** (a) E180 -- -- Lutein E161b -- -- Lycopene*** E160d 75125 -- Paprika Extract E160c -- Capsanthin, Capsorubin Patent Blue V (a) E131 42051 Acid Blue 3 Ponceau 4R (a) E124 16255 Cochineal Red A Page 1 of 2 Document Reference No.: GLO-10107, revision 2 Effective Date: September 2014 Reviewed Date: November 2017 This document is valid at the time of distribution. Distributed 24-Sep-2021 (UTC) E Colour Index Colour Alternate Names Number Number Quinoline Yellow** (a) E104 47005 China Yellow Riboflavins (a) E101 -- -- Silver*** E174 -- -- Sunset Yellow FCF (a) E110 15985 FD&C Yellow #6, Orange Yellow S Tartrazine (a) E102 19140 FD&C Yellow #5 Titanium Dioxide E171 77891 -- Vegetable Carbon E153 77268:1 Carbo Medicinalis Vegetalis The above list is derived from Part B, List of All Additives, from Annex II to Regulation (EC) No 1333/2008 on food additives. -

Role of Microorganisms in Biodegradation of Food Additive Azo Dyes: a Review
Vol. 19(11), pp.799-805, November, 2020 DOI: 10.5897/AJB2020.17250 Article Number: F63AA1865367 ISSN: 1684-5315 Copyright ©2020 Author(s) retain the copyright of this article African Journal of Biotechnology http://www.academicjournals.org/AJB Review Role of microorganisms in biodegradation of food additive Azo dyes: A review Fatimah Alshehrei Department of Biology, Jamum College University, Umm AlQura University, Makkah24382, Saudi Arabia. Received 22 September, 2020; Accepted 27 October, 2020 Food additives Azo dyes are synthetic compounds added to foods to impart color and improve their properties. Some azo dyes have been banned as food additives due to toxic, mutagenic, and carcinogenic side effects. Long exposure to foods containing azo dye leads to chronic toxicity. Some microorganisms are capable to degrade these dyes and convert them to aromatic amines. In human body, microbiota can play a vital role in biodegradation of azo dyes by producing azo reductase. Aromatic amines are toxic, water-soluble and well absorbed via human intestine. In the current study, the role of microorganisms in biodegradation of six dyes related to azo group was discussed. These dyes are: Tartrazine E102, Sunset Yellow E110, Ponceau E124, Azorubine E122, Amaranth E123, and Allura Red E129 which are classified as the most harmful food additive dyes. Key word: Food additive, azo dyes, microorganisms, azo reductase, aromatic amines. INTRODUCTION Food additives are synthetic compounds added to food In the USA and European countries, some azo dyes have for many proposes such as maintaining the product from been banned as food additives due to toxic, mutagenic, deterioration or improving its safety, freshness, taste, and carcinogenic side effects (Chung, 2000). -

Food Additives As Inhibitors of Intestinal Drug Transporter Oatp2b1
1 FOOD ADDITIVES AS INHIBITORS OF INTESTINAL DRUG TRANSPORTER OATP2B1 Alli Tikkanen1, Estelle Pierrot1, Feng Deng1,2, Virginia Barras Sánchez1, Marja Hagström1, Jan B. Koenderink3, Heidi Kidron1* 1Division of Pharmaceutical Biosciences, Faculty of Pharmacy, University of Helsinki, P.O. Box 56, 00014 Helsinki, Finland 2 Current address: Department of Clinical Pharmacology, Faculty of Medicine, University of Helsinki 3 Radboud University Medical Center, Department of Pharmacology and Toxicology, Nijmegen, The Netherlands *corresponding author Telephone: +358405666660 Email: [email protected] 2 FOR TABLE OF CONTENTS USE ONLY FOOD ADDITIVES AS INHIBITORS OF INTESTINAL DRUG TRANSPORTER OATP2B1 Alli Tikkanen, Estelle Pierrot, Feng Deng, Virginia Barras Sánchez, Marja Hagström, Jan B. Koenderink, Heidi Kidron 3 ABSTRACT Food additives are compounds that are added to food and beverage to improve taste, color, preservation or composition. Generally, food additives are considered safe for human use due to safety evaluation conducted by food safety authorities and high safety margins applied to permitted usage levels. However, the interaction potential of food additives with simultaneously administered medication has not received much attention. Even though many food additives are poorly absorbed into systemic circulation, high concentrations could exist in the intestinal lumen making intestinal drug transporters, such as the uptake transporter organic anion transporting polypeptide 2B1 (OATP2B1), a possible site of food additive–drug interaction. In the present work, we aimed to characterize the interaction of a selection of 25 food additives including colorants, preservatives and sweeteners with OATP2B1 in vitro. In HEK293 cells transiently overexpressing OATP2B1 or control, uptake of dibromofluorescein was studied with and without 50 µM food additive at pH 7.4. -
Automation of AOAC 988.13 for the Identification of FD&C Color
May, 2012 Automation of AOAC 988.13 for the Identification of FD&C Color Additives in Foods using Solid Phase Extraction Application Note FB0112 Keywords GX-274 ASPEC™, AOAC, Spectrophotometer, Food and Beverage, Solid Phase Extraction, SPE, Color Additives, FD&C, FDA, TRILUTION ® LH, Liquid Handling Introduction A color additive is any dye, pigment or other substance which imparts color to a food, drug or cosmetic or to the human body (1). Color additives for food are commonly found in expected places, such as candies and powdered drink mixes, but also can be added to fruit skins to make them look more appealing. The addition of synthetic color additives is regulated closely by the FDA and is examined from the manufacturing of the pigment itself, through to its use and appropriate product labeling. Color additives have come under scrutiny recently because of their potential adverse physical and mental health effects that may be linked to ingestion, especially in children. AOAC method 988.13 qualitatively tests for the presence of eight synthetic color additives, one of which is now banned. These color additives are FD&C colors approved for use in food, drugs and cosmetics. Additives are extracted from the sample matrix using solid phase extraction (SPE), and then identified by spectrum analysis on a spectrophotometer. The color additives examined by the method – FD&C Red Nos. 3 and 40, Blue Nos. 1 and 2, Yellow Nos. 5 and 6, Green No. 3 and the now banned Red No. 2 – are listed in Table 1, along with the E Number used in the EU and UK, common chemical name and chemical structure. -

Tattoos and Permanent Make-Up State of Play and Trends in Tattoo Practices
Safety of tattoos and permanent make-up State of play and trends in tattoo practices Report on Work Package 2 Administrative Arrangement N. 2014 -33617 Analysis conducted on behalf of DG JUST Paola Picc inini, Laura Contor, Sazan Pakalin, Tim Raemaekers, Chiara Senaldi 2 0 1 5 LIMITED ReportDISTRIBUTION EUR 27528 EN This publication is a Technical report by the Joint Research Centre, the European Commission’s in-house science service. It aims to provide evidence-based scientific support to the European policy-making process. The scientific output expressed does not imply a policy position of the European Commission. Neither the European Commission nor any person acting on behalf of the Commission is responsible for t he use which might be made of this publication. JRC Science Hub https://ec.europa.eu/jrc JRC96808 EUR 27528 EN ISBN 978-92-79-52789-0 (PDF) ISSN 1831-9424 (online) doi:10.2788/924128 (online) © European Union, 2015 Reproduction is authorised provided the source is acknowledged. All images © European Union 2015, except: [cover page, Kolidzei, image #65391434], 2015. Source: [Fotolia.com] How to cite: Authors; title; EUR; doi (Paola Piccinini, Laura Contor, Sazan Pakalin, Tim Raemaekers, Chiara Senaldi; Safety of tattoos and permanent make-up. State of play and trends in tattoo practices; EUR 27528 EN ; 10.2788/924128) Safety of tattoos and permanent make-up State of play and trends in tattoo practices Table of contents Abstract 1 1. Introduction 3 2. Tattoos and Permanent Make-up Project 4 3. Methodology 5 3.1 Questionnaires 5 3.2 Web search 7 3.3 RAPEX notifications 7 3.4 National studies and surveys 8 3.5 Literature 8 3.6 Presentations 8 4. -
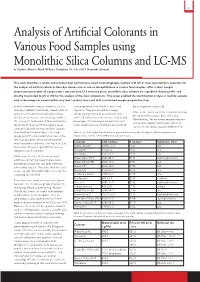
Analysis of Artificial Colorants in Various Food Samples Using Monolithic Silica Columns and LC-MS by Stephan Altmaier, Merck Millipore, Frankfurter Str
31 Analysis of Artificial Colorants in Various Food Samples using Monolithic Silica Columns and LC-MS by Stephan Altmaier, Merck Millipore, Frankfurter Str. 250, 64293 Darmstadt, Germany This work describes a simple and sensitive high performance liquid chromatography method with UV or mass spectrometry detection for the analysis of artificial colorants from dye classes such as azo or chinophthalone in various food samples. After a short sample preparation procedure all samples were separated on C18 reversed phase monolithic silica columns via a gradient elution profile and directly transferred to UV or MS for the analysis of the main components. This setup enabled the identification of dyes in real life samples such as beverages or sweets within very short analysis times and with a minimised sample preparation step. In the nineteenth century chemicals such as azo compounds (see Tables 1 and 2 and by an organism very easily. mercury sulphide, lead oxide, copper salts or Figure 1). They are utilised as a single Most of the current artificial colorants can now fuchsine were utilised to artificially colour colouring ingredient or as a mixture with be replaced by natural dyes very easily. food such as cheese, confectionary, pickles other colorants in a wide variety of foods and Nevertheless, for economic reasons they are [1] or wine [2]. In the end of that century the beverages. All listed dyes are nontoxic and still used to improve the attractiveness of discovery of many synthetic organic food water soluble and can therefore be excreted sweets or soft drinks towards children or of colorants allowed for more brilliant colours than traditional natural dyes. -

FDA Regulation of Color Additives in Drug Products
FDA Regulation of Color Additives in Drug Products Bhakti Petigara Harp, Ph.D. Office of Cosmetics and Colors Center for Food Safety and Applied Nutrition Food and Drug Administration Learning Objectives • Recognize a color additive • Describe color additive petition process • Identify certification exempt color additives • Identify certified color additives • Summarize certification process for color additives • Identify enforcement tools 2 Definition of Color Additive • A color additive is a substance that imparts color to a food, drug, cosmetic, or medical device • FDA has regulatory responsibilities for all of these products when they are marketed in the U.S. • FDA must pre-approve the color additives used in FDA-regulated products 3 Ideal Properties of Color Additives • Non-toxic and no physiological activity • High coloring power so only small quantity needed • Stable – Not light sensitive – Not temperature sensitive – pH stable • Free from taste or odor • Water or oil soluble depending on formulation 4 Types of Color Additives • Dyes and pigments • Inorganic and mineral compounds • Plant and animal sources • Lakes – insoluble pigments formed from water- soluble dyes, precipitants, and substrata • Mixtures – color additives made by mixing multiple color additives and one or more diluents – Diluents facilitate the use of mixtures in products – Listed for drug use under 21 CFR 73.1001 • Injected drugs • Branding inks • Externally applied drugs 5 Permitted Uses for Color Additives in Drugs • General use • Ingested drugs • External -

Finrep FAD-2010-0347 Allura Red AC Sensient
Ref. Ares(2019)1685502 - 14/03/2019 EUROPEAN COMMISSION JOINT RESEARCH CENTRE Directorate F - Health, Consumers & Reference Materials (Geel/Ispra) European Union Reference Laboratory for Feed Additives JRC.F.5/CvH/ZE/AS/Ares Subject: Addendum to the EURL evaluation reports References: FAD-2010-0342 Tartrazine (JRC.D.5/CvH/ZE/mds/ Ares(2016)2938957) FAD-2010-0348 Carmoisine (JRC.DG.D.6/CvH/RM/ag/ARES(2011)991812) FAD-2010-0349 Ponceau 4R (JRC.D.5/SFB/CvH/JK/ag/Ares(2012)1483410) FAD-2010-0382 Erythrosine (JRC.DG.D.6/CvH/RM/ag/ARES(2011)861655) FAD-2010-0347 Allura Red AC (JRC.DG.D.6/CvH/RM/ag/ARES(2011)991812) FAD-2010-0346 Indigo Carmine (JRC.DG.D.6/CvH/RM/ag/ARES(2011)861655) FAD-2010-0351 Brilliant Blue FCF (JRC.D.5/SFB/CvH/ZE/ag/Ares(2012)1483410) Upon the requests from DG SANTE [1, 2], the EURL evaluated the supplementary information provided [3-11] in the frame of the following feed additive dossiers: 2010-0342, 2010-0348, 2010-0349, 2010-0382, 2010-0347, 2010-0346 and 2010-0351 for the analysis of Tartrazine, Carmoisine, Ponceau 4R, Erythrosine, Allura Red AC, Indigo Carmine and Brilliant Blue FCF in feedingstuffs, respectively. For the quantification of the above mentioned colourants the Applicant submitted a multi-analyte single-laboratory validated and further verified method based on high performance liquid chromatography coupled to tandem mass spectrometry (LC-MS/MS) [3]. The sample (5 g) is sonicated with mixture of methanol, aqueous bicarbonate solution and acetonitrile, shaken and centrifuged. -

Determination of Synthetic Food Colors, Caffeine, Sodium Benzoate and Potassium Sorbate in Sports Drinks
Moghaddam et al Tropical Journal of Pharmaceutical Research January 2016; 15 (1): 183-188 ISSN: 1596-5996 (print); 1596-9827 (electronic) © Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, 300001 Nigeria. All rights reserved. Available online at http://www.tjpr.org http://dx.doi.org/10.4314/tjpr.v15i1.25 Original Research Article Determination of Synthetic Food Colors, Caffeine, Sodium Benzoate and Potassium Sorbate in Sports Drinks Fatemeh Zamani Mazdeh1, Zeinab Moradi1, Ghazaleh Moghaddam1, Zhila Moradi-Khatoonabadi1, Farideh Esmaeili Aftabdari1, Parnaz Badaei2 and Mannan Hajimahmoodi1,2* 1Food and Drug Administration, 2Department of Drug and Food Control, Faculty of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran *For correspondence: Email: Received: 26 February 2015 Revised accepted: 11 November 2015 Abstract Purpose: To employ high performance liquid chromatography (HPLC) techniques to determine edible additives in commercial sports drinks. Methods: A total of 105 samples including 21 different brands of sports drinks were purchased from markets in Tehran, Iran. The process conditions included a C18 column, a mobile phase consisting of aqueous ammonium acetate buffer (pH = 4.2) and acetonitrile (80:20 v/v) at a flow rate of 0.8 ml min–1. The injection volume was 20 μL and the UV detector was set at 225 nm. Results: Mean recovery was between 95 and 106 %. The mean concentrations of sodium benzoate and potassium sorbate in Iranian brands (147.72 and 11.54 ppm, respectively) were significantly higher than in foreign brands (19.43 and 4.91 ppm, respectively, p < 0.05). The maximum amount of sodium benzoate and potassium sorbate was 251.50 ± 18.69 and 96.38 ± 38.56 ppm, respectively, while caffeine content was in the range of 293.48 ± 14.33 - 607.32 ± 135.33 ppm. -

Technological Applications of Natural Colorants in Food Systems: a Review
foods Review Technological Applications of Natural Colorants in Food Systems: A Review Ivan Luzardo-Ocampo 1 , Aurea K. Ramírez-Jiménez 2 , Jimena Yañez 2 , Luis Mojica 3 and Diego A. Luna-Vital 2,* 1 Instituto de Neurobiología, Universidad Nacional Autónoma de México (UNAM), Santiago de Querétaro, QRO 76230, Mexico; [email protected] 2 Tecnologico de Monterrey, School of Engineering and Science, Avenida Eugenio Garza Sada 2501 Sur, Monterrey, N. L. 64849, Mexico; [email protected] (A.K.R.-J.); [email protected] (J.Y.) 3 Tecnología Alimentaria, Centro de Investigación y Asistencia en Tecnología y Diseño del Estado de Jalisco (CIATEJ), A. C., Camino Arenero #1227 Col. El Bajío, Zapopan, JAL 45019, Mexico; [email protected] * Correspondence: [email protected] Abstract: Natural colorants have emerged as an alternative to their synthetic counterparts due to an existing health concern of these later. Moreover, natural-food colorants are a renewable option providing health benefits and interesting technological and sensory attributes to the food systems containing them. Several sources of natural colorants have been explored aiming to deliver the required wide color range demanded by consumers. This review aimed to compare and discuss the technological applications of the main natural-food colorants into food system in the last six years, giving additional information about their extraction process. Although natural colorants are promising choices to replace synthetic ones, optimization of processing conditions, research on new sources, and new formulations to ensure stability are required to equate their properties to their Citation: Luzardo-Ocampo, I.; synthetic counterparts. Ramírez-Jiménez, A.K.; Yañez, J.; Mojica, L.; Luna-Vital, D.A.