Faecalibacterium Prausnitzii and Human Intestinal Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -

Altered Fecal Microbiota Composition in Patients with Major Depressive Disorder
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector Brain, Behavior, and Immunity 48 (2015) 186–194 Contents lists available at ScienceDirect Brain, Behavior, and Immunity journal homepage: www.elsevier.com/locate/ybrbi Altered fecal microbiota composition in patients with major depressive disorder Haiyin Jiang a,1, Zongxin Ling a,1, Yonghua Zhang b,1, Hongjin Mao c, Zhanping Ma d, Yan Yin c, ⇑ Weihong Wang e, Wenxin Tang c, Zhonglin Tan c, Jianfei Shi c, Lanjuan Li a,2, Bing Ruan a, a Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310003, China b Department of Traditional Chinese Medicine, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China c Department of Psychiatry, The Seventh People’s Hospital of Hangzhou, Hangzhou, Zhejiang 310003, China d Department of Psychiatry, Psychiatric Hospital of Hengshui, Hebei 053000, China e Department of Infectious Diseases, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China article info abstract Article history: Studies using animal models have shown that depression affects the stability of the microbiota, but the Received 29 July 2014 actual structure and composition in patients with major depressive disorder (MDD) are not well under- Received in revised form 29 March 2015 stood. Here, we analyzed fecal samples from 46 patients with depression (29 active-MDD and 17 Accepted 29 March 2015 responded-MDD) and 30 healthy controls (HCs). High-throughput pyrosequencing showed that, accord- Available online 13 April 2015 ing to the Shannon index, increased fecal bacterial a-diversity was found in the active-MDD (A-MDD) vs. -

Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis
International Journal of Molecular Sciences Review Fatty Acid Diets: Regulation of Gut Microbiota Composition and Obesity and Its Related Metabolic Dysbiosis David Johane Machate 1, Priscila Silva Figueiredo 2 , Gabriela Marcelino 2 , Rita de Cássia Avellaneda Guimarães 2,*, Priscila Aiko Hiane 2 , Danielle Bogo 2, Verônica Assalin Zorgetto Pinheiro 2, Lincoln Carlos Silva de Oliveira 3 and Arnildo Pott 1 1 Graduate Program in Biotechnology and Biodiversity in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] (D.J.M.); [email protected] (A.P.) 2 Graduate Program in Health and Development in the Central-West Region of Brazil, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; pri.fi[email protected] (P.S.F.); [email protected] (G.M.); [email protected] (P.A.H.); [email protected] (D.B.); [email protected] (V.A.Z.P.) 3 Chemistry Institute, Federal University of Mato Grosso do Sul, Campo Grande 79079-900, Brazil; [email protected] * Correspondence: [email protected]; Tel.: +55-67-3345-7416 Received: 9 March 2020; Accepted: 27 March 2020; Published: 8 June 2020 Abstract: Long-term high-fat dietary intake plays a crucial role in the composition of gut microbiota in animal models and human subjects, which affect directly short-chain fatty acid (SCFA) production and host health. This review aims to highlight the interplay of fatty acid (FA) intake and gut microbiota composition and its interaction with hosts in health promotion and obesity prevention and its related metabolic dysbiosis. -
MALDI-TOF MS for the Identification of Anaerobic Bacteria
University Medical Center Groningen Department Medical Microbiology and Infection Prevention Linda Veloo Expert Center Anaerobic Infections The Netherlands www.mmb-umcg.eu © by author ESCMID Online Lecture Library Matrix Assisted Laser Desorption/Ionization time-of-flight Mass Spectrometry (MALDI-TOF MS) Time of flight tube Target at 15-25 kV Detector Ion source © by author ESCMID- “Time of flight” Online of individual Lecture proteins is converted Library into mass information. - Spectrum is produced - Database is built Veloo et al. Anaerobe 2011; 17:211-212 Workflow Direct spotting of bacteria on target using a toothpick Add HCCA matrix Data acquisition © Databy analyses author ESCMID Online Lecture Library Log score: <1.7 no reliable identification 1.7 – 2.0 reliable genus identification ≥ 2.0 reliable species identification Obtained spectrum is unique for bacterial species Intensity © by author ESCMID Online Lecture Library Anaerobic culture Phenotypic pure culture primary incubation 2 days 2-7 days aerotolerance identification MALDI-TOF MS 1 day 2-14 days primary incubation 2-7 days © by author MALDI-TOF MS testing minutes ESCMID Online Lecture Library How many anaerobic bacteria can be identified using MALDI-TOF MS? UMCG 2011/2012 Total no. of strains 1000 Species ID 650 65% Genus ID 149 15% No ID © 201by author20% ESCMID Online Lecture Library Performance differs per genus Genus* % species ID % genus ID Clostridium sp. (n=149) 97 3 B. fragilis sp. (n=179) 97 3 Parabacteroides sp. (n=14) 93 7 GPAC (n=133) 85 15 Prevotella sp.(n=83) 78 12 Propionibacterium sp. (n=129) 64 36 Actinomyces sp. (n=28) 57 43 Fusobacterium sp. -
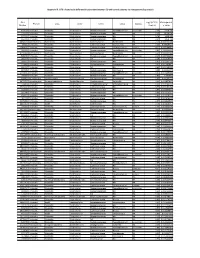
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Microbiota of Human Precolostrum and Its Potential Role As a Source Of
www.nature.com/scientificreports OPEN Microbiota of human precolostrum and its potential role as a source of bacteria to the infant mouth Received: 24 October 2018 Lorena Ruiz1,2, Rodrigo Bacigalupe3, Cristina García-Carral2,4, Alba Boix-Amoros3, Accepted: 2 April 2019 Héctor Argüello5, Camilla Beatriz Silva2,6, Maria de los Angeles Checa7, Alex Mira3 & Published: xx xx xxxx Juan M. Rodríguez 2 Human milk represents a source of bacteria for the initial establishment of the oral (and gut) microbiomes in the breastfed infant, however, the origin of bacteria in human milk remains largely unknown. While some evidence points towards a possible endogenous enteromammary route, other authors have suggested that bacteria in human milk are contaminants from the skin or the breastfed infant mouth. In this work 16S rRNA sequencing and bacterial culturing and isolation was performed to analyze the microbiota on maternal precolostrum samples, collected from pregnant women before delivery, and on oral samples collected from the corresponding infants. The structure of both ecosystems demonstrated a high proportion of taxa consistently shared among ecosystems, Streptococcus spp. and Staphylococcus spp. being the most abundant. Whole genome sequencing on those isolates that, belonging to the same species, were isolated from both the maternal and infant samples in the same mother-infant pair, evidenced that in 8 out of 10 pairs both isolates were >99.9% identical at nucleotide level. The presence of typical oral bacteria in precolostrum before contact with the newborn indicates that they are not a contamination from the infant, and suggests that at least some oral bacteria reach the infant’s mouth through breastfeeding. -

Microbial Strain-Level Population Structure and Genetic Diversity from Metagenomes
Downloaded from genome.cshlp.org on October 1, 2021 - Published by Cold Spring Harbor Laboratory Press Method Microbial strain-level population structure and genetic diversity from metagenomes Duy Tin Truong,1 Adrian Tett,1 Edoardo Pasolli,1 Curtis Huttenhower,2,3 and Nicola Segata1 1Centre for Integrative Biology, University of Trento, 38123 Trento, Italy; 2Biostatistics Department, Harvard School of Public Health, Boston, Massachusetts 02115, USA; 3The Broad Institute, Cambridge, Massachusetts 02142, USA Among the human health conditions linked to microbial communities, phenotypes are often associated with only a subset of strains within causal microbial groups. Although it has been critical for decades in microbial physiology to characterize individual strains, this has been challenging when using culture-independent high-throughput metagenomics. We introduce StrainPhlAn, a novel metagenomic strain identification approach, and apply it to characterize the genetic structure of thou- sands of strains from more than 125 species in more than 1500 gut metagenomes drawn from populations spanning North and South American, European, Asian, and African countries. The method relies on per-sample dominant sequence variant reconstruction within species-specific marker genes. It identified primarily subject-specific strain variants (<5% inter-subject strain sharing), and we determined that a single strain typically dominated each species and was retained over time (for >70% of species). Microbial population structure was correlated in several distinct ways with the geographic structure of the host population. In some cases, discrete subspecies (e.g., for Eubacterium rectale and Prevotella copri) or continuous mi- crobial genetic variations (e.g., for Faecalibacterium prausnitzii) were associated with geographically distinct human populations, whereas few strains occurred in multiple unrelated cohorts. -

The Human Milk Microbiome and Factors Influencing Its
1 THE HUMAN MILK MICROBIOME AND FACTORS INFLUENCING ITS 2 COMPOSITION AND ACTIVITY 3 4 5 Carlos Gomez-Gallego, Ph. D. ([email protected])1; Izaskun Garcia-Mantrana, Ph. D. 6 ([email protected])2, Seppo Salminen, Prof. Ph. D. ([email protected])1, María Carmen 7 Collado, Ph. D. ([email protected])1,2,* 8 9 1. Functional Foods Forum, Faculty of Medicine, University of Turku, Itäinen Pitkäkatu 4 A, 10 20014, Turku, Finland. Phone: +358 2 333 6821. 11 2. Institute of Agrochemistry and Food Technology, National Research Council (IATA- 12 CSIC), Department of Biotechnology. Valencia, Spain. Phone: +34 96 390 00 22 13 14 15 *To whom correspondence should be addressed. 16 -IATA-CSIC, Av. Agustin Escardino 7, 49860, Paterna, Valencia, Spain. Tel. +34 963900022; 17 E-mail: [email protected] 18 19 20 21 22 23 24 25 26 27 1 1 SUMMARY 2 Beyond its nutritional aspects, human milk contains several bioactive compounds, such as 3 microbes, oligosaccharides, and other substances, which are involved in host-microbe 4 interactions and have a key role in infant health. New techniques have increased our 5 understanding of milk microbiota composition, but little data on the activity of bioactive 6 compounds and their biological role in infants is available. While the human milk microbiome 7 may be influenced by specific factors, including genetics, maternal health and nutrition, mode of 8 delivery, breastfeeding, lactation stage, and geographic location, the impact of these factors on 9 the infant microbiome is not yet known. This article gives an overview of milk microbiota 10 composition and activity, including factors influencing microbial composition and their 11 potential biological relevance on infants' future health. -

Altered Fecal Short-Chain Fatty Acid Concentrations and Dysbiosis In
Received: 9 January 2019 Accepted: 3 May 2019 DOI: 10.1111/jvim.15520 STANDARD ARTICLE Fecal short-chain fatty acid concentrations and dysbiosis in dogs with chronic enteropathy Yasushi Minamoto | Tomomi Minamoto | Anitha Isaiah | Panpicha Sattasathuchana | Agostino Buono | Venkat R. Rangachari | Isaac H. McNeely | Jonathan Lidbury | Jörg M. Steiner | Jan S. Suchodolski Gastrointestinal Laboratory, Department of Small Animal Clinical Sciences, College of Abstract Veterinary Medicine and Biomedical Sciences, Background: Accumulating evidence shows an important relationship between the Texas A&M University, College Station, Texas gastrointestinal (GI) microbiota and host health. Microbial metabolites are believed to Correspondence play a critical role in host-microbial interactions. Short-chain fatty acids (SCFAs) are Jan S. Suchodolski, Gastrointestinal Laboratory, Department of Small Animal major end products of bacterial carbohydrate fermentation in the intestinal tract. Clinical Sciences, College of Veterinary Decreased concentrations of SCFAs have been observed in humans with GI disease. Medicine and Biomedical Sciences, Texas A&M University, 4474 TAMU, College Station, However, large-scale clinical data in dogs are lacking. TX 77843-4474. Hypothesis/Objective: To evaluate fecal concentrations of SCFAs and the fecal Email: [email protected] microbiota in healthy control (HC) dogs and dogs with chronic enteropathy (CE). Animals: Forty-nine privately owned HC dogs and 73 dogs with CE. Methods: Prospective cohort study. Fecal concentrations of SCFAs were measured using gas chromatography/mass spectrometry. Illumina sequencing and quantita- tive real-time polymerase chain reaction were utilized to evaluate the fecal microbiota. Results: Fecal concentrations (median [range] μmol/g of dry matter) of acetate were lower (P = .03) in dogs with CE (185.8 [20.1-1042.1]) than in HC dogs (224.0 [87.7-672.8]). -
Identification of Anaerobic Gram Negative Rods
UK Standards for Microbiology Investigations 2014 Identification of Anaerobic Gram Negative Rods FEBRUARY 24 - JANUARY 24 BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 25 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 1 of 21 © Crown copyright 2013 Identification of Anaerobic Gram Negative Rods Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website http://www.hpa.org.uk/SMI/Partnerships. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see http://www.hpa.org.uk/SMI/WorkingGroups). The contributions of many individuals in clinical, specialist and reference laboratories2014 who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: FEBRUARY 24 Standards Unit - Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ JANUARY E-mail: [email protected] 24 Website: http://www.hpa.org.uk/SMI UK Standards for Microbiology Investigations are produced in association with: BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Bacteriology – Identification | ID 25 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 2 of 21 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Anaerobic Gram Negative Rods Contents ACKNOWLEDGMENTS ......................................................................................................... -

Growth Requirements and Fermentation Products of Fusobacterium Prausnitzii, and a Proposal to Reclassify It As Faecalibacterium Prausnitzii Gen
International Journal of Systematic and Evolutionary Microbiology (2002), 52, 2141–2146 DOI: 10.1099/ijs.0.02241-0 Growth requirements and fermentation products of Fusobacterium prausnitzii, and a proposal to reclassify it as Faecalibacterium prausnitzii gen. nov., comb. nov. 1 Division of Gut Sylvia H. Duncan,1 Georgina L. Hold,1 Hermie J. M. Harmsen,2 Microbiology and 1 1 Immunology, Rowett Colin S. Stewart and Harry J. Flint Research Institute, Greenburn Road, Bucksburn, Aberdeen Author for correspondence: Sylvia H. Duncan. Tel: j44 1224 712751. Fax: j44 1224 716687. AB21 9SB, UK e-mail: shd!rri.sari.ac.uk 2 Department of Medical Microbiology, University of Groningen, Groningen, Two newly isolated strains of obligately anaerobic bacteria from human faeces The Netherlands are shown here to be related to Fusobacterium prausnitzii, which is regarded as one of the most abundant colonizers of the human colon. These strains, along with Fusobacterium prausnitzii ATCC 27768T and 27766, are non-motile and produce butyrate, formate and lactate, but not hydrogen as fermentation products. A new finding is that all four strains produce D-lactate, but not L- lactate. The strains have a requirement for acetate in the growth medium and this may account for the previously reported requirement for rumen fluid. The DNA GMC content of the four strains is 47–57 mol%. Together with phylogenetic analysis based on 16S rRNA sequencing, this establishes that Fusobacterium prausnitzii strains are only distantly related to Fusobacterium sensu stricto and are more closely related to members of Clostridium cluster IV (the Clostridium leptum group). It is proposed that a new genus, Faecalibacterium gen. -

Studying Vertical Microbiome Transmission from Mothers to Infants by Strain-Level Metagenomic Profiling
bioRxiv preprint doi: https://doi.org/10.1101/081828; this version posted October 21, 2016. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. 1 Studying vertical microbiome transmission from mothers to infants by strain-level metagenomic profiling Francesco Asnicar*,1, Serena Manara*,1, Moreno Zolfo1, Duy Tin Truong1, Matthias Scholz1, Federica Armanini1, Pamela Ferretti1, Valentina Gorfer2, Anna Pedrotti2, Adrian Tett1,#, Nicola Segata1,# * Equal contribution # Corresponding authors: [email protected], [email protected] 1 Centre for Integrative Biology, University of Trento, Italy 2 Azienda Provinciale per i Servizi Sanitari, Trento, Italy Abstract The gut microbiome starts to be shaped in the first days of life and continues to increase its diversity during the first months. Several investigations are assessing the link between the configuration of the infant gut microbiome and infant health, but a comprehensive strain-level assessment of vertically transmitted microbes from mother to infant is still missing. We longitudinally collected fecal and breast milk samples from multiple mother-infant pairs during the first year of life, and applied shotgun metagenomic sequencing followed by strain-level profiling. We observed several specific strains including those from Bifidobacterium bifidum, Coprococcus comes, and Ruminococcus bromii, that were present in samples from the same mother-infant pair, while being clearly distinct from those carried by other pairs, which is indicative of vertical transmission. We further applied metatranscriptomics to study the in vivo expression of vertically transmitted microbes, for example Bacteroides vulgatus and Bifidobacterium spp., thus suggesting that transmitted strains are functionally active in the two rather different environments of the adult and infant guts.