Association of Helicobacter Pylori with Gastroduodenal Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Food Or Beverage Product, Or Probiotic Composition, Comprising Lactobacillus Johnsonii 456
(19) TZZ¥¥¥ _T (11) EP 3 536 328 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 11.09.2019 Bulletin 2019/37 A61K 35/74 (2015.01) A61K 35/66 (2015.01) A61P 35/00 (2006.01) (21) Application number: 19165418.5 (22) Date of filing: 19.02.2014 (84) Designated Contracting States: • SCHIESTL, Robert, H. AL AT BE BG CH CY CZ DE DK EE ES FI FR GB Encino, CA California 91436 (US) GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO • RELIENE, Ramune PL PT RO RS SE SI SK SM TR Los Angeles, CA California 90024 (US) • BORNEMAN, James (30) Priority: 22.02.2013 US 201361956186 P Riverside, CA California 92506 (US) 26.11.2013 US 201361909242 P • PRESLEY, Laura, L. Santa Maria, CA California 93458 (US) (62) Document number(s) of the earlier application(s) in • BRAUN, Jonathan accordance with Art. 76 EPC: Tarzana, CA California 91356 (US) 14753847.4 / 2 958 575 (74) Representative: Müller-Boré & Partner (71) Applicant: The Regents of the University of Patentanwälte PartG mbB California Friedenheimer Brücke 21 Oakland, CA 94607 (US) 80639 München (DE) (72) Inventors: Remarks: • YAMAMOTO, Mitsuko, L. This application was filed on 27-03-2019 as a Alameda, CA California 94502 (US) divisional application to the application mentioned under INID code 62. (54) FOOD OR BEVERAGE PRODUCT, OR PROBIOTIC COMPOSITION, COMPRISING LACTOBACILLUS JOHNSONII 456 (57) The present invention relates to food products, beverage products and probiotic compositions comprising Lacto- bacillus johnsonii 456. EP 3 536 328 A1 Printed by Jouve, 75001 PARIS (FR) EP 3 536 328 A1 Description CROSS-REFERENCE TO RELATED APPLICATIONS 5 [0001] This application claims the benefit of U.S. -

Kongre Kitabı
Book of Abstracts International VETistanbul Group Congress 2014 28-30 April, 2014 Istanbul, Turkey Book of Abstracts www.vetistanbul2014.org International VETistanbul Group Congress 2014 28-30 April 2014 International VETistanbul Group Congress 2014 28-30 April, 2014 Istanbul, Turkey Organizing Committee Prof. Dr. Halil GÜNEŞ, Chair Prof. Dr. Bülent EKİZ Prof. Dr. Ali AYDIN Assoc. Prof. Dr. Serkan İKİZ Assoc. Prof. Dr. Hasret DEMİRCAN YARDİBİ Assoc. Prof. Dr. Gülsün PAZVANT Scientific Committee* Prof. Dr. Kemal AK, Turkey Prof. Dr. Anatoliy ALEXANDROVICH STEKOLNIKOV, Russia Prof. Dr. Bogdan AMINKOV, Bulgaria Prof. Dr. Geno ATASANOV ANGELOV, Bulgaria Prof. Dr. Hajrudin BESIROVIC, Bosnia and Herzegovina Prof. Dr. Nihad FEJZIC, Bosnia and Herzegovina Assoc. Prof. Dr. Plamen GEORGIEV, Bulgaria Prof. Dr. Zehra HAJRULAI MUSLIU, Macedonia Assoc. Prof. Dr. Afrim HAMIDI, Kosovo Prof. Dr. Telman ISKENDEROV, Azerbaijan Prof. Dr. Larisa KARPENKO, Russia Prof. Dr. Ismail KIRSAN, Turkey Prof. Dr. Mihni LYUTSKANOV, Bulgaria Assoc. Prof. Dr. Avni ROBAJ, Kosovo Prof. Dr. Velimir STOJKOVSKI, Macedonia Prof. Dr. Semsir VELIYEV, Azerbaijan *Alphabetically listed by the according to the family name Scientific Secreteria Prof. Dr. Bülent EKİZ, Turkey Dr. Karlo MURATOĞLU, Turkey International VETistanbul Group Congress 2014, 28-30 April, Istanbul, Turkey IV International VETistanbul Group Congress 2014 28-30 April 2014 Dear Respectable Colleagues and Guests, First of all, I greet you all with my heart. Also, I would like to thank you for taking place on our side due to the contribution given to the establishment of VETistanbul Group. Known as, VETistanbul Group was established, under the coordination of Istanbul University, with joint decision of Veterinary Faculty of the University of Sarajevo, Saint Petersburg State Academy of Veterinary Medicine, Stara Zagora Trakia University, Ss. -

Review: Other Helicobacter Species
DOI: 10.1111/hel.12645 SUPPLEMENT ARTICLE Review: Other Helicobacter species Armelle Ménard1 | Annemieke Smet2 1INSERM, UMR1053, Bordeaux Research in Translational Oncology, BaRITOn, Université Abstract de Bordeaux, Bordeaux, France This article is a review of the most important, accessible, and relevant literature pub‐ 2 Laboratorium of Experimental lished between April 2018 and April 2019 in the field of Helicobacter species other than Medicine and Pediatrics, Department of Translational Research in Immunology and Helicobacter pylori. The initial part of the review covers new insights regarding the pres‐ Inflammation, Faculty of Medicine and ence of gastric and enterohepatic non‐H. pylori Helicobacter species (NHPH) in humans Health Sciences, University of Antwerp, Wilrijk (Antwerp), Belgium and animals, while the subsequent section focuses on the progress in our understand‐ ing of the pathogenicity and evolution of these species. Over the last year, relatively Correspondence Armelle Ménard, Laboratoire de few cases of gastric NHPH infections in humans were published, with most NHPH in‐ Bactériologie, INSERM U1053, Campus de fections being attributed to enterohepatic Helicobacters. A novel species, designated Carreire, Université de Bordeaux, Bâtiment 2B RDC ‐ Case 76, 146 rue Léo Saignat, “Helicobacter caesarodunensis,” was isolated from the blood of a febrile patient and F33076 Bordeaux, France. numerous cases of human Helicobacter cinaedi infections underlined this species as a Email: Armelle.Menard@u‐bordeaux.fr true emerging pathogen. With regard to NHPH in animals, canine/feline gastric NHPH cause little or no harm in their natural host; however they can become opportunistic when translocated to the hepatobiliary tract. The role of enterohepatic Helicobacter species in colorectal tumors in pets has also been highlighted. -

Table of Contents
MARCH 2013 • VOLUME 51 • NO. 3 TABLE OF CONTENTS PHOTO QUIZ Bacteremia in a Patient with Hepatic Encephalopathy Benjamin H. Hinrichs, Robert C. Jerris, 739 Eileen M. Burd Answer to Photo Quiz Benjamin H. Hinrichs, Robert C. Jerris, 1062–1063 Eileen M. Burd POINT-COUNTERPOINT Quantitative Cultures of Bronchoscopically Obtained Vickie Baselski, J. Stacey Klutts 740–744 Specimens Should Be Performed for Optimal Management of Ventilator-Associated Pneumonia BACTERIOLOGY Pan-PCR, a Computational Method for Designing Bacterium- Joy Y. Yang, Shelise Brooks, Jennifer A. 752–758 Typing Assays Based on Whole-Genome Sequence Data Meyer, Robert R. Blakesley, Adrian M. Zelazny, Julia A. Segre, Evan S. Snitkin Identification of Anaerobic Bacteria by Bruker Biotyper Matrix- Bryan H. Schmitt, Scott A. 782–786 Assisted Laser Desorption Ionization–Time of Flight Mass Cunningham, Aaron L. Dailey, Spectrometry with On-Plate Formic Acid Preparation Daniel R. Gustafson, Robin Patel Use of Universal 16S rRNA Gene PCR as a Diagnostic Tool for M. Guembe, M. Marín, P. Martín- 799–804 Venous Access Port-Related Bloodstream Infections Rabadán, A. Echenagusia, F. Camúñez, G. Rodríguez-Rosales, G. Simó, M. Echenagusia, E. Bouza, on behalf of the GEIDI Study Group Rapid Identification of Bacteria and Yeasts from Positive-Blood- Amy Fothergill, Vyjayanti Kasinathan, 805–809 Culture Bottles by Using a Lysis-Filtration Method and Matrix- Jay Hyman, John Walsh, Tim Drake, Assisted Laser Desorption Ionization–Time of Flight Mass Yun F. (Wayne) Wang Spectrum Analysis with the SARAMIS Database Pseudo-Outbreak of Vancomycin-Resistant-Enterococcus Rita M. Gander, Dominick Cavuoti, 810–813 (VRE) Colonization in a Neonatal Intensive Care Unit Using Adnan Alatoom, Paul Southern, Jr., Spectra VRE Surveillance Medium Debra Grant, Kathleen Salinas, Donna Gaffney, Jennifer MacKenzie, Linda Byrd Changes in Molecular Epidemiology of Streptococcus Bruno Pichon, Shamez N. -
C O N F E R E N C E 22 27 April 2016
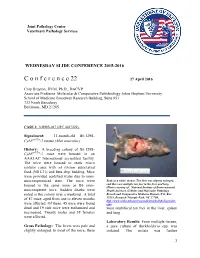
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Genomics of Helicobacter Species 91
Genomics of Helicobacter Species 91 6 Genomics of Helicobacter Species Zhongming Ge and David B. Schauer Summary Helicobacter pylori was the first bacterial species to have the genome of two independent strains completely sequenced. Infection with this pathogen, which may be the most frequent bacterial infec- tion of humanity, causes peptic ulcer disease and gastric cancer. Other Helicobacter species are emerging as causes of infection, inflammation, and cancer in the intestine, liver, and biliary tract, although the true prevalence of these enterohepatic Helicobacter species in humans is not yet known. The murine pathogen Helicobacter hepaticus was the first enterohepatic Helicobacter species to have its genome completely sequenced. Here, we consider functional genomics of the genus Helico- bacter, the comparative genomics of the genus Helicobacter, and the related genera Campylobacter and Wolinella. Key Words: Cytotoxin-associated gene; H-Proteobacteria; gastric cancer; genomic evolution; genomic island; hepatobiliary; peptic ulcer disease; type IV secretion system. 1. Introduction The genus Helicobacter belongs to the family Helicobacteriaceae, order Campylo- bacterales, and class H-Proteobacteria, which is also known as the H subdivision of the phylum Proteobacteria. The H-Proteobacteria comprise of a relatively small and recently recognized line of descent within this extremely large and phenotypically diverse phy- lum. Other genera that colonize and/or infect humans and animals include Campylobac- ter, Arcobacter, and Wolinella. These organisms are all microaerophilic, chemoorgano- trophic, nonsaccharolytic, spiral shaped or curved, and motile with a corkscrew-like motion by means of polar flagella. Increasingly, free living H-Proteobacteria are being recognized in a wide range of environmental niches, including seawater, marine sedi- ments, deep-sea hydrothermal vents, and even as symbionts of shrimp and tubeworms in these environments. -

Supplemental Material S1.Pdf
Phylogeny of Selenophosphate synthetases (SPS) Supplementary Material S1 ! SelD in prokaryotes! ! ! SelD gene finding in sequenced prokaryotes! We downloaded a total of 8263 prokaryotic genomes from NCBI (see Supplementary Material S7). We scanned them with the program selenoprofiles (Mariotti 2010, http:// big.crg.cat/services/selenoprofiles) using two SPS-family profiles, one prokaryotic (seld) and one mixed eukaryotic-prokaryotic (SPS). Selenoprofiles removes overlapping predictions from different profiles, keeping only the prediction from the profile that seems closer to the candidate sequence. As expected, the great majority of output predictions in prokaryotic genomes were from the seld profile. We will refer to the prokaryotic SPS/SelD !genes as SelD, following the most common nomenclature in literature.! To be able to inspect results by hand, and also to focus on good-quality genomes, we considered a reduced set of species. We took the prok_reference_genomes.txt list from ftp://ftp.ncbi.nlm.nih.gov/genomes/GENOME_REPORTS/, which NCBI claims to be a "small curated subset of really good and scientifically important prokaryotic genomes". We named this the prokaryotic reference set (223 species - see Supplementary Material S8). We manually curated most of the analysis in this set, while we kept automatized the !analysis on the full set.! We detected SelD proteins in 58 genomes (26.0%) in the prokaryotic reference set (figure 1 in main paper), which become 2805 (33.9%) when considering the prokaryotic full set (figure SM1.1). The difference in proportion between the two sets is due largely to the presence of genomes of very close strains in the full set, which we consider redundant. -

Co-Infection Associated with Diarrhea in a Colony of <I>Scid
Laboratory Animal Science Vol 48, No 5 Copyright 1998 October 1998 by the American Association for Laboratory Animal Science Helicobacter bilis/Helicobacter rodentium Co-Infection Associated with Diarrhea in a Colony of scid Mice Nirah H. Shomer,* Charles A. Dangler, Robert P. Marini, and James G. Fox† Abstract _ An outbreak of diarrhea spanning 3 months occurred in a breeding colony of scid/Trp53 knockout mice. Approximately a third of the 150 mice were clinically affected, with signs ranging from mucoid or watery diarrhea to severe hemorrhagic diarrhea with mortality. Helicobacter bilis and the newly recognized urease-negative organ- ism H. rodentium were isolated from microaerobic culture of feces or cecal specimens from affected mice. Dual infection with H. bilis and H. rodentium were confirmed by culture and polymerase chain reaction (PCR) in several animals. Both Helicobacter species rapidly colonized immunocompetent sentinel mice exposed to bedding from cages containing affected mice, but the sentinel remained asymptomatic. Mice with diarrhea had multifocal to segmental proliferative typhlitis, colitis, and proctitis. Several affected mice had multifocal mucosal necrosis with a few focal ulcers in the cecum, colon, and rectum. Mice with diarrhea were treated with antibiotic food wafers (1.5 mg of amoxicillin, 0.69 mg of metronidazole, and 0.185 mg of bismuth/mouse per day) previously shown to eradi- cate H. hepaticus in immunocompetent mice. Antibiotic treatment resulted in resolution of diarrhea, but not eradication of H. bilis and H. rodentium; mice continued to have positive PCR results after a 2-week treatment regimen, and clinical signs of diarrhea returned in some mice when treatment was suspended. -

Enterohepatic Lesions in SCID Mice Infected with Helicobacter Bilis
Laboratory Animal Science Vol 48, No 4 Copyright 1998 August 1998 by the American Association for Laboratory Animal Science Enterohepatic Lesions in SCID Mice Infected with Helicobacter bilis Craig L. Franklin, Lela K. Riley, Robert S. Livingston, Catherine S. Beckwith, Cynthia L. Besch-Williford, and Reuel R. Hook, Jr. Abstract _ Helicobacter bilis is a recently identified species that colonizes the intestine and liver of mice. In immunocompetent mice, infections have been associated with mild hepatitis, and in immunocompromised mice, inflammatory bowel disease has been induced by intraperitoneal inoculation of the organism. We re- port inoculation of 6-week-old C.B-17 scid/scid mice by gastric gavage with approximately 107 H. bilis colony- forming units. Groups of mice were euthanized and necropsied 12, 24, and 36 weeks after inoculation. Mild to moderate proliferative typhlitis was evident in all mice at 12 and 36 weeks after inoculation and in most mice 24 weeks after inoculation. Mild to severe chronic active hepatitis was detected in 10 of 10 male mice and 3 of 10 female mice. These results indicate that H. bilis can cause moderate to severe enterohepatic disease in immunocompromised mice. The genus Helicobacter is a rapidly expanding genus volved in lesion development. Culture of specimens from currently containing 17 named species. Members of this mice confirmed intestinal colonization with H. hepaticus. Fox genus are microaerophilic, have curved to spiral rod mor- et al. reported enteric lesions in immunocompetent germ- phology, and are motile by flagella that vary in number free Swiss Webster mice infected with H. hepaticus (15), and and location among various species (1). -

Biliary Tract Microbiota: a New Kid on the Block of Liver Diseases?
European Review for Medical and Pharmacological Sciences 2020; 24: 2750-2775 Biliary tract microbiota: a new kid on the block of liver diseases? A. NICOLETTI1, F.R. PONZIANI2, E. NARDELLA1, G. IANIRO2, A. GASBARRINI1, L. ZILERI DAL VERME2 1Internal Medicine, Gastroenterology and Hepatology, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy 2Internal Medicine, Gastroenterology and Hepatology, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy Abstract. – The microbiome plays a crucial man body1,2. Indeed, a resident microbiota has recent- role in maintaining the homeostasis of the or- ly been described in several human environments ganism. Recent evidence has provided novel previously described as devoid of microorganisms, insights for understanding the interaction be- such as the urinary tract and the stomach3-9. Even tween the microbiota and the host. However, the 10 vast majority of such studies have analyzed the healthy placenta hosts microbial communities . interactions taking place in the intestinal tract. Bile has traditionally been considered sterile The biliary tree has traditionally been consid- under normal conditions11-14. ered sterile under normal conditions. However, The physical and chemical features of bile and the advent of metagenomic techniques has re- its antimicrobial activity were supposed to create vealed an unexpectedly rich bacterial communi- a hostile environment for bacteria. Moreover, the ty in the biliary tract. Associations between specific microbiolog- difficulty in collecting bile samples, coupled with ical patterns and inflammatory biliary diseases the lack of sensibility of culture techniques in and cancer have been recently described. Hence, detecting microbes in low-charge samples, sus- biliary dysbiosis may be a primary trigger in the tained this hypothesis for a long time. -

Helicobacter Spp. — Food- Or Waterborne Pathogens?
FRI FOOD SAFETY REVIEWS Helicobacter spp. — Food- or Waterborne Pathogens? M. Ellin Doyle Food Research Institute University of Wisconsin–Madison Madison WI 53706 Contents34B Introduction....................................................................................................................................1 Virulence Factors ...........................................................................................................................2 Associated Diseases .......................................................................................................................2 Gastrointestinal Disease .........................................................................................................2 Neurological Disease..............................................................................................................3 Other Diseases........................................................................................................................4 Epidemiology.................................................................................................................................4 Prevalence..............................................................................................................................4 Transmission ..........................................................................................................................4 Summary .......................................................................................................................................5 -

Helicobacter Hepaticus Model of Infection: the Human Hepatocellular Carcinoma Controversy
Review articles Helicobacter hepaticus model of infection: the human hepatocellular carcinoma controversy Yessica Agudelo Zapata, MD,1 Rodrigo Castaño Llano, MD,2 Mauricio Corredor, PhD.3 1 Medical Doctor and General Surgeon in the Abstract Gastrohepatology Group at Universidad de Antioquia in Medellin, Colombia The discovery of Helicobacter 30 years ago by Marshall and Warren completely changed thought about peptic 2 Gastrointestinal Surgeon and Endoscopist in the and duodenal ulcers. The previous paradigm posited the impossibility of the survival of microorganisms in the Gastrohepatology Group at the Universidad de stomach’s low pH environment and that, if any microorganisms survived, they would stay in the duodenum Antioquia in Medellin, Colombia 3 Institute Professor of Biology in the Faculty of or elsewhere in the intestine. Today the role of H. pylori in carcinogenesis is indisputable, but little is known Natural Sciences and the GEBIOMIC Group the about other emerging species of the genus Helicobacter in humans. Helicobacter hepaticus is one of these Gastroenterology Group at the Universidad de species that has been studied most, after H. pylori. We now know about their microbiological, genetic and Antioquia in Medellin, Colombia pathogenic relationships with HCC in murine and human infections. This review aims to show the medical and ......................................... scientifi c community the existence of new species of Helicobacter that have pathogenic potential in humans, Received: 07-05-13 thus encouraging research. Accepted: 27-08-13 Keywords Helicobacter hepaticus, Helicobacter pylori, Helicobacter spp., hepatocellular carcinoma. INTRODUCTION bacterium can infect animals including mice, dogs and ger- bils which could lead to a proposal to use H.