Advances in Clinical and Experimental Medicine 2020, Vol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Final Program of CCC2020
第三十九届中国控制会议 The 39th Chinese Control Conference 程序册 Final Program 主办单位 中国自动化学会控制理论专业委员会 中国自动化学会 中国系统工程学会 承办单位 东北大学 CCC2020 Sponsoring Organizations Technical Committee on Control Theory, Chinese Association of Automation Chinese Association of Automation Systems Engineering Society of China Northeastern University, China 2020 年 7 月 27-29 日,中国·沈阳 July 27-29, 2020, Shenyang, China Proceedings of CCC2020 IEEE Catalog Number: CFP2040A -USB ISBN: 978-988-15639-9-6 CCC2020 Copyright and Reprint Permission: This material is permitted for personal use. For any other copying, reprint, republication or redistribution permission, please contact TCCT Secretariat, No. 55 Zhongguancun East Road, Beijing 100190, P. R. China. All rights reserved. Copyright@2020 by TCCT. 目录 (Contents) 目录 (Contents) ................................................................................................................................................... i 欢迎辞 (Welcome Address) ................................................................................................................................1 组织机构 (Conference Committees) ...................................................................................................................4 重要信息 (Important Information) ....................................................................................................................11 口头报告与张贴报告要求 (Instruction for Oral and Poster Presentations) .....................................................12 大会报告 (Plenary Lectures).............................................................................................................................14 -

YAO-DISSERTATION-2016.Pdf
CONSUMING SCIENCE: A HISTORY OF SOFT DRINKS IN MODERN CHINA A Dissertation Presented to The Academic Faculty by Liang Yao In Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the School of History and Sociology Georgia Institute of Technology May 2016 COPYRIGHT © 2015 BY LIANG YAO CONSUMING SCIENCE: A HISTORY OF SOFT DRINKS IN MODERN CHINA Approved by: Dr. Hanchao Lu, Advisor Dr. Laura Bier School of History and Sociology School of History and Sociology Georgia Institute of Technology Georgia Institute of Technology Dr. John Krige Dr. Kristin Stapleton chool of History and Sociology History Department Georgia Institute of Technology University at Buffalo Dr. Steven Usselman chool of History and Sociology Georgia Institute of Technology Date Approved: December 2, 2015 ACKNOWLEDGEMENTS I would never have finished my dissertation without the guidance, help, and support from my committee members, friends, and family. Firstly, I would like to express my deepest gratitude to my advisor Professor Hanchao Lu for his caring, continuous support, and excellent intellectual guidance in all the time of research and writing of this dissertation. During my graduate study at Georgia Tech, Professor Lu guided me where and how to find dissertation sources, taught me how to express ideas and write articles like a historian. He provided me opportunities to teach history courses on my own. He also encouraged me to participate in conferences and publish articles on journals in the field. His patience and endless support helped me overcome numerous difficulties and I could not have imagined having a better advisor and mentor for my doctorial study. -

Xi Jinping and the Party Apparatus
Miller, China Leadership Monitor, No. 25 Xi Jinping and the Party Apparatus Alice Miller In the six months since the 17th Party Congress, Xi Jinping’s public appearances indicate that he has been given the task of day-to-day supervision of the Party apparatus. This role will allow him to expand and consolidate his personal relationships up and down the Party hierarchy, a critical opportunity in his preparation to succeed Hu Jintao as Party leader in 2012. In particular, as Hu Jintao did in his decade of preparation prior to becoming top Party leader in 2002, Xi presides over the Party Secretariat. Traditionally, the Secretariat has served the Party’s top policy coordinating body, supervising implementation of decisions made by the Party Politburo and its Standing Committee. For reasons that are not entirely clear, Xi’s Secretariat has been significantly trimmed to focus solely on the Party apparatus, and has apparently relinquished its longstanding role in coordinating decisions in several major sectors of substantive policy. Xi’s Activities since the Party Congress At the First Plenum of the Chinese Communist Party’s 17th Central Committee on 22 October 2007, Xi Jinping was appointed sixth-ranking member of the Politburo Standing Committee and executive secretary of the Party Secretariat. In December 2007, he was also appointed president of the Central Party School, the Party’s finishing school for up and coming leaders and an important think-tank for the Party’s top leadership. On 15 March 2008, at the 11th National People’s Congress (NPC), Xi was also elected PRC vice president, a role that gives him enhanced opportunity to meet with visiting foreign leaders and to travel abroad on official state business. -

An "Exceedingly Delicate Undertaking": Sino-American
An "exceedingly delicate undertaking": Sino-American science diplomacy, 1966–78 LSE Research Online URL for this paper: http://eprints.lse.ac.uk/102296/ Version: Accepted Version Article: Millwood, Peter (2019) An "exceedingly delicate undertaking": Sino-American science diplomacy, 1966–78. Journal of Contemporary History. ISSN 0022-0094 (In Press) Reuse Items deposited in LSE Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the LSE Research Online record for the item. [email protected] https://eprints.lse.ac.uk/ An “Exceedingly Delicate Undertaking”: Sino-American Science Diplomacy, 1966–78 Pete Millwood International History Department, London School of Economics In the first half of the twentieth century, China sought to modernize through opening to the world. Decades of what would become a century of humiliation had disabused the country of its previous self-perceived technological superiority, as famously expressed by Emperor Qianlong to the British envoy George Macartney in 1793. The Chinese had instead become convinced that they needed knowledge from outside to become strong enough to resist imperial aggression. No country encouraged this opening more than the United States. Americans threw money and expertise at the training of Chinese students and intellectuals. The Rockefeller Foundation’s first major overseas project was the creation of China’s finest medical college and other US institutions followed Rockefeller’s lead by establishing dozens of Chinese universities and technical schools to train a new generation of Chinese scientists. -

The CCP Central Committee's Leading Small Groups Alice Miller
Miller, China Leadership Monitor, No. 26 The CCP Central Committee’s Leading Small Groups Alice Miller For several decades, the Chinese leadership has used informal bodies called “leading small groups” to advise the Party Politburo on policy and to coordinate implementation of policy decisions made by the Politburo and supervised by the Secretariat. Because these groups deal with sensitive leadership processes, PRC media refer to them very rarely, and almost never publicize lists of their members on a current basis. Even the limited accessible view of these groups and their evolution, however, offers insight into the structure of power and working relationships of the top Party leadership under Hu Jintao. A listing of the Central Committee “leading groups” (lingdao xiaozu 领导小组), or just “small groups” (xiaozu 小组), that are directly subordinate to the Party Secretariat and report to the Politburo and its Standing Committee and their members is appended to this article. First created in 1958, these groups are never incorporated into publicly available charts or explanations of Party institutions on a current basis. PRC media occasionally refer to them in the course of reporting on leadership policy processes, and they sometimes mention a leader’s membership in one of them. The only instance in the entire post-Mao era in which PRC media listed the current members of any of these groups was on 2003, when the PRC-controlled Hong Kong newspaper Wen Wei Po publicized a membership list of the Central Committee Taiwan Work Leading Small Group. (Wen Wei Po, 26 December 2003) This has meant that even basic insight into these groups’ current roles and their membership requires painstaking compilation of the occasional references to them in PRC media. -

Comrade Chou En-Lal Great Proletarian Reyolutionary of The
China Reconstructs Eternal Glory to Comrade Chou En-lal Great Proletarian ReYolutionary of the Chinese People and Outstanding Communist Fighter! Supplement COMRADE CHOU EN-LAI PASSES AWAY Obituary Notice Issued by CPC Central Committee, NPC Standing Committee and State Council "pHE Central Committee of the' Communist Party of treatment, Comrade Chou En-lai, the great fighter of China, the Standing'Committee of the Notional the Chinese people, left us forever. His death is a People's Congress and the State Council of the Peo gigantic loss to our Party, our army and the people of ple's Republic of China announce with deepest grief: our country, to the cause of China's socialist revolu Comrade Chou En-lai, Member of the CPC Central tion and construction, to the international cause of opposing imperialism, colonialism and hegemonism, Committee, Member of the Political Bureau of the and to the cause of the international communist CPC Central Committee, Member of the Standing movement. Committee of the Political Bureau of the CPC Central Committee, Vice-Chairman of the CPC Central Com Comrade Chou En-lai was loyal to the Party and mittee, Premier of the State Council of the People's Re the people. Fighting heroically and working with utter public of China and Chairman of the Notional Com devotion, he selflessly dedicated all his energies mittee of the Chinese People's Political Consultative throughout his life to the implementation of Chairman Conference, died of cancer at 09:57 hours on January Mao's proletarian revolutionary line and to the victory 8, 1976, in Peking at the age of 78. -

November 11, 1965 Record of Second Conversation of Premier Zhou Enlai and Vice Premier Chen Yi with Foreign Minister Pak Seong- Cheol
Digital Archive digitalarchive.wilsoncenter.org International History Declassified November 11, 1965 Record of Second Conversation of Premier Zhou Enlai and Vice Premier Chen Yi with Foreign Minister Pak Seong- cheol Citation: “Record of Second Conversation of Premier Zhou Enlai and Vice Premier Chen Yi with Foreign Minister Pak Seong-cheol,” November 11, 1965, History and Public Policy Program Digital Archive, PRC FMA 106-01476-06, 70-117. Translated by Stephen Mercado. http://digitalarchive.wilsoncenter.org/document/118693 Summary: Chen Yi, Zhou Enlai, Pak Seong-cheol, and Ri Ju-yeon have a detailed conversation about the situations in Indonesia, Algeria, Uganda, Mali, Guinea, and members of the Third World. Credits: This document was made possible with support from the Henry Luce Foundation. Original Language: Chinese Contents: English Translation Foreign Ministry Top Secret Archives Record of Second Conversation of Premier Zhou Enlai and Vice Premier Chen Yi with Vice Premier Ri Ju-yeon [Ri Ju-yon] (Premier, Vice Premier have not yet examined and approved) Time: 8:30 a.m. To 1:30 p.m., 11 November 1965 Location: Conference Room, Villa 4, Diaoyutai State Guest House Participants: Chinese side: Li Xiannian, Fang Yi, Zhang Hanfu, Qiao Guanhua, Li Qiang, Hao Deqing, Jiao Ruoyu, Liu Xianglun Korean side: Pak Seong-cheol (Pak Song-chol), Pak Se-chang Interpreters: Chinese side: Jiang Chunyi Korean side: Kim Sun-ho Recorders: Chinese side. Tao Bingwei, He Zhangming Korean side: Go Sang-gyun [Ko Sang-gyun], Baek Hyeong-bu [Paek Hyong-bu] Vice Premier Chen Yi (hereafter, “Chen”): I will first discuss our relations with Asian and African countries and the situation in Asia and Africa. -

July 11, 1961 Minutes of Conversation Between Zhou Enlai and Kim Il Sung
Digital Archive digitalarchive.wilsoncenter.org International History Declassified July 11, 1961 Minutes of Conversation between Zhou Enlai and Kim Il Sung Citation: “Minutes of Conversation between Zhou Enlai and Kim Il Sung,” July 11, 1961, History and Public Policy Program Digital Archive, PRC FMA 204-01454-01, 1-12. Translated by Jeffrey Wang and Charles Kraus. http://digitalarchive.wilsoncenter.org/document/114178 Summary: Zhou Enlai and Kim Il Sung discuss economic cooperation between China and North Korea, including industrial development in North Korea, Chinese economic support to North Korea, bilateral trade, Chinese training of North Korean technicians, agricultural development in North Korea, cross-border migration, and development strategies in the DPRK. Credits: This document was made possible with support from the MacArthur Foundation and the Leon Levy Foundation. Original Language: Chinese Contents: English Translation (Not yet proof read) Time: 11 July 1961, 11:40 a.m.– 1:20 p.m. Location: 18th floor reception room, Diaoyutai Accompanying the visit [on the Chinese side] are: Members of the Political Bureau of the CPC Central Committee Chen Yi and Li Fuchun, State Council Vice Premier Luo Ruiqing, Foreign Trade Minister Ye Jizhuang, State Planning Commission Deputy Director Fang Yi, Vice Foreign Minister Ji Pengfei, and [Chinese] Ambassador to [North] Korea Qiao Xiaoguang. Seated on the Korean side are: Korean Workers’ Party Central Committee Vice Chairman Kim Chang-man [Kim Chang Man], Korean Workers’ Party Central Committee Standing Committee Member, Vice Premier, and Minister for the Protection of the Nation Kim Gwang-hyeop [Kim Kwang Hyop], Korean Workers’ Party Central Committee Standing Committee Alternate Member, Vice Premier, and Chairman of the Heavy Industry Committee Ri Jeong-ok [Ri Jeong-ok], Foreign Minister Pak Seong-cheol [Pak Song Chol], and charge d’affaires of [North] Korean Embassy in China Ma Dong-san [Ma Tong San]. -

The Communist Party of China: I • Party Powers and Group Poutics I from the Third Plenum to the Twelfth Party Congress
\ 1 ' NUMBER 2- 1984 (81) NUMBER 2 - 1984 (81) THE COMMUNIST PARTY OF CHINA: I • PARTY POWERS AND GROUP POUTICS I FROM THE THIRD PLENUM TO THE TWELFTH PARTY CONGRESS Hung-mao Tien School of LAw ~ of MAaylANCI • ' Occasional Papers/Reprint Series in Contemporary Asian Studies General Editor: Hungdah Chiu Executive Editor: Mitchell A. Silk Managing Editor: Shirley Lay Editorial Advisory Board Professor Robert A. Scalapino, University of California at Berkeley Professor Martin Wilbur, Columbia University Professor Gaston J. Sigur, George Washington University Professor Shao-chuan Leng, University of Virginia Professor Lawrence W. Beer, Lafayette College Professor James Hsiung, New York University Dr. Lih-wu Han, Political Science Association of the Republic of China Professor J. S. Prybyla, The Pennsylvania State University Professor Toshio Sawada, Sophia University, Japan Professor Gottfried-Karl Kindermann, Center for International Politics, University of Munich, Federal Republic of Germany Professor Choon-ho Park, College of Law and East Asian Law of the Sea Institute, Korea University, Republic of Korea Published with the cooperation of the Maryland International Law Society All contributions (in English only) and communications should be sent to Professor Hungdah Chiu, University of Maryland School of Law, 500 West Baltimore Street, Baltimore, Maryland 21201 USA. All publications in this series reflect only the views of the authors. While the editor accepts responsibility for the selection of materials to be published, the individual author is responsible for statements of facts and expressions of opinion contained therein. Subscription is US $10.00 for 6 issues (regardless of the price of individual issues) in the United States and Canada and $12.00 for overseas. -
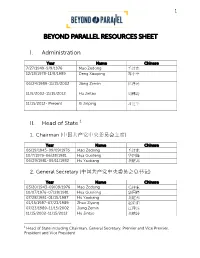
Beyond Parallel Resources Sheet
1 BEYOND PARALLEL RESOURCES SHEET I. Administration Year Name Chinese 7/27/1949-9/9/1976 Mao Zedong 毛泽东 12/18/1978-11/8/1989 Deng Xiaoping 邓小平 06/24/1989-11/15/2002 Jiang Zemin 江泽民 11/5/2002-11/15/2012 Hu Jintao 胡锦涛 11/15/2012- Present Xi Jinping 习近平 II. Head of State 1 1. Chairman (中国共产党中央委员会主席) Year Name Chinese 06/19/1945-09/09/1976 Mao Zedong 毛泽东 10/7/1976-06/28/1981 Hua Guofeng 华国锋 06/29/1981-09/11/1982 Hu Yaobang 胡耀邦 2. General Secretary (中国共产党中央委员会总书记) Year Name Chinese 03/20/1943-09/09/1976 Mao Zedong 毛泽东 10/07/1976-07/28/1981 Hua Guofeng 华国锋 07/28/1981-01/15/1987 Hu Yaobang 胡耀邦 01/15/1987-07/23/1989 Zhao Ziyang 赵紫阳 07/23/1989-11/15/2002 Jiang Zemin 江泽民 11/15/2002-11/15/2012 Hu Jintao 胡锦涛 1 Head of State including Chairman, General Secretary, Premier and Vice Premier, President and Vice President 2 11/15/2012-Present Xi Jinping 习近平 3. Premier (中华人民共和国国务院总理) Year Name Chinese 10/1949-01/1976 Zhou Enlai 周恩来 2/2/1976-09/10/1980 Hua Guofeng 华国锋 09/10/1980-11/24/1987 Zhao Ziyang 赵紫阳 11/24/1987-03/17/1998 Li Peng 李鹏 03/17/1998-03/16/2003 Zhu Rongji 朱镕基 03/16/2003-03/15/2013 Wen Jiabao 温家宝 03/15/2013-Present Li Keqiang 李克强 4. Vice Premier (中华人民共和国国务院副总理) Year Name Chinese 09/15/1954-12/21/1964 Chen Yun 陈云 12/21/1964-09/13/1971 Lin Biao 林彪 09/13/1971-09/10/1980 Deng Xiaoping 邓小平 09/10/1980-03/25/1988 Wan Li 万里 03/25/1988-3/05/1993 Yao Yilin 姚依林 3/25/1993-03/17/1998 Zhu Rongji 朱镕基 03/17/1998-03/06/2003 Li Lanqing 李岚清 03/06/2003-06/02/2007 Huang Ju 黄菊 06/02/2007-03/16/2008 Wu Yi 吴仪 03/16/2008-03/16/2013 Li Keqiang 李克强 03/16/2013-Present Zhang Gaoli 张高丽 5. -

A Physicist's View of Science and Technology in China 1
C. K. JEN A PHYSICIST'S VIEW OF SCIENCE AND TECHNOLOGY IN CHINA 1 A Chinese-born scientist reviews the Science Policy for Modernization in China, as formulated by the Chinese leadership in 1978, its initial results, and some future prospects. He uses information derived from his long-time personal experiences and many on-the-spot observations; discussions with his Chinese friends, former colleagues, and students; and professional opinions on China's Modernization expressed by visiting foreign experts. PROLOGUE: A SHORT ACCOUNT OF science and technology, principally because of the CHINA'S CONNECTION WITH SCIENCE disruptions caused first by the tumultuous civil strife among the Chinese warlords and later the prolonged AND TECHNOLOGY Sino-J apanese War. Ancient and medieval China are universally After the Chinese communists succeeded in their credited with the invention of the abacus, the mag revolution in 1949, the Russians sent a large number netic compass, gunpowder, papermaking, printing, of technical experts to help China's reconstruction and mechanical clocks, and with early observations and exerted great influence in all areas of Chinese so of astronomical phenomena and earthquakes. How ciety, including science and technology. China sent to ever, for more than 300 years, China's place in the Soviet Union a number of scholars to do research science and technology had fallen into a dismal and a sizable number of students to pursue scientific abyss, while the Western world reached great heights and technological studies. Upon their return, many in these fields through the Renaissance and the of these scholars became leaders in their own fields in periods of Scientific and Industrial Revolution. -

From the Conference Chair
2008 International Conference on Computer Science and Software Engineering (CSSE 2008) Wuhan, China 12 – 14 December 2008 Volume 1 Pages 1-621 IEEE Catalog Number: CFP08CSA-PRT ISBN: 978-1-4244-3902-7 TABLE OF CONTENTS ARTIFICIAL INTELLIGENCE HMM-Based-Correlations in Infrared Remote-Image ....................................................................................1 Rui Yang, Bo Li A Fuzzy Interactive Approach for Decentralized Bilevel Programming Problem with a Common Decision Variable................................................................................................................................5 Guangmin Wang, Zhongping Wan The Research about Integration of Process Planning and Production Scheduling Based on Genetic Algorithm...............................................................................................................................................9 Wang Zhanjie, Tian Ju Water Quality Assessment Using Artificial Neural Network........................................................................13 Ma Huiqun, Liu Ling A Hybrid Multi-user Receiver Based on Parallel Interference Cancellation and Improved Genetic Algorithm.............................................................................................................................................16 Lili Lin Query-Focused Multi-document Summarization Using Keyword Extraction ............................................20 Liang Ma, Tingting He, Fang Li, Zhuomin Gui, Jinguang Chen Weak Biosignal Processing Using Adaptive Wavelet Neural