Clinical Characteristics of Fusobacterial Brain Abscess
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
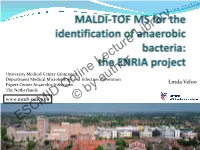
MALDI-TOF MS for the Identification of Anaerobic Bacteria
University Medical Center Groningen Department Medical Microbiology and Infection Prevention Linda Veloo Expert Center Anaerobic Infections The Netherlands www.mmb-umcg.eu © by author ESCMID Online Lecture Library Matrix Assisted Laser Desorption/Ionization time-of-flight Mass Spectrometry (MALDI-TOF MS) Time of flight tube Target at 15-25 kV Detector Ion source © by author ESCMID- “Time of flight” Online of individual Lecture proteins is converted Library into mass information. - Spectrum is produced - Database is built Veloo et al. Anaerobe 2011; 17:211-212 Workflow Direct spotting of bacteria on target using a toothpick Add HCCA matrix Data acquisition © Databy analyses author ESCMID Online Lecture Library Log score: <1.7 no reliable identification 1.7 – 2.0 reliable genus identification ≥ 2.0 reliable species identification Obtained spectrum is unique for bacterial species Intensity © by author ESCMID Online Lecture Library Anaerobic culture Phenotypic pure culture primary incubation 2 days 2-7 days aerotolerance identification MALDI-TOF MS 1 day 2-14 days primary incubation 2-7 days © by author MALDI-TOF MS testing minutes ESCMID Online Lecture Library How many anaerobic bacteria can be identified using MALDI-TOF MS? UMCG 2011/2012 Total no. of strains 1000 Species ID 650 65% Genus ID 149 15% No ID © 201by author20% ESCMID Online Lecture Library Performance differs per genus Genus* % species ID % genus ID Clostridium sp. (n=149) 97 3 B. fragilis sp. (n=179) 97 3 Parabacteroides sp. (n=14) 93 7 GPAC (n=133) 85 15 Prevotella sp.(n=83) 78 12 Propionibacterium sp. (n=129) 64 36 Actinomyces sp. (n=28) 57 43 Fusobacterium sp. -

Microbiota of Human Precolostrum and Its Potential Role As a Source Of
www.nature.com/scientificreports OPEN Microbiota of human precolostrum and its potential role as a source of bacteria to the infant mouth Received: 24 October 2018 Lorena Ruiz1,2, Rodrigo Bacigalupe3, Cristina García-Carral2,4, Alba Boix-Amoros3, Accepted: 2 April 2019 Héctor Argüello5, Camilla Beatriz Silva2,6, Maria de los Angeles Checa7, Alex Mira3 & Published: xx xx xxxx Juan M. Rodríguez 2 Human milk represents a source of bacteria for the initial establishment of the oral (and gut) microbiomes in the breastfed infant, however, the origin of bacteria in human milk remains largely unknown. While some evidence points towards a possible endogenous enteromammary route, other authors have suggested that bacteria in human milk are contaminants from the skin or the breastfed infant mouth. In this work 16S rRNA sequencing and bacterial culturing and isolation was performed to analyze the microbiota on maternal precolostrum samples, collected from pregnant women before delivery, and on oral samples collected from the corresponding infants. The structure of both ecosystems demonstrated a high proportion of taxa consistently shared among ecosystems, Streptococcus spp. and Staphylococcus spp. being the most abundant. Whole genome sequencing on those isolates that, belonging to the same species, were isolated from both the maternal and infant samples in the same mother-infant pair, evidenced that in 8 out of 10 pairs both isolates were >99.9% identical at nucleotide level. The presence of typical oral bacteria in precolostrum before contact with the newborn indicates that they are not a contamination from the infant, and suggests that at least some oral bacteria reach the infant’s mouth through breastfeeding. -
Identification of Anaerobic Gram Negative Rods
UK Standards for Microbiology Investigations 2014 Identification of Anaerobic Gram Negative Rods FEBRUARY 24 - JANUARY 24 BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 25 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 1 of 21 © Crown copyright 2013 Identification of Anaerobic Gram Negative Rods Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website http://www.hpa.org.uk/SMI/Partnerships. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see http://www.hpa.org.uk/SMI/WorkingGroups). The contributions of many individuals in clinical, specialist and reference laboratories2014 who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: FEBRUARY 24 Standards Unit - Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ JANUARY E-mail: [email protected] 24 Website: http://www.hpa.org.uk/SMI UK Standards for Microbiology Investigations are produced in association with: BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Bacteriology – Identification | ID 25 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 2 of 21 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Anaerobic Gram Negative Rods Contents ACKNOWLEDGMENTS ......................................................................................................... -

Growth Requirements and Fermentation Products of Fusobacterium Prausnitzii, and a Proposal to Reclassify It As Faecalibacterium Prausnitzii Gen
International Journal of Systematic and Evolutionary Microbiology (2002), 52, 2141–2146 DOI: 10.1099/ijs.0.02241-0 Growth requirements and fermentation products of Fusobacterium prausnitzii, and a proposal to reclassify it as Faecalibacterium prausnitzii gen. nov., comb. nov. 1 Division of Gut Sylvia H. Duncan,1 Georgina L. Hold,1 Hermie J. M. Harmsen,2 Microbiology and 1 1 Immunology, Rowett Colin S. Stewart and Harry J. Flint Research Institute, Greenburn Road, Bucksburn, Aberdeen Author for correspondence: Sylvia H. Duncan. Tel: j44 1224 712751. Fax: j44 1224 716687. AB21 9SB, UK e-mail: shd!rri.sari.ac.uk 2 Department of Medical Microbiology, University of Groningen, Groningen, Two newly isolated strains of obligately anaerobic bacteria from human faeces The Netherlands are shown here to be related to Fusobacterium prausnitzii, which is regarded as one of the most abundant colonizers of the human colon. These strains, along with Fusobacterium prausnitzii ATCC 27768T and 27766, are non-motile and produce butyrate, formate and lactate, but not hydrogen as fermentation products. A new finding is that all four strains produce D-lactate, but not L- lactate. The strains have a requirement for acetate in the growth medium and this may account for the previously reported requirement for rumen fluid. The DNA GMC content of the four strains is 47–57 mol%. Together with phylogenetic analysis based on 16S rRNA sequencing, this establishes that Fusobacterium prausnitzii strains are only distantly related to Fusobacterium sensu stricto and are more closely related to members of Clostridium cluster IV (the Clostridium leptum group). It is proposed that a new genus, Faecalibacterium gen. -

Faecalibacterium Prausnitzii: from Microbiology to Diagnostics and Prognostics
The ISME Journal (2017) 11, 841–852 © 2017 International Society for Microbial Ecology All rights reserved 1751-7362/17 www.nature.com/ismej MINI REVIEW Faecalibacterium prausnitzii: from microbiology to diagnostics and prognostics Mireia Lopez-Siles1, Sylvia H Duncan2, L Jesús Garcia-Gil1 and Margarita Martinez-Medina1 1Laboratori de Microbiologia Molecular, Departament de Biologia, Universitat de Girona, Girona, Spain and 2Microbiology Group, Rowett Institute of Nutrition and Health, University of Aberdeen, Aberdeen, UK There is an increasing interest in Faecalibacterium prausnitzii, one of the most abundant bacterial species found in the gut, given its potentially important role in promoting gut health. Although some studies have phenotypically characterized strains of this species, it remains a challenge to determine which factors have a key role in maintaining the abundance of this bacterium in the gut. Besides, phylogenetic analysis has shown that at least two different F. prausnitzii phylogroups can be found within this species and their distribution is different between healthy subjects and patients with gut disorders. It also remains unknown whether or not there are other phylogroups within this species, and also if other Faecalibacterium species exist. Finally, many studies have shown that F. prausnitzii abundance is reduced in different intestinal disorders. It has been proposed that F. prausnitzii monitoring may therefore serve as biomarker to assist in gut diseases diagnostics. In this mini- review, we aim to serve as an overview of F. prausnitzii phylogeny, ecophysiology and diversity. In addition, strategies to modulate the abundance of F. prausnitzii in the gut as well as its application as a biomarker for diagnostics and prognostics of gut diseases are discussed. -

Laboratory Diagnosis of Sexually Transmitted Infections, Including Human Immunodeficiency Virus
Laboratory diagnosis of sexually transmitted infections, including human immunodeficiency virus human immunodeficiency including Laboratory transmitted infections, diagnosis of sexually Laboratory diagnosis of sexually transmitted infections, including human immunodeficiency virus Editor-in-Chief Magnus Unemo Editors Ronald Ballard, Catherine Ison, David Lewis, Francis Ndowa, Rosanna Peeling For more information, please contact: Department of Reproductive Health and Research World Health Organization Avenue Appia 20, CH-1211 Geneva 27, Switzerland ISBN 978 92 4 150584 0 Fax: +41 22 791 4171 E-mail: [email protected] www.who.int/reproductivehealth 7892419 505840 WHO_STI-HIV_lab_manual_cover_final_spread_revised.indd 1 02/07/2013 14:45 Laboratory diagnosis of sexually transmitted infections, including human immunodeficiency virus Editor-in-Chief Magnus Unemo Editors Ronald Ballard Catherine Ison David Lewis Francis Ndowa Rosanna Peeling WHO Library Cataloguing-in-Publication Data Laboratory diagnosis of sexually transmitted infections, including human immunodeficiency virus / edited by Magnus Unemo … [et al]. 1.Sexually transmitted diseases – diagnosis. 2.HIV infections – diagnosis. 3.Diagnostic techniques and procedures. 4.Laboratories. I.Unemo, Magnus. II.Ballard, Ronald. III.Ison, Catherine. IV.Lewis, David. V.Ndowa, Francis. VI.Peeling, Rosanna. VII.World Health Organization. ISBN 978 92 4 150584 0 (NLM classification: WC 503.1) © World Health Organization 2013 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO web site (www.who.int/about/licensing/copyright_form/en/index.html). -

Fusobacterium Nucleatum Subspecies Animalis Influences Proinflammatory Cytokine Expression and Monocyte Activation in Human Colorectal Tumors
Published OnlineFirst May 8, 2017; DOI: 10.1158/1940-6207.CAPR-16-0178 Research Article Cancer Prevention Research Fusobacterium Nucleatum Subspecies Animalis Influences Proinflammatory Cytokine Expression and Monocyte Activation in Human Colorectal Tumors Xiangcang Ye1, Rui Wang1, Rajat Bhattacharya1, Delphine R. Boulbes1, Fan Fan1, Ling Xia1, Harish Adoni1, Nadim J. Ajami2, Matthew C. Wong2, Daniel P. Smith2, Joseph F. Petrosino2, Susan Venable3, Wei Qiao4, Veera Baladandayuthapani4, Dipen Maru5, and Lee M. Ellis1,6 Abstract Chronic infection and associated inflammation have using immunoassays and found that expression of the long been suspected to promote human carcinogenesis. cytokines IL17A and TNFa was markedly increased but Recently, certain gut bacteria, including some in the Fuso- IL21 decreased in the colorectal tumors. Furthermore, the bacterium genus, have been implicated in playing a role in chemokine (C-C motif) ligand 20 was differentially human colorectal cancer development. However, the Fuso- expressed in colorectal tumors at all stages. In in vitro co- bacterium species and subspecies involved and their onco- culture assays, F. nucleatum ssp. animalis induced CCL20 genic mechanisms remain to be determined. We sought to protein expression in colorectal cancer cells and monocytes. identify the specific Fusobacterium spp. and ssp. in clinical It also stimulated the monocyte/macrophage activation and colorectal cancer specimens by targeted sequencing of migration. Our observations suggested that infection with Fusobacterium 16S ribosomal RNA gene. Five Fusobacterium F. nucleatum ssp. animalis in colorectal tissue could induce spp. were identified in clinical colorectal cancer specimens. inflammatory response and promote colorectal cancer Additional analyses confirmed that Fusobacterium nuclea- development. Further studies are warranted to determine tum ssp. -

University of Ghana College of Basic and Applied Sciences by Shirley Victoria Simpson (10551058) This Thesis Is Submitted To
UNIVERSITY OF GHANA COLLEGE OF BASIC AND APPLIED SCIENCES ISOLATION AND CHARACTERIZATION of Haemophilus ducreyi STRAINS FROM CHILDREN WITH CUTANEOUS LESIONS IN YAWS ENDEMIC REGIONS, GHANA BY SHIRLEY VICTORIA SIMPSON (10551058) THIS THESIS IS SUBMITTED TO THE UNIVERSITY OF GHANA, LEGON IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE AWARD OF MPHIL MOLECULAR CELL BIOLOGY OF INFECTIOUS DISEASES DEGREE JULY, 2017 DECLARATION This is to certify that this thesis is the result of research undertaken by me, Shirley Victoria Simpson towards the award of Master of Philosophy in Molecular Cell Biology of Infectious Diseases in the Department of Biochemistry, Cell and Molecular Biology, School of Biological Sciences, College of Basic And Applied Sciences, University of Ghana. Signature--------------------------------------- Date-------------------------- Shirley Victoria Simpson (Candidate) Signature--------------------------------------- Date----------------------- Prof. Kennedy Kwasi Addo (Supervisor) Signature------------------------------------ Date----------------------- Dr. Lydia Mosi (Co-Supervisor) i ABSTRACT Recent discovery of cutaneous H. ducreyi has complicated the epidemiology of Yaws in endemic countries. Yaws and H. ducreyi ulcers are clinically indistinguishable from each other and some other causes of skin ulcerations. The aim of the study was to isolate and characterize H. ducreyi strains from lesions of children in yaws-endemic areas. Symptomatic patients were first screened with Dual Path Platform (DPP-RDT) Syphilis Screen & Confirm test kit (Chembio, Medford, New York) for yaws. Lesion exudates were tested by culture for H. ducreyi and real-time multiplex PCR assays were used to identify T.p subsp. pertenue DNA and H. ducreyi DNA. Azithromycin (AZT) resistance markers were screened for in T.p subsp. pertenue PCR positives. Bacterial 16S rRNA gene was amplified and sequenced to detect the presence of other pathogenic bacteria. -

An Insight Into Pericoronitis REVIEW ARTICLE
Dhonge RP et al: An Insight Into Pericoronitis REVIEW ARTICLE An Insight into Pericoronitis Roshan P. Dhonge1, R. M. Zade2, V. Gopinath3, Ramesh Amirisetty4 1- Post Graduate Student, Department of Periodontology, Chhattisgarh Dental College And Research Institute, Rajnandgaon, Chhattisgarh (India). 2- Professor, HOD and Dean, Department of Periodontology, Chhattisgarh Dental College And Research Correspondence to: Institute, Rajnandgaon, Chhattisgarh (India). 3- Professor, Department of Dr. Roshan P. Dhonge, 10, Ganesh Vihar No. I, Near Periodontology, Chhattisgarh Dental College And Research Institute, Rajnandgaon, Swastik Nagar and Water Tank, Amravati, Maharashtra, Chhattisgarh (India). 4- Reader, Department of Periodontology, Chhattisgarh Dental India. College And Research Institute, Rajnandgaon, Chhattisgarh (India). ABSTRACT Pericoronitis is inflammation of the soft tissue associated with the crown of a partially erupted tooth. It is seen most commonly in relation to the mandibular third molar. The common symptoms and signs are pain, swelling, trismus, halitosis, bad taste, inflammation of pericoronal flap and pus discharge from underneath it, inflammation sometimes aggravated by trauma from an antagonist tooth. In severe episodes, an acute pericoronal abscess may develop which may remain localized or spread to involve one or more of the adjacent deep surgical spaces and may be associated with systemic as well as local signs and symptoms. The treatment for acute phase include debridement of plaque and food debris, drainage of pus, irrigation with sterile saline, chlorhexidine or hydrogen peroxide, elimination of occlusal trauma and prophylactic antibiotic along with analgesics. The treatment planning for surgical intervention will be made after acute phase subsided. An extraction of partially or completely impacted third molar should be done. -

Microbiota Network and Mathematic Microbe Mutualism in Colostrum and Mature Milk Collected in Two Different Geographic Areas: Italy Versus Burundi
The ISME Journal (2017) 11, 875–884 OPEN © 2017 International Society for Microbial Ecology All rights reserved 1751-7362/17 www.nature.com/ismej ORIGINAL ARTICLE Microbiota network and mathematic microbe mutualism in colostrum and mature milk collected in two different geographic areas: Italy versus Burundi Lorenzo Drago1,2, Marco Toscano1, Roberta De Grandi2, Enzo Grossi3, Ezio M Padovani4 and Diego G Peroni5,6 1Clinical Chemistry and Microbiology Laboratory, IRCCS Galeazzi Orthopaedic Institute, Milan, Italy; 2Clinical Microbiology Laboratory, Department of Biomedical Science for Health, University of Milan, Milan, Italy; 3Villa Santa Maria Institute, Via IV Novembre Tavernerio, Como, Italy; 4Pediatric Department, University of Verona & Pro-Africa Foundation, Verona, Italy; 5Department of Clinical and Experimental Medicine, Section of Pediatrics, University of Pisa, Pisa, Italy and 6International Inflammation (in-FLAME) Network of the World Universities Network, Sydney, NSW, Australia Human milk is essential for the initial development of newborns, as it provides all nutrients and vitamins, such as vitamin D, and represents a great source of commensal bacteria. Here we explore the microbiota network of colostrum and mature milk of Italian and Burundian mothers using the auto contractive map (AutoCM), a new methodology based on artificial neural network (ANN) architecture. We were able to demonstrate the microbiota of human milk to be a dynamic, and complex, ecosystem with different bacterial networks among different populations containing diverse microbial hubs and central nodes, which change during the transition from colostrum to mature milk. Furthermore, a greater abundance of anaerobic intestinal bacteria in mature milk compared with colostrum samples has been observed. The association of complex mathematic systems such as ANN and AutoCM adopted to metagenomics analysis represents an innovative approach to investigate in detail specific bacterial interactions in biological samples. -

Fusobacterium Nucleatum, Strain CTI-03 Catalog No. HM-994 for Research Use Only. Not for Human Use
Product Information Sheet for HM-994 Fusobacterium nucleatum, Strain CTI-03 immediately upon arrival. For long-term storage, the vapor phase of a liquid nitrogen freezer is recommended. Freeze- thaw cycles should be avoided. Catalog No. HM-994 Growth Conditions: For research use only. Not for human use. Media: Modified Chopped Meat medium or equivalent Contributor: Tryptic Soy agar with 5% defibrinated sheep blood or Wendy S. Garrett, M.D., Ph.D., Assistant Professor, and equivalent Aleksander D. Kostic, Department of Immunology and Incubation: Infectious Diseases, Harvard School of Public Health, Boston, Temperature: 37°C Massachusetts, USA Atmosphere: Anaerobic Propagation: Manufacturer: 1. Keep vial frozen until ready for use, then thaw. BEI Resources 2. Transfer the entire thawed aliquot into a single tube of broth. Product Description: 3. Use several drops of the suspension to inoculate an Bacteria Classification: Fusobacteriaceae, Fusobacterium agar slant and/or plate. Species: Fusobacterium nucleatum 4. Incubate the tube, slant and/or plate at 37°C for 24 to 72 Strain: CTI-03 hours. Original Source: Fusobacterium nucleatum (F. nucleatum), strain CTI-03 was isolated in 2012 from colonic tumor tissue Citation: from a human patient with colorectal carcinoma in Acknowledgment for publications should read “The following Massachusetts, USA.1 reagent was obtained through BEI Resources, NIAID, NIH as Comments: F. nucleatum, strain CTI-03 (HMP ID 1540) is a part of the Human Microbiome Project: Fusobacterium reference genome for The Human Microbiome Project nucleatum, Strain CTI-03, HM-994.” (HMP). HMP is an initiative to identify and characterize human microbial flora. The complete genome of F. -

Reevaluating the Fusobacterium Virulence Factor Landscape 1* 1* 1 1 2 Ariana Umana , Blake E
bioRxiv preprint doi: https://doi.org/10.1101/534297; this version posted January 29, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Reevaluating the Fusobacterium Virulence Factor Landscape 1* 1* 1 1 2 Ariana Umana , Blake E. Sanders , Chris C. Yoo , Michael A. Casasanta , Barath Udayasuryan , Scott 2 1,# S. Verbridge , Daniel J. Slade 1 Department of Biochemistry, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA. 2 Laboratory of Integrative Tumor Ecology, and Virginia Tech – Wake Forest School of Biomedical Engineering and Sciences, Blacksburg, VA, USA *These authors contributed equally # To whom correspondence should be addressed: Dr. Daniel J. Slade, Department of Biochemistry, Virginia Polytechnic Institute and State University, Blacksburg, VA 24061. Telephone: +1 (540) 231-2842. Email: [email protected] ________________________________________________________________________________________ ABSTRACT Fusobacterium are Gram-negative, anaerobic, opportunistic pathogens involved in multiple diseases, including the oral pathogen Fusobacterium nucleatum being linked to the progression and severity of colorectal cancer. The global identification of virulence factors in Fusobacterium has been greatly hindered by a lack of properly assembled and annotated genomes. Using newly completed genomes from nine strains and seven species of Fusobacterium, we report the identification and correction of virulence factors from the Type 5 secreted autotransporter and FadA protein families, with a focus on the genetically tractable strain F. nucleatum subsp. nucleatum ATCC 23726 and the classic typed strain F. nucleatum subsp.