Insect Repellents • Men Reside Or Travel to Endemic Area: Abstinence, Consistently Use Condoms Notes on Insect Repellants
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

'Tqiltfl Gn Qrahdt 'T.T+Ttfl - 3Cg U\To
qlc{l}s'fts d'r rL'ftl-tct oilc{-sfl 'tqiltfl gN qRaHdt 't.t+ttfl - 3Cg U\tO r5rfr I ff EEtf,IlFfrt u f Effltfy lt|.[b.ft rrti uQqarcj.e{ tI[ troa C tJdderor il.&a, ?ooc scrrr u (r) o{l Page No.-1 f,iar- o{l qRqa t{ls (irL{l.oer .rdt.rfl fd.atclotL ct.3 \/oL/?oog, crr'oc/oc/?o1'e{ ' q2t {lrlSl-loeoog-3 3 tt3 sY-r,rtaAqttjil.e r'ti' sct ufdtrr{lat s}tis "i' q"cf otg r{. - ? o q, d[. O S,/o Y,/ ? o t q D' ) {./ ?U / 3 . 3,/ Y 3 o t Uq'o / t Ul{|'qtq'( r,tell uqtQ.a secrt:{ l,tta. E } {[d.ft r,t[Qstt r't[0'G.qq"t 5a{ - u dact.{ +qai m&e sa.rt"t ortqaf riLl}.sA.t Stualsr G.A.D.) ql "[L sl{ rtat i.qn sr.rt:{i r,tO.a E. qi. at. ot,/ott/?o?o"t qQ(Adl uutgl rtuaa sacrtul r,rtda D. ar{trrt - te,/oq,/?o?o ql.cft)s'fts o't A"{l{a ou"s{l 't.til{t 5G. qRqHdl "t.{il{-3CS YttO ,ffiu )aftgf't.t. oesgo Qet c?Y .ra<,ig daaafl sldn <.r+u{ gR qG.oRdt dqut{-3e9 u\to Page No.-2 {r[dd ui uRqqcj.E ot/or{/?o?o r,rqstrQlsr 93?gt [d.ot.t ULctL dtGt? 1. {+urq {+errua, GEeit, stqf ui gerf"0 ficra] ox {+€rtat u[0.stflr,i. -
![[46I ] the SENSORY PHYSIOLOGY of the HARVEST MITE](https://docslib.b-cdn.net/cover/7751/46i-the-sensory-physiology-of-the-harvest-mite-227751.webp)
[46I ] the SENSORY PHYSIOLOGY of the HARVEST MITE
[46i ] THE SENSORY PHYSIOLOGY OF THE HARVEST MITE TROMBICULA AUTUMNALIS SHAW BY B. M. JONES Department of Zoology, University of Edinburgh (Received 18 May 1950) (With Twenty-four Text-figures) INTRODUCTION The ectoparasitic habit of the hexapod larva of Trombicula autumnalis is the cause of much discomfort to residents of infected localities in the British Isles, between late June and the beginning of October. The mite is a member of the Trombiculid group which includes species known to transmit disease in some parts of the world. The unfed larvae are found either upon the soil or climbing upon low-lying vegetation. Under suitable conditions they aggregate into clusters and are then more easily detected as orange patches. Development to the nymphal stage cannot take place unless the larvae obtain a meal from the superficial tissue of a vertebrate host to which they must securely attach themselves. The nymphs and adults are non-parasitic and lead a hypogeal existence at a depth of about 12 in. below the surface of the soil (Cockings, 1948). The hairs of a mammal, or the feathers of a bird, as they brush against infected soil or low-lying vegetation, are admirably suited for picking up the mites, but the question arises, to what extent are sensory perceptions of environmental stimuli of the mites directed towards the acquisition of a host. The chief aim of the present work has therefore been to investigate (a) the responses of the mite to stimuli most likely to have value with respect to the problem of acquiring a host, and (b) the nature of the sensory organs. -

Arthropod Parasites in Domestic Animals
ARTHROPOD PARASITES IN DOMESTIC ANIMALS Abbreviations KINGDOM PHYLUM CLASS ORDER CODE Metazoa Arthropoda Insecta Siphonaptera INS:Sip Mallophaga INS:Mal Anoplura INS:Ano Diptera INS:Dip Arachnida Ixodida ARA:Ixo Mesostigmata ARA:Mes Prostigmata ARA:Pro Astigmata ARA:Ast Crustacea Pentastomata CRU:Pen References Ashford, R.W. & Crewe, W. 2003. The parasites of Homo sapiens: an annotated checklist of the protozoa, helminths and arthropods for which we are home. Taylor & Francis. Taylor, M.A., Coop, R.L. & Wall, R.L. 2007. Veterinary Parasitology. 3rd edition, Blackwell Pub. HOST-PARASITE CHECKLIST Class: MAMMALIA [mammals] Subclass: EUTHERIA [placental mammals] Order: PRIMATES [prosimians and simians] Suborder: SIMIAE [monkeys, apes, man] Family: HOMINIDAE [man] Homo sapiens Linnaeus, 1758 [man] ARA:Ast Sarcoptes bovis, ectoparasite (‘milker’s itch’)(mange mite) ARA:Ast Sarcoptes equi, ectoparasite (‘cavalryman’s itch’)(mange mite) ARA:Ast Sarcoptes scabiei, skin (mange mite) ARA:Ixo Ixodes cornuatus, ectoparasite (scrub tick) ARA:Ixo Ixodes holocyclus, ectoparasite (scrub tick, paralysis tick) ARA:Ixo Ornithodoros gurneyi, ectoparasite (kangaroo tick) ARA:Pro Cheyletiella blakei, ectoparasite (mite) ARA:Pro Cheyletiella parasitivorax, ectoparasite (rabbit fur mite) ARA:Pro Demodex brevis, sebacceous glands (mange mite) ARA:Pro Demodex folliculorum, hair follicles (mange mite) ARA:Pro Trombicula sarcina, ectoparasite (black soil itch mite) INS:Ano Pediculus capitis, ectoparasite (head louse) INS:Ano Pediculus humanus, ectoparasite (body -
What's Eating You? Chiggers
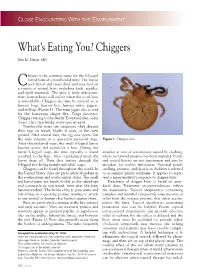
CLOSE ENCOUNTERS WITH THE ENVIRONMENT What’s Eating You? Chiggers Dirk M. Elston, MD higger is the common name for the 6-legged larval form of a trombiculid mite. The larvae C suck blood and tissue fluid and may feed on a variety of animal hosts including birds, reptiles, and small mammals. The mite is fairly indiscrimi- nate; human hosts will suffice when the usual host is unavailable. Chiggers also may be referred to as harvest bugs, harvest lice, harvest mites, jiggers, and redbugs (Figure 1). The term jigger also is used for the burrowing chigoe flea, Tunga penetrans. Chiggers belong to the family Trombiculidae, order Acari, class Arachnida; many species exist. Trombiculid mites are oviparous; they deposit their eggs on leaves, blades of grass, or the open ground. After several days, the egg case opens, but the mite remains in a quiescent prelarval stage. Figure 1. Chigger mite. After this prelarval stage, the small 6-legged larvae become active and search for a host. During this larval 6-legged stage, the mite typically is found attaches at sites of constriction caused by clothing, attached to the host. After a prolonged meal, the where its forward progress has been impeded. Penile larvae drop off. Then they mature through the and scrotal lesions are not uncommon and may be 8-legged free-living nymph and adult stages. mistaken for scabies infestation. Seasonal penile Chiggers can be found throughout the world. In swelling, pruritus, and dysuria in children is referred the United States, they are particularly abundant in to as summer penile syndrome. -

Leptotrombidium Deliense
ISSN (Print) 0023-4001 ISSN (Online) 1738-0006 Korean J Parasitol Vol. 56, No. 4: 313-324, August 2018 ▣ MINI REVIEW https://doi.org/10.3347/kjp.2018.56.4.313 Research Progress on Leptotrombidium deliense 1,2 1,2 1 Yan Lv , Xian-Guo Guo *, Dao-Chao Jin 1Institute of Entomology, Guizhou University, and the Provincial Key Laboratory for Agricultural Pest Management in Mountainous Region, Guiyang 550025, P. R. China; 2Vector Laboratory, Institute of Pathogens and Vectors, Yunnan Provincial Key Laboratory for Zoonosis Control and Prevention, Dali University, Dali, Yunnan Province 671000, P. R. China Abstract: This article reviews Leptotrombidium deliense, including its discovery and nomenclature, morphological features and identification, life cycle, ecology, relationship with diseases, chromosomes and artificial cultivation. The first record of L. deliense was early in 1922 by Walch. Under the genus Leptotrombidium, there are many sibling species similar to L. de- liense, which makes it difficult to differentiate L. deliense from another sibling chigger mites, for example, L. rubellum. The life cycle of the mite (L. deliense) includes 7 stages: egg, deutovum (or prelarva), larva, nymphochrysalis, nymph, ima- gochrysalis and adult. The mite has a wide geographical distribution with low host specificity, and it often appears in differ- ent regions and habitats and on many species of hosts. As a vector species of chigger mite, L. deliense is of great impor- tance in transmitting scrub typhus (tsutsugamushi disease) in many parts of the world, especially in tropical regions of Southeast Asia. The seasonal fluctuation of the mite population varies in different geographical regions. The mite has been successfully cultured in the laboratory, facilitating research on its chromosomes, biochemistry and molecular biology. -

ESCCAP Guidelines Final
ESCCAP Malvern Hills Science Park, Geraldine Road, Malvern, Worcestershire, WR14 3SZ First Published by ESCCAP 2012 © ESCCAP 2012 All rights reserved This publication is made available subject to the condition that any redistribution or reproduction of part or all of the contents in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise is with the prior written permission of ESCCAP. This publication may only be distributed in the covers in which it is first published unless with the prior written permission of ESCCAP. A catalogue record for this publication is available from the British Library. ISBN: 978-1-907259-40-1 ESCCAP Guideline 3 Control of Ectoparasites in Dogs and Cats Published: December 2015 TABLE OF CONTENTS INTRODUCTION...............................................................................................................................................4 SCOPE..............................................................................................................................................................5 PRESENT SITUATION AND EMERGING THREATS ......................................................................................5 BIOLOGY, DIAGNOSIS AND CONTROL OF ECTOPARASITES ...................................................................6 1. Fleas.............................................................................................................................................................6 2. Ticks ...........................................................................................................................................................10 -

Epidemiology and Treatment of Sarcoptic Mange in Bu:Ffalo Calves Around Lahore
Paki.wan Vel. J.. 18 (/ J · !91JS EPIDEMIOLOGY AND TREATMENT OF SARCOPTIC MANGE IN BU:FFALO CALVES AROUND LAHORE Farhat Jabeen. N. Ahmad1, M. Anwar Chaudhry and Ijaz Javed1 Livestock and Dairy Development Department. Punjab. 1Facuhy of Veterinary Science. University of Agriculture. Faisalabad. Pakistan ABSTRACT A project was conducted to study the prevalence of sarcoptic mange in buffalo calves around Lahore city. The effects of age and sex of the calf and the seasons of the year on the incidence of this disease were also investigated. For this purpose, 2000 buffalo calves. varying in age from I to 12 momhs. \Verc examined over a 12 month period, from January to December, 1994. The results showed thai 7. 00 1;; ' 140 out of 2000) of the calves were infected with the disease. The highest prevalence ( 12.67%) was recorded in winter while the lowest (0.46%) in summer. During spring and autumn, the prevalence of the problem was R. 94 and 8. 17%, respectively. Sex of the calf did not seem to influence the prevalence <51 .42 1fr; for malt calves and 48.58% for females). However. the prevalence was remarkably higher among calves less than 8 months of age than 8-12 month old calves (82.14 v 17.86%). External trealment of 35 affected culves with 0.2% solution of Neguvon resulted in 100% recovery within 20 day�. INTRODUCTION MATERIALS AND l\1ETH(lDS Ectoparasitcs are responsible for great economic A total of 2000 buffalo calves. varying in a�e frum losses to liveswck industry . Btsides causing great to 12 months, were examined for the pn:scncc 11! irritation and unrest. -

Comparative Effects of Growth Inhibitors on Sterol Metabolism in the Nematode Caenorhabditis Elegans
Camp. Biochem. Physiol. Vol. 79C, No. 1, pp. 21-26, 1984 0306-4492/84$3.00 + 0.00 Printed in Great Britain 0 1984Pergamon Press Ltd COMPARATIVE EFFECTS OF GROWTH INHIBITORS ON STEROL METABOLISM IN THE NEMATODE CAENORHABDITIS ELEGANS RUBEN LOZANO*~, DAVID J. CHITWOOD, WILLIAM R. LUSBY, MALCOLM J. THOMPSON, JAMES A. SVOBODA and GLENN W. PATTERSON* Insect Physiology Laboratory, ARS, USDA, Beltsville, MD 20705 and *Department of Botany, University of Maryland, College Park, MD 20742, USA. Telephone: (301) 344-2389 (Received 9 February 1984) Abstract-l. An analogous series of dimethylalkyl compounds, consisting of four amines, an amide, and a phosphonate ester, inhibited motility and reproduction of the nematode Caenorhabditis elegans. 2. Dimethylamines with straight-chain lengths of 12, 14, or 16 carbon atoms were equally active nematicides, causing greater than 80% population growth inhibition at a concentration of 25 ppm. 3. The C,, straight-chain amine and its corresponding amide produced similar inhibition and were much more potent than either the corresponding C,, phosphonate or a C,, branched-chain amine. 4. Inhibition of the A”-sterol reductase system was exhibited by all four amines, but not by the amide or phosphonate, in the following order of activity: C,2 branched-chain amine > C,? straight-chain amine > C,, amine > C,, amine. 5. The C,, branched amine also blocked the C-24(28)-dehydrogenase system in the conversion of sitosterol to fucosterol, the initial step in sitosterol dealkylation. INTRODUCTION 1978; Svoboda et al., 1978; Thompson et al., 1978). In some cases, they blocked conversion of phy- Research of model compounds as potential agricul- tosterols to cholesterol in insects (Robbins et al., tural pesticides has revealed interesting biological 1975; Cohen et al., 1983). -
Class: Arachnida
Class: Arachnida Mk- vthr dqekj ijthoh foKku foHkkx fcgkj Ik’kqfpfdRlk egkfo|ky; fcgkj Ik’kq foKku fo’ofo|ky; iVuk&800014 ¼fcgkj½ Image source: Google image Phylum: Arthropoda CLASSIFICATION: Phylum: Arthropoda Classes Insecta Arachnida Pentastomida Order: Acarina Family: Linguatulidae Flies, Lice, ( Ticks , mites, ( Tongue worms) fleas, bugs etc. spider & scorpions) Phylum: Arthropoda CLASSIFICATION: Phylum: Arthropoda Classes Insecta Arachnida Pentastomida Subclasses: Apterygota (Generallyo C wingless insects) and Pterygota Subclasse: Pterygota Divisions Exoterygota Endopterygota Order: (1) Mallophaga (biting lice) Order: (1) Diptera ( true flies) (2) Siphunculata/Anoplura (sucking lice) (2) Siphonaptera ( fleas) (3) Hemiptera (bugs) (3) Coleoptera (beetles) (4) Odonata( dragon flies) (5) Orthoptera ( cockroaches, (4) Hymenoptera (bees, wasps, grasshoppers) ants) Class: Arachnida Phylum: Arthropoda Class Insecta Arachnida Pentastomida Sub-class: Acari Family: Linguatulidae (Acarina) ( Tongue worm) ORDER Parasitiformes Acariformes Sub-order Sub-order Ixodida Gamasida Actinedida Acaridida Oribatida ( metastigmata) ( Mesostignmata) (Prostigmagta) ( Astigmata) ( Cryptostigmata) TICKS Family: Trombiculidae Family: Demodicidae Genus: Trombicula Genus: Demodex Family: Dermanyssidae Genus: Demanyssus Family: Psoroptidae Family: Sarcoptidae Family: Genus: Psoroptes, Genus: Sarcoptes, Knemidocoptidae Chorioptes, Notoedres Genus: Knemidocoptes Otodectes Mites Phylum: Arthropoda Class Arachnida Sub-class: Acari (Acarina) ORDER Parasitiformes Acariformes -

Review Article Potential of Traditional Knowledge of Plants in the Management of Arthropods in Livestock Industry with Focus on (Acari) Ticks
Hindawi Evidence-Based Complementary and Alternative Medicine Volume 2017, Article ID 8647919, 33 pages https://doi.org/10.1155/2017/8647919 Review Article Potential of Traditional Knowledge of Plants in the Management of Arthropods in Livestock Industry with Focus on (Acari) Ticks Wycliffe Wanzala1,2 1 Department of Biological Sciences, School of Science and Information Sciences, Maasai Mara University, P.O.Box861-20500,Narok,Kenya 2Behavioural and Chemical Ecology Department, International Centre of Insect Physiology and Ecology, African Insect Science for Food and Health, P.O. Box 30772-00100-GPO, Nairobi, Kenya Correspondence should be addressed to Wycliffe Wanzala; [email protected] Received 19 December 2016; Accepted 11 May 2017; Published 17 July 2017 Academic Editor: Jose´ L. Rios Copyright © 2017 Wycliffe Wanzala. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Antitick plants and related ethnoknowledge/ethnopractices with potential for integrated tick control and management strategies to improve livestock production are reviewed. About 231 plants reviewed showed a variety of bioactive properties, namely, being toxic, repellent, antifeedant, and antiovipositant and ability to immobilize target tick species. These ethnobotanical substances are potentially useful in developing sustainable, efficient, and effective antitick agents suitable for rural livestock farmers. -
Mites and Endosymbionts – Towards Improved Biological Control
Mites and endosymbionts – towards improved biological control Thèse de doctorat présentée par Renate Zindel Université de Neuchâtel, Suisse, 16.12.2012 Cover photo: Hypoaspis miles (Stratiolaelaps scimitus) • FACULTE DES SCIENCES • Secrétariat-Décanat de la faculté U11 Rue Emile-Argand 11 CH-2000 NeuchAtel UNIVERSIT~ DE NEUCHÂTEL IMPRIMATUR POUR LA THESE Mites and endosymbionts- towards improved biological control Renate ZINDEL UNIVERSITE DE NEUCHATEL FACULTE DES SCIENCES La Faculté des sciences de l'Université de Neuchâtel autorise l'impression de la présente thèse sur le rapport des membres du jury: Prof. Ted Turlings, Université de Neuchâtel, directeur de thèse Dr Alexandre Aebi (co-directeur de thèse), Université de Neuchâtel Prof. Pilar Junier (Université de Neuchâtel) Prof. Christoph Vorburger (ETH Zürich, EAWAG, Dübendorf) Le doyen Prof. Peter Kropf Neuchâtel, le 18 décembre 2012 Téléphone : +41 32 718 21 00 E-mail : [email protected] www.unine.ch/sciences Index Foreword ..................................................................................................................................... 1 Summary ..................................................................................................................................... 3 Zusammenfassung ........................................................................................................................ 5 Résumé ....................................................................................................................................... -

Course Syllabus for Diploma in Animal Husbandry
COURSE SYLLABUS FOR DIPLOMA IN ANIMAL HUSBANDRY KAMDHENU UNIVERSITY GANDHINAGAR 2014 1 SEMESTER WISE COURSE DISTRIBUTION (Total duration Three years) First Semester Sr. no Course No. Title of the Course Credit 1. LAN-111 Introductory Livestock Anatomy 3+1=4 2. APHY-111 Introductory Animal Physiology 3+1=4 3. LPM-111 Introductory Animal Management-I 2+1=3 4. ENG-111 English 2+1=3 5. CA-111 Introduction to Computer Application 1+2=3 Total 11+6=17 Second Semester Sr. no Course No. Title of the Course Credit 1. STAT-121 Elementary Statistics 2+1=3 2. AN-121 Introductory Fodder Management and grassland 1+1=2 Management 3. AB-121 Introductory Animal Breeding 1+1=2 4. LPM-121 Introductory Animal Management-II 2+1=3 5. AHE-121 Introductory Animal Husbandry Extension-I 2+1=3 6. ENVS-121 Introduction to Environmental Science 2+1=3 Total 10+6=16 Third Semester Sr. no Course No. Title of the Course Credit 1. VMI-211 Introductory Veterinary Microbiology 2+1=3 2. VPARA-211 Introductory Veterinary Parasitology 2+1=3 3. VPA-211 Preliminary Pathology 2+1=3 4. AHE-211 Introductory Animal Husbandry Extension-II 2+1=3 5. AN-211 Introductory Animal Nutrition-I 1+1=2 Total 9+5=14 Fourth Semester Sr. no Course No. Title of the Course Credit 1. AHEM-221 Introductory Animal Husbandry Economics and 2+0=2 Marketing 2. AN-222 Introductory Animal Nutrition-II 1+1=2 3. VP-221 Introductory Pharmacology 3+2=5 4. AR-221 Introductory Animal Reproductions-I 1+2=3 5.