VFR Flight Into Dark Night Conditions and Loss of Control Involving Piper PA-28-180, VH-POJ
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Airport City Developments in Australia : Land Use Classification and Analyses
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Queensland University of Technology ePrints Archive QUT Digital Repository: http://eprints.qut.edu.au/ Walker, Arron R. and Stevens, Nicholas J. (2008) Airport city developments in Australia : land use classification and analyses. In: 10th TRAIL Congress and Knowledge Market, 14-15 October 2008, Rotterdam, The Netherlands. © Copyright 2008 [please consult the authors] Airport city developments in Australia Land use classification and analyses TRAIL Research School, Delft, October 2008 Authors Dr. Arron Walker, Dr. Nicholas Stevens Faculty of Built Environment and Engineering, School of Urban Development, Queensland University of Technology, Qld, Australia © 2008 by A. Walker, N. Stevens and TRAIL Research School Contents Abstract 1 Introduction.......................................................................................................1 2 Background........................................................................................................2 2.1 Aviation growth in Australia...............................................................................2 2.2 Airport ownership in Australia ...........................................................................3 2.3 Airport Planning under Airports Act 1996 .........................................................4 2.4 Diversification of airport revenue.......................................................................5 3 Land use analysis: methods and materials .....................................................5 -

MINUTES AAA VIC Division Meeting
MINUTES AAA VIC Division Meeting Wednesday 7 August 2019 08:30 – 15:30 Holiday Inn Melbourne Airport Grand Centre Room, 10-14 Centre Road, Melbourne Airport Chair: Katie Cooper Attendees & Apologies: Please see attached 1. Introduction from Victorian Chair, Apologies, Minutes and Chair’s Report (Katie Cooper) • Introduced Daniel Gall, Deputy Chair for Vic Division • Provided overview of speakers for the day. • Dinner held previous evening which was a great way to meet and network – feedback welcome on if it is something you would like to see as an ongoing event Chairman’s Report Overview – • Board and Stakeholder dinner in Canberra with various industry and political leader and influences in attendance • AAA represented at the ACI Asia Pacific Conference and World AGM in Hong Kong • AAA Pavement & Lighting Forum held in Melbourne CBD with excellent attendance and positive feedback on its value to the industry • June Board Meeting in Brisbane coinciding with Qld Div meeting and dinner • Announcement of Federal Government $100M for regional airports • For International Airports, the current revisions of the Port Operators Guide for new and redeveloping ports which puts a lot of their costs onto industry is gaining focus from those affected industry members • MOS 139 changes update • Airport Safety Week in October • National Conference in November on the Gold Coast incl Women in Airports Forum • Launch of the new Corporate Member Advisory Panel (CMAP) which will bring together a panel of corporate members to gain feedback on issues impacting the AAA and wider airport sector and chaired by the AAA Chairman Thanks to Smiths Detection as the Premium Division Meetings Partner 2. -

1. Gina Rinehart 2. Anthony Pratt & Family • 3. Harry Triguboff
1. Gina Rinehart $14.02billion from Resources Chairman – Hancock Prospecting Residence: Perth Wealth last year: $20.01b Rank last year: 1 A plunging iron ore price has made a big dent in Gina Rinehart’s wealth. But so vast are her mining assets that Rinehart, chairman of Hancock Prospecting, maintains her position as Australia’s richest person in 2015. Work is continuing on her $10billion Roy Hill project in Western Australia, although it has been hit by doubts over its short-term viability given falling commodity prices and safety issues. Rinehart is pressing ahead and expects the first shipment late in 2015. Most of her wealth comes from huge royalty cheques from Rio Tinto, which mines vast swaths of tenements pegged by Rinehart’s late father, Lang Hancock, in the 1950s and 1960s. Rinehart's wealth has been subject to a long running family dispute with a court ruling in May that eldest daughter Bianca should become head of the $5b family trust. 2. Anthony Pratt & Family $10.76billion from manufacturing and investment Executive Chairman – Visy Residence: Melbourne Wealth last year: $7.6billion Rank last year: 2 Anthony Pratt’s bet on a recovering United States economy is paying off. The value of his US-based Pratt Industries has surged this year thanks to an improving manufacturing sector and a lower Australian dollar. Pratt is also executive chairman of box maker and recycling business Visy, based in Melbourne. Visy is Australia’s largest private company by revenue and the biggest Australian-owned employer in the US. Pratt inherited the Visy leadership from his late father Richard in 2009, though the firm’s ownership is shared with sisters Heloise Waislitz and Fiona Geminder. -

Loss of Control, Clyde North, Vic., 23 February 2007, Van's Aircraft Inc
ATSB TRANSPORT SAFETY INVESTIGATION REPORT Aviation Occurrence Investigation – 200701033 Final Loss of Control Clyde North, Victoria 23 February 2007 Van’s Aircraft Inc. RV-4, VH-ZGH ATSB TRANSPORT SAFETY INVESTIGATION REPORT Aviation Occurrence Investigation 200701033 Final Loss of Control Clyde North, Victoria 23 February 2007 Van’s Aircraft Inc. RV-4, VH-ZGH Released in accordance with section 25 of the Transport Safety Investigation Act 2003 - i - Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office location: 15 Mort Street, Canberra City, Australian Capital Territory Telephone: 1800 621 372; from overseas + 61 2 6274 6440 Accident and incident notification: 1800 011 034 (24 hours) Facsimile: 02 6247 3117; from overseas + 61 2 6247 3117 E-mail: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2008. This work is copyright. In the interests of enhancing the value of the information contained in this publication you may copy, download, display, print, reproduce and distribute this material in unaltered form (retaining this notice). However, copyright in the material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you want to use their material you will need to contact them directly. Subject to the provisions of the Copyright Act 1968, you must not make any other use of the material in this publication unless you have the permission of the Australian Transport Safety Bureau. Please direct requests for further information or authorisation to: Commonwealth Copyright Administration, Copyright Law Branch Attorney-General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 www.ag.gov.au/cca ISBN and formal report title: see ‘Document retrieval information’ on page iii. -
Experience Won't Always Save
Avoidable Accidents No. 6 Experience won’t always save you Pilot experience is not always a protection against an accident Research AR-2012-035 Publication title Avoidable Accidents No. 6 Experience won’t always save you: Pilot experience is not always a protection against an accident Report No. AR-2012-035 Publication date March 2013 ISBN 978-1-74251-291-4 Publishing information Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office: 62 Northbourne Avenue Canberra, Australian Capital Territory 2601 Telephone: 1800 020 616, from overseas +61 2 6257 4150 (24 hours) Accident and incident notification: 1800 011 034 (24 hours) Facsimile: 02 6247 3117, from overseas +61 2 6247 3117 Email: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2013 Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this publication is owned by the Commonwealth of Australia (referred to below as the Commonwealth). Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form license agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. -

Aviation Short Investigation Bulletin
InsertAviation document Short Investigations title Bulletin LocationIssue 36 | Date ATSB Transport Safety Report Investigation [InsertAviation Mode] Short OccurrenceInvestigations Investigation XX-YYYY-####AB-2014-158 Final – 3 December 2014 Released in accordance with section 25 of the Transport Safety Investigation Act 2003 Publishing information Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office: 62 Northbourne Avenue Canberra, Australian Capital Territory 2601 Telephone: 1800 020 616, from overseas +61 2 6257 4150 (24 hours) Accident and incident notification: 1800 011 034 (24 hours) Facsimile: 02 6247 3117, from overseas +61 2 6247 3117 Email: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2014 Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form license agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you want to use their material you will need to contact them directly. -
Essendon Fields Precinct – Hyatt Place Melbourne
insert cover positional here MELBOURNE CBD about this 15 minutes box size 10% Transparency of your 16 DFO ESSENDON cover artwork Tullamarine Freeway & CityLink TRA N S P O R T A BOUT U S 15 iFLY THINGS TO D O F OOD & DRINK 6 ESSENDON FIELDS AIRPORT 7 GYMNASIUM S ERVICE S 9 ESSENDON FIELDS CENTRAL 12 LAMANNA CAFÉ & SUPERMARKET ue ven 1 THE HUNGRY FOX CAFÉ ve A Hargra Bristol Street 2 CAR DEALERSHIPS MELBOURNE AIRPORT 3 FLIGHT EXPERIENCES 8 CHILDCARE 11 DENTIST 7km* 4 AIRWAYS MUSEUM 13 HYATT PLACE HOTEL & EVENTS CENTRE CYCLING TRAIL 5 BOUNCE INC. TRAM STOP 56 10 MEDICAL CENTRE English Street ESSENDON STATION oad Nomad R levard kin Bou Lar ESSENDON FIELDS IS WELL CONNECTED TO BOTH THE BUSINESS DISTRICT MELBOURNE CBD AND 14 MR MCCRACKEN RESTAURANT & BAR MELBOURNE AIRPORT MELBOURNE CBD 10km* Public Transport The free EF Station Shuttle operates from Essendon Fields to Essendon Train Station. Every weekday departing on the half hour between 7.15 – 9.30am & 4.15 – 6.30pm. Tram service 59 is a short walk from EF. Stop 56 (Airport West), located on Matthews Ave/ Earl Street departs every 8 minutes. Myki available from EF Newsagency. Airport Transit 16 DFO Essendon The free airport shuttle bus operates on- DFO Essendon comprises over 110 outlet retailers including demand daily between Essendon Fields Polo Ralph Lauren, Hugo Boss, Ted Baker and Coach. The Airport and Melbourne Airport between adjacent Homemaker Hub comprises over 20 stores. 6.00am and 10.00pm. Visit ef.com.au/ 100 Bulla Road, Essendon airportshuttle for booking details. -

TTF Rapid Buses, Road & Rail (Melbourne Airport)
RAPID BUSES, ROAD AND RAIL GROUND TRANSPORT SOLUTIONS TO MEET MELBOURNE AIRPORT’S PASSENGER GROWTH TO 2050 JULY 2013 Membership of Tourism & Transport Forum Tourism & Transport Forum (TTF) is a national, member-funded CEO forum, advocating the public policy interests of 200 leading corporations and institutions in the Australian tourism, transport, aviation and investment sectors For further information please contact: Justin Wastnage | Director, Aviation Policy | [email protected] Martin Gray | Policy Officer |[email protected] Contents EXECUTIVE SUMMARY ............................................................................................... 4 Ensuring transport choice for Melbourne Airport ................................................................ 4 SUMMARY OF RECOMMENDATIONS ....................................................................... 6 List of figures ........................................................................................................................................................... 6 MELBOURNE AIRPORT – THE NEXT 30 YEARS ............................................................ 7 Forecast demand .................................................................................................................... 7 ACCESSING MELBOURNE AIRPORT .......................................................................... 8 Internal airport transport ......................................................................................................... 8 Broader road network ............................................................................................................ -
Aerodromes and Ala Codes
CODE - ENCODED 17 JUN 2021 IND - GEN - 1 AERODROMES AND ALA CODES - ENCODED LOCATION STATE CODE LOCATION STATE CODE ABBIEGLASSIE QLD YABG/ALA ANGLESTONE QLD YAST/ALA ABC TV STUDIOS GORE HILL NSW YABC/HLS ANMATJERE/GEMTREE NT YGTC/ALA ABERDEEN QLD YABD/ALA CARAVAN PARK ABERFOYLE QLD YABF/ALA ANMATJERE/PINE HILL NT YPHS/ALA STATION ABINGDON DOWNS QLD YABI/ALA ANNA CREEK SA YANK/ALA ACACIA DOWNS NSW YACS/ALA ANNA PLAINS HS WA YAPA/ALA ADAMINABY NSW YADY/ALA ANNANDALE QLD YADE/ALA ADAMINABY MEDICAL NSW YXAM/HLS ANNINGIE NT YANN/ALA ADAVALE QLD YADA/ALA ANNITOWA NT YANW/ALA ADELAIDE SA YPAD/AD ANSWER DOWNS QLD YAND/ALA ADELAIDE INTL RACEWAY SA YAIW/HLS ANTHONY LAGOON NT YANL/ALA ADELAIDE OVAL SA YAOV/HLS ANTRIM QLD YANM/ALA ADELAIDE/PARAFIELD SA YPPF/AD APOLLO BAY VIC YAPO/ALA ADELE ISLAND WA YADL/ALA ARAMAC QLD YAMC/ALA ADELS GROVE QLD YALG/ALA ARAPUNYA NT YARP/ALA AGINCOURT NORTH QLD YAIN/HLS ARARAT VIC YARA/AD AGINCOURT SOUTH QLD YAIS/HLS ARARAT HOSPITAL VIC YXAR/HLS AGNES WATER QLD YAWT/ALA ARCADIA QLD YACI/ALA AGNEW QLD YAGN/ALA ARCHER RIVER QLD YARC/ALA AILERON NT YALR/ALA ARCKARINGA SA YAKG/ALA ALAMEIN SA YAMN/ALA ARCTURUS DOWNS HS QLD YATU/ALA ALBANY WA YABA/AD ARDGOUR NSW YADU/ALA ALBANY PARK NT YAPK/ALA ARDLETHAN NSW YARL/ALA ALBILBAH QLD YALH/ALA ARDMORE QLD YAOR/ALA ALBION DOWNS WA YABS/ALA ARDROSSAN HOSPITAL SA YXAN/HLS ALBURY NSW YMAY/AD AREYONGA NT YARN/ALA ALBURY HOSPITAL NSW YXAL/HLS ARGADARGADA NT YARD/ALA ALCOOTA STN NT YALC/ALA ARGYLE QLD YAGL/ALA ALDERLEY QLD YALY/ALA ARGYLE WA YARG/AD ALDERSYDE QLD YADR/ALA ARIZONA HS -
MINUTES AAA Victorian Division Meeting
MINUTES AAA Victorian Division Meeting Tuesday 22 March 2016 10:00-15:00 Flight Deck Bar & Grill, 37 First Avenue, Moorabbin Airport, VIC 1. Welcome and Apologies Paul Ferguson (Chair) opened the meeting and welcomed members, thanking them for their attendance. A lunchtime visit to the Australian National Aviation Museum was offered to all attending members as well as a site tour of Moorabbin Airport. Attendees and apologies are listed below. ATTENDEES Paul Ferguson (Chair) Moorabbin Airport Corporation Guy Thompson AAA (National Chairman) Jared Feehely AAA Matt Smale Air BP Bryan Fitzgerald Airport Surveys Pty Ltd Kent Quigley Airservices Australia Ken Keech Australian International Airshow Chris Stocks Avdata Australia Sharon Lee Avdata Australia Bron Wiseman Avdata Australia Jeremy King Avlite Systems Pty Ltd Roger Druce Bacchus Marsh Aerodrome Management Inc. Joseph Walsh Beca Darren Angelo CASA Ron Brownlees City of Kingston Phil McConnell Cloud Aviation Department of Economic Development, Jobs, Marianne Richards Transport and Resources (DEDJTR) Ross Ioakim Downer Rory Kennedy Essendon Airport Graeme Ware Essendon Airport Daniel Taylor Fulton Hogan Nick Hrysomallis Fulton Hogan David Spencer Gannawarra Shire Brian Roberts Gannawarra Shire Ian Bell Global Safety Partners Trent Kneebush Kneebush Planning Garry Baum Lethbridge Airport MINUTES | AAA Victorian Division Meeting | Tuesday 22 March 2016 Tim Marks Marshall Day Acoustics Christophe Delaire Marshall Day Acoustics Justin Adcock Marshall Day Acoustics Melanie Hearne Melbourne -
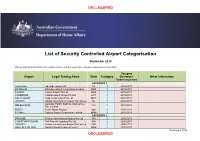
Airport Categorisation List
UNCLASSIFIED List of Security Controlled Airport Categorisation September 2018 *Please note that this table will continue to be updated upon new category approvals and gazettal Category Airport Legal Trading Name State Category Operations Other Information Commencement CATEGORY 1 ADELAIDE Adelaide Airport Ltd SA 1 22/12/2011 BRISBANE Brisbane Airport Corporation Limited QLD 1 22/12/2011 CAIRNS Cairns Airport Pty Ltd QLD 1 22/12/2011 CANBERRA Capital Airport Group Pty Ltd ACT 1 22/12/2011 GOLD COAST Gold Coast Airport Pty Ltd QLD 1 22/12/2011 DARWIN Darwin International Airport Pty Limited NT 1 22/12/2011 Australia Pacific Airports (Melbourne) MELBOURNE VIC 1 22/12/2011 Pty. Limited PERTH Perth Airport Pty Ltd WA 1 22/12/2011 SYDNEY Sydney Airport Corporation Limited NSW 1 22/12/2011 CATEGORY 2 BROOME Broome International Airport Pty Ltd WA 2 22/12/2011 CHRISTMAS ISLAND Toll Remote Logistics Pty Ltd WA 2 22/12/2011 HOBART Hobart International Airport Pty Limited TAS 2 29/02/2012 NORFOLK ISLAND Norfolk Island Regional Council NSW 2 22/12/2011 September 2018 UNCLASSIFIED UNCLASSIFIED PORT HEDLAND PHIA Operating Company Pty Ltd WA 2 22/12/2011 SUNSHINE COAST Sunshine Coast Airport Pty Ltd QLD 2 29/06/2012 TOWNSVILLE AIRPORT Townsville Airport Pty Ltd QLD 2 19/12/2014 CATEGORY 3 ALBURY Albury City Council NSW 3 22/12/2011 ALICE SPRINGS Alice Springs Airport Pty Limited NT 3 11/01/2012 AVALON Avalon Airport Australia Pty Ltd VIC 3 22/12/2011 Voyages Indigenous Tourism Australia NT 3 22/12/2011 AYERS ROCK Pty Ltd BALLINA Ballina Shire Council NSW 3 22/12/2011 BRISBANE WEST Brisbane West Wellcamp Airport Pty QLD 3 17/11/2014 WELLCAMP Ltd BUNDABERG Bundaberg Regional Council QLD 3 18/01/2012 CLONCURRY Cloncurry Shire Council QLD 3 29/02/2012 COCOS ISLAND Toll Remote Logistics Pty Ltd WA 3 22/12/2011 COFFS HARBOUR Coffs Harbour City Council NSW 3 22/12/2011 DEVONPORT Tasmanian Ports Corporation Pty. -

St Helens Aerodrome Assess Report
MCa Airstrip Feasibility Study Break O’ Day Council Municipal Management Plan December 2013 Part A Technical Planning & Facility Upgrade Reference: 233492-001 Project: St Helens Aerodrome Prepared for: Break Technical Planning and Facility Upgrade O’Day Council Report Revision: 1 16 December 2013 Document Control Record Document prepared by: Aurecon Australia Pty Ltd ABN 54 005 139 873 Aurecon Centre Level 8, 850 Collins Street Docklands VIC 3008 PO Box 23061 Docklands VIC 8012 Australia T +61 3 9975 3333 F +61 3 9975 3444 E [email protected] W aurecongroup.com A person using Aurecon documents or data accepts the risk of: a) Using the documents or data in electronic form without requesting and checking them for accuracy against the original hard copy version. b) Using the documents or data for any purpose not agreed to in writing by Aurecon. Report Title Technical Planning and Facility Upgrade Report Document ID 233492-001 Project Number 233492-001 File St Helens Aerodrome Concept Planning and Facility Upgrade Repot Rev File Path 0.docx Client Break O’Day Council Client Contact Rev Date Revision Details/Status Prepared by Author Verifier Approver 0 05 April 2013 Draft S.Oakley S.Oakley M.Glenn M. Glenn 1 16 December 2013 Final S.Oakley S.Oakley M.Glenn M. Glenn Current Revision 1 Approval Author Signature SRO Approver Signature MDG Name S.Oakley Name M. Glenn Technical Director - Title Senior Airport Engineer Title Airports Project 233492-001 | File St Helens Aerodrome Concept Planning and Facility Upgrade Repot Rev 1.docx |