New York State Newborn Screening Panel
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

In the Prevention of Occupational Diseases 94 7.1 Introduction
Report on the current situation in relation to occupational diseases' systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects ‘Report on the current situation in relation to occupational diseases’ systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects’ Table of Contents 1 Introduction 4 1.1 Foreword .................................................................................................... 4 1.2 The burden of occupational diseases ......................................................... 4 1.3 Recommendation 2003/670/EC .................................................................. 6 1.4 The EU context .......................................................................................... 9 1.5 Information notices on occupational diseases, a guide to diagnosis .................................................................................................. 11 1.6 Objectives of the project ........................................................................... 11 1.7 Methodology and sources ........................................................................ 12 1.8 Structure of the report .............................................................................. 15 2 Developments -

A Retrospective Chart Review Examining the Clinical Utility of Family Health History
Sarah Lawrence College DigitalCommons@SarahLawrence The Joan H. Marks Graduate Program in Human Genetics Theses Human Genetics 5-2017 A Retrospective Chart Review Examining the Clinical Utility of Family Health History Katherine Dao Sarah Lawrence College Julia Russo Sarah Lawrence College Follow this and additional works at: https://digitalcommons.slc.edu/genetics_etd Part of the Genetics Commons Recommended Citation Dao, Katherine and Russo, Julia, "A Retrospective Chart Review Examining the Clinical Utility of Family Health History" (2017). Human Genetics Theses. 33. https://digitalcommons.slc.edu/genetics_etd/33 This Thesis - Open Access is brought to you for free and open access by the The Joan H. Marks Graduate Program in Human Genetics at DigitalCommons@SarahLawrence. It has been accepted for inclusion in Human Genetics Theses by an authorized administrator of DigitalCommons@SarahLawrence. For more information, please contact [email protected]. Katherine Dao and Julia Russo A Retrospective Chart Review Examining the Clinical Utility of Family Health History Authors: Katherine Dao, Julia Russo, Jennifer L. Garbarini, Sheila C. Johal, Shannon Wieloch Submitted in partial completion of the Master of Science Degree at Sarah Lawrence College, May 2017 1/34 Katherine Dao and Julia Russo Abstract Family health history (FHH) is a simple and cost-effective clinical tool widely used by genetic professionals. Although the value of FHH for assessing personal and familial health and reproductive risk within a prenatal population has been demonstrated in past studies, its utility within a genetic carrier screening population has not been evaluated. The purpose of this study was to examine the utility of FHH as a clinical screening tool and explore the general outcomes of full FHH evaluations within an expanded carrier screening (ECS) population. -

European Conference on Rare Diseases
EUROPEAN CONFERENCE ON RARE DISEASES Luxembourg 21-22 June 2005 EUROPEAN CONFERENCE ON RARE DISEASES Copyright 2005 © Eurordis For more information: www.eurordis.org Webcast of the conference and abstracts: www.rare-luxembourg2005.org TABLE OF CONTENT_3 ------------------------------------------------- ACKNOWLEDGEMENTS AND CREDITS A specialised clinic for Rare Diseases : the RD TABLE OF CONTENTS Outpatient’s Clinic (RDOC) in Italy …………… 48 ------------------------------------------------- ------------------------------------------------- 4 / RARE, BUT EXISTING The organisers particularly wish to thank ACKNOWLEDGEMENTS AND CREDITS 4.1 No code, no name, no existence …………… 49 ------------------------------------------------- the following persons/organisations/companies 4.2 Why do we need to code rare diseases? … 50 PROGRAMME COMMITTEE for their role : ------------------------------------------------- Members of the Programme Committee ……… 6 5 / RESEARCH AND CARE Conference Programme …………………………… 7 …… HER ROYAL HIGHNESS THE GRAND DUCHESS OF LUXEMBOURG Key features of the conference …………………… 12 5.1 Research for Rare Diseases in the EU 54 • Participants ……………………………………… 12 5.2 Fighting the fragmentation of research …… 55 A multi-disciplinary approach ………………… 55 THE EUROPEAN COMMISSION Funding of the conference ……………………… 14 Transfer of academic research towards • ------------------------------------------------- industrial development ………………………… 60 THE GOVERNEMENT OF LUXEMBOURG Speakers ……………………………………………… 16 Strengthening cooperation between academia -
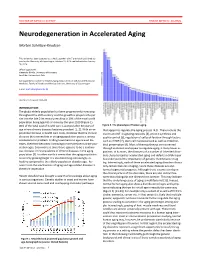
Neurodegeneration in Accelerated Aging
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -
National System for Recording and Notification of Occupational Diseases Practical Guide
InternationalInternational LabourLabour OfficeOffice GenevaGeneva National System for Recording and Notification of Occupational Diseases Practical guide Programme on Safety and Health at Work and the Environment (SafeWork) International Labour Organization Route des Morillons 4 CH -1211 Geneva 22 Switzerland TEL. + 41 22 7996715 FAX + 41 22 7996878 E-mail : safework @ ilo.org www.ilo.org / safework ILO National System for Recording and Notification of Occupational Diseases – Practical guide ISBN 978-92-2-127057-7 9 789221 270577 Programme on Safety and Health at Work and the Environment (SafeWork) National System for Recording and Notification of Occupational Diseases Practical guide International Labour Office, Geneva Copyright © International Labour Organization 2013 First published 2013 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Never- theless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. -

Regulations for Disease Reporting and Control
Department of Health Regulations for Disease Reporting and Control Commonwealth of Virginia State Board of Health October 2016 Virginia Department of Health Office of Epidemiology 109 Governor Street P.O. Box 2448 Richmond, VA 23218 Department of Health Department of Health TABLE OF CONTENTS Part I. DEFINITIONS ......................................................................................................................... 1 12 VAC 5-90-10. Definitions ............................................................................................. 1 Part II. GENERAL INFORMATION ............................................................................................... 8 12 VAC 5-90-20. Authority ............................................................................................... 8 12 VAC 5-90-30. Purpose .................................................................................................. 8 12 VAC 5-90-40. Administration ....................................................................................... 8 12 VAC 5-90-70. Powers and Procedures of Chapter Not Exclusive ................................ 9 Part III. REPORTING OF DISEASE ............................................................................................. 10 12 VAC 5-90-80. Reportable Disease List ....................................................................... 10 A. Reportable disease list ......................................................................................... 10 B. Conditions reportable by directors of -

“List of Occupational Diseases” Annexed to the List of Occupational Diseases Recommendation, 2002 (No
MEULOD/2005/1 INTERNATIONAL LABOUR ORGANIZATION Report on the replies to the questionnaire on the updating of the “list of occupational diseases” annexed to the List of Occupational Diseases Recommendation, 2002 (No. 194) and on the amendments to the list of occupational diseases submitted to the Committee on Occupational Accidents and Diseases of the 90th Session of the International Labour Conference in 2002 Working document for the Meeting of Experts on updating the List of Occupational Diseases (Geneva, 13-20 December 2005) InFocus Programme on Safety and Health at Work and the Environment (SafeWork) Geneva, October 2005 INTERNATIONAL LABOUR OFFICE GENEVA MEULOD/2005/1 INTERNATIONAL LABOUR ORGANIZATION Report on the replies to the questionnaire on the updating of the “list of occupational diseases” annexed to the List of Occupational Diseases Recommendation, 2002 (No. 194) and on the amendments to the list of occupational diseases submitted to the Committee on Occupational Accidents and Diseases of the 90th Session of the International Labour Conference in 2002 Working document for the Meeting of Experts on updating the List of Occupational Diseases (Geneva, 13-20 December 2005) InFocus Programme on Safety and Health at Work and the Environment (SafeWork) Geneva, October 2005 INTERNATIONAL LABOUR OFFICE GENEVA Copyright © International Labour Organization 2005 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to the Publications Bureau (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland. -

LIST of OCCUPATIONAL DISEASES (Revised 2010)
LIST OF OCCUPATIONAL DISEASES (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Occupational Safety and Health Series, No. 74 List of occupational diseases (revised 2010) Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases INTERNATIONAL LABOUR OFFICE • GENEVA Copyright © International Labour Organization 2010 First published 2010 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: pubdroit@ ilo.org. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. ILO List of occupational diseases (revised 2010). Identification and recognition of occupational diseases: Criteria for incorporating diseases in the ILO list of occupational diseases Geneva, International Labour Office, 2010 (Occupational Safety and Health Series, No. 74) occupational disease / definition. 13.04.3 ISBN 978-92-2-123795-2 ISSN 0078-3129 Also available in French: Liste des maladies professionnelles (révisée en 2010): Identification et reconnaissance des maladies professionnelles: critères pour incorporer des maladies dans la liste des maladies professionnelles de l’OIT (ISBN 978-92-2-223795-1, ISSN 0250-412x), Geneva, 2010, and in Spanish: Lista de enfermedades profesionales (revisada en 2010). -

ICD-10 International Statistical Classification of Diseases and Related Health Problems
ICD-10 International Statistical Classification of Diseases and Related Health Problems 10th Revision Volume 2 Instruction manual 2010 Edition WHO Library Cataloguing-in-Publication Data International statistical classification of diseases and related health problems. - 10th revision, edition 2010. 3 v. Contents: v. 1. Tabular list – v. 2. Instruction manual – v. 3. Alphabetical index. 1.Diseases - classification. 2.Classification. 3.Manuals. I.World Health Organization. II.ICD-10. ISBN 978 92 4 154834 2 (NLM classification: WB 15) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

FAQ REGARDING DISEASE REPORTING in MONTANA | Rev
Disease Reporting in Montana: Frequently Asked Questions Title 50 Section 1-202 of the Montana Code Annotated (MCA) outlines the general powers and duties of the Montana Department of Public Health & Human Services (DPHHS). The three primary duties that serve as the foundation for disease reporting in Montana state that DPHHS shall: • Study conditions affecting the citizens of the state by making use of birth, death, and sickness records; • Make investigations, disseminate information, and make recommendations for control of diseases and improvement of public health to persons, groups, or the public; and • Adopt and enforce rules regarding the reporting and control of communicable diseases. In order to meet these obligations, DPHHS works closely with local health jurisdictions to collect and analyze disease reports. Although anyone may report a case of communicable disease, such reports are submitted primarily by health care providers and laboratories. The Administrative Rules of Montana (ARM), Title 37, Chapter 114, Communicable Disease Control, outline the rules for communicable disease control, including disease reporting. Communicable disease surveillance is defined as the ongoing collection, analysis, interpretation, and dissemination of disease data. Accurate and timely disease reporting is the foundation of an effective surveillance program, which is key to applying effective public health interventions to mitigate the impact of disease. What diseases are reportable? A list of reportable diseases is maintained in ARM 37.114.203. The list continues to evolve and is consistent with the Council of State and Territorial Epidemiologists (CSTE) list of Nationally Notifiable Diseases maintained by the Centers for Disease Control and Prevention (CDC). In addition to the named conditions on the list, any occurrence of a case/cases of communicable disease in the 20th edition of the Control of Communicable Diseases Manual with a frequency in excess of normal expectancy or any unusual incident of unexplained illness or death in a human or animal should be reported. -

ICD-10 International Statistical Classification of Diseases And
ICD-10 International statistical classification of diseases and related health problems 10th revision Volume 2 Instruction manual Fifth edition 2016 Volume 2.indb 1 11/09/15 10:46 WHO Library Cataloguing-in-Publication Data International statistical classification of diseases and related health problems. - 10th revision, Fifth edition, 2016. 3 v. Contents: v. 1. Tabular list -- v. 2. Instruction manual -- v. 3. Alphabetical index. 1.Diseases - classification. 2.Classification. 3.Manuals. I.World Health Organization. II.ICD-10. ISBN 978 92 4 154916 5 (NLM classification: WB 15) © World Health Organization 2011. Reprinted in 2015. All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned.