Triplet Repeat Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Brief Evaluation and Image Formation of Pediatrics Nutritional Forum in Opinion Sector Disouja Wills* Nutritonal Sciences, Christian Universita Degli Studo, Italy
d Pediatr Wills, Matern Pediatr Nutr 2016, 2:2 an ic l N a u n t DOI: 10.4172/2472-1182.1000113 r r e i t t i o Maternal and Pediatric a n M ISSN: 2472-1182 Nutrition ShortResearch Commentary Article OpenOpen Access Access A Brief Evaluation and Image formation of Pediatrics Nutritional Forum in Opinion Sector Disouja Wills* Nutritonal Sciences, Christian Universita degli studo, Italy Abstract Severe most and one of the main global threat is Nutritional disorders to backward countries, with respect to this issue WHO involved and trying to overcome this issue with the Co-ordination of INF and BNF. International Nutrition Foundation and British Nutrition Foundation, development in weight gain through proper nutrition and proper immune mechanism in the kids is their main role to eradicate and overcome nutritional problems in world. Keywords: INF; BNF; Malnutrition; Merasmus; Rickets; Weight loss; Precautions to Avoid Nutrition Deficiency in Paediatric health issue Paediatrics Introduction Respective disease having respective deficiency dis order but in the case of nutritional diseases. Proper nutrition is the only thing to cure In the mankind a respective one health and weight gain is fully nutritional disorders. Providing sufficient diet like fish, meat, egg, milk based on perfect nutritional intake which he is having daily, poor diet to malnourished kids and consuming beef, fish liver oil, sheep meat, will show the improper impact and injury to the some of the systems boiled eggs from the age of 3 itself (Tables 1 and 2). in the body, total health also in some times. Blindness, Scurvy, Rickets will be caused by nutritional deficiency disorders only, mainly in kids. -

Neonatal Orthopaedics
NEONATAL ORTHOPAEDICS NEONATAL ORTHOPAEDICS Second Edition N De Mazumder MBBS MS Ex-Professor and Head Department of Orthopaedics Ramakrishna Mission Seva Pratishthan Vivekananda Institute of Medical Sciences Kolkata, West Bengal, India Visiting Surgeon Department of Orthopaedics Chittaranjan Sishu Sadan Kolkata, West Bengal, India Ex-President West Bengal Orthopaedic Association (A Chapter of Indian Orthopaedic Association) Kolkata, West Bengal, India Consultant Orthopaedic Surgeon Park Children’s Centre Kolkata, West Bengal, India Foreword AK Das ® JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTD. New Delhi • London • Philadelphia • Panama (021)66485438 66485457 www.ketabpezeshki.com ® Jaypee Brothers Medical Publishers (P) Ltd. Headquarters Jaypee Brothers Medical Publishers (P) Ltd. 4838/24, Ansari Road, Daryaganj New Delhi 110 002, India Phone: +91-11-43574357 Fax: +91-11-43574314 Email: [email protected] Overseas Offices J.P. Medical Ltd. Jaypee-Highlights Medical Publishers Inc. Jaypee Brothers Medical Publishers Ltd. 83, Victoria Street, London City of Knowledge, Bld. 237, Clayton The Bourse SW1H 0HW (UK) Panama City, Panama 111, South Independence Mall East Phone: +44-2031708910 Phone: +507-301-0496 Suite 835, Philadelphia, PA 19106, USA Fax: +02-03-0086180 Fax: +507-301-0499 Phone: +267-519-9789 Email: [email protected] Email: [email protected] Email: [email protected] Jaypee Brothers Medical Publishers (P) Ltd. Jaypee Brothers Medical Publishers (P) Ltd. 17/1-B, Babar Road, Block-B, Shaymali Shorakhute, Kathmandu Mohammadpur, Dhaka-1207 Nepal Bangladesh Phone: +00977-9841528578 Mobile: +08801912003485 Email: [email protected] Email: [email protected] Website: www.jaypeebrothers.com Website: www.jaypeedigital.com © 2013, Jaypee Brothers Medical Publishers All rights reserved. No part of this book may be reproduced in any form or by any means without the prior permission of the publisher. -

Type II Familial Synpolydactyly: Report on Two Families with an Emphasis on Variations of Expression
European Journal of Human Genetics (2011) 19, 112–114 & 2011 Macmillan Publishers Limited All rights reserved 1018-4813/11 www.nature.com/ejhg SHORT REPORT Type II familial synpolydactyly: report on two families with an emphasis on variations of expression Mohammad M Al-Qattan*,1 Type II familial synpolydactyly is rare and is known to have variable expression. However, no previous papers have attempted to review these variations. The aim of this paper was to review these variations and show several of these variable expressions in two families. The classic features of type II familial synpolydactyly are bilateral synpolydactyly of the third web spaces of the hands and bilateral synpolydactyly of the fourth web spaces of the feet. Several members of the two families reported in this paper showed the following variations: the third web spaces of the hands showing syndactyly without the polydactyly, normal feet, concurrent polydactyly of the little finger, concurrent clinodactyly of the little finger and the ‘homozygous’ phenotype. It was concluded that variable expressions of type II familial synpolydactyly are common and awareness of such variations is important to clinicians. European Journal of Human Genetics (2011) 19, 112–114; doi:10.1038/ejhg.2010.127; published online 18 August 2010 Keywords: type II familial syndactyly; inherited synpolydactyly; variations of expression INTRODUCTION CASE REPORTS Type II familial synpolydactyly is rare and it has been reported in o30 The first family families.1–12 It is characterized by bilateral synpolydactyly of the third The family had a history of synpolydactyly type II for several web spaces of the hands and bilateral synpolydactyly of the fourth web generations on the mother’s side (Table 1). -

The Genetic Basis for Skeletal Diseases
insight review articles The genetic basis for skeletal diseases Elazar Zelzer & Bjorn R. Olsen Harvard Medical School, Department of Cell Biology, 240 Longwood Avenue, Boston, Massachusetts 02115, USA (e-mail: [email protected]) We walk, run, work and play, paying little attention to our bones, their joints and their muscle connections, because the system works. Evolution has refined robust genetic mechanisms for skeletal development and growth that are able to direct the formation of a complex, yet wonderfully adaptable organ system. How is it done? Recent studies of rare genetic diseases have identified many of the critical transcription factors and signalling pathways specifying the normal development of bones, confirming the wisdom of William Harvey when he said: “nature is nowhere accustomed more openly to display her secret mysteries than in cases where she shows traces of her workings apart from the beaten path”. enetic studies of diseases that affect skeletal differentiation to cartilage cells (chondrocytes) or bone cells development and growth are providing (osteoblasts) within the condensations. Subsequent growth invaluable insights into the roles not only of during the organogenesis phase generates cartilage models individual genes, but also of entire (anlagen) of future bones (as in limb bones) or membranous developmental pathways. Different mutations bones (as in the cranial vault) (Fig. 1). The cartilage anlagen Gin the same gene may result in a range of abnormalities, are replaced by bone and marrow in a process called endo- and disease ‘families’ are frequently caused by mutations in chondral ossification. Finally, a process of growth and components of the same pathway. -

Genetics of Congenital Hand Anomalies
G. C. Schwabe1 S. Mundlos2 Genetics of Congenital Hand Anomalies Die Genetik angeborener Handfehlbildungen Original Article Abstract Zusammenfassung Congenital limb malformations exhibit a wide spectrum of phe- Angeborene Handfehlbildungen sind durch ein breites Spektrum notypic manifestations and may occur as an isolated malforma- an phänotypischen Manifestationen gekennzeichnet. Sie treten tion and as part of a syndrome. They are individually rare, but als isolierte Malformation oder als Teil verschiedener Syndrome due to their overall frequency and severity they are of clinical auf. Die einzelnen Formen kongenitaler Handfehlbildungen sind relevance. In recent years, increasing knowledge of the molecu- selten, besitzen aber aufgrund ihrer Häufigkeit insgesamt und lar basis of embryonic development has significantly enhanced der hohen Belastung für Betroffene erhebliche klinische Rele- our understanding of congenital limb malformations. In addi- vanz. Die fortschreitende Erkenntnis über die molekularen Me- tion, genetic studies have revealed the molecular basis of an in- chanismen der Embryonalentwicklung haben in den letzten Jah- creasing number of conditions with primary or secondary limb ren wesentlich dazu beigetragen, die genetischen Ursachen kon- involvement. The molecular findings have led to a regrouping of genitaler Malformationen besser zu verstehen. Der hohe Grad an malformations in genetic terms. However, the establishment of phänotypischer Variabilität kongenitaler Handfehlbildungen er- precise genotype-phenotype correlations for limb malforma- schwert jedoch eine Etablierung präziser Genotyp-Phänotyp- tions is difficult due to the high degree of phenotypic variability. Korrelationen. In diesem Übersichtsartikel präsentieren wir das We present an overview of congenital limb malformations based Spektrum kongenitaler Malformationen, basierend auf einer ent- 85 on an anatomic and genetic concept reflecting recent molecular wicklungsbiologischen, anatomischen und genetischen Klassifi- and developmental insights. -

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

Angeborene Fehlbildungen Der Extremitäten
Aus der Klinik für Orthopädie (Direktor: Prof. Dr. med. J. Hassenpflug) der Medizinischen Fakultät der Christian-Albrechts-Universität zu Kiel Die angeborenen Fehlbildungen der oberen und unteren Extremitäten in der Orthopädischen Universitätsklinik Kiel von 1974-2001 Inauguraldissertation zur Erlangung der Doktorwürde vorgelegt von Karsten Naused aus Wolfenbüttel Kiel 2014 1. Berichterstatter: Prof. Dr. J. Hassenpflug, Klinik für Orthopädie 2. Berichterstatter: Prof. Dr. M. Schrappe, Klinik für Allgemeine Pädiatrie Tag der mündlichen Prüfung: 12.06.2014 Zum Druck genehmigt, Kiel, den 12.06.2014 gez.: PD Dr. S. Lippross, Klinik Unfallchirurgie (Prüfer) Prof. Dr. A. Seekamp, Klinik Unfallchirurgie (Beisitzer) Prof. Dr. Johann Roider, Vorsitzender des Ausschusses für Promotion Inhaltsverzeichnis 1. Einleitung Seite 1.1 Vorbemerkung.................................................................................................1 1.2 Historisches.....................................................................................................2 1.3 Embryologie.....................................................................................................3 1.4 Ätiologie und Pathogenese..............................................................................6 2. Patientengut und Methode 2.1 Quellen der Patientendaten...........................................................................10 2.2 Dokumentation der Daten..............................................................................12 2.3 Datenabfrage.................................................................................................13 -

In the Prevention of Occupational Diseases 94 7.1 Introduction
Report on the current situation in relation to occupational diseases' systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects ‘Report on the current situation in relation to occupational diseases’ systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects’ Table of Contents 1 Introduction 4 1.1 Foreword .................................................................................................... 4 1.2 The burden of occupational diseases ......................................................... 4 1.3 Recommendation 2003/670/EC .................................................................. 6 1.4 The EU context .......................................................................................... 9 1.5 Information notices on occupational diseases, a guide to diagnosis .................................................................................................. 11 1.6 Objectives of the project ........................................................................... 11 1.7 Methodology and sources ........................................................................ 12 1.8 Structure of the report .............................................................................. 15 2 Developments -

European Conference on Rare Diseases
EUROPEAN CONFERENCE ON RARE DISEASES Luxembourg 21-22 June 2005 EUROPEAN CONFERENCE ON RARE DISEASES Copyright 2005 © Eurordis For more information: www.eurordis.org Webcast of the conference and abstracts: www.rare-luxembourg2005.org TABLE OF CONTENT_3 ------------------------------------------------- ACKNOWLEDGEMENTS AND CREDITS A specialised clinic for Rare Diseases : the RD TABLE OF CONTENTS Outpatient’s Clinic (RDOC) in Italy …………… 48 ------------------------------------------------- ------------------------------------------------- 4 / RARE, BUT EXISTING The organisers particularly wish to thank ACKNOWLEDGEMENTS AND CREDITS 4.1 No code, no name, no existence …………… 49 ------------------------------------------------- the following persons/organisations/companies 4.2 Why do we need to code rare diseases? … 50 PROGRAMME COMMITTEE for their role : ------------------------------------------------- Members of the Programme Committee ……… 6 5 / RESEARCH AND CARE Conference Programme …………………………… 7 …… HER ROYAL HIGHNESS THE GRAND DUCHESS OF LUXEMBOURG Key features of the conference …………………… 12 5.1 Research for Rare Diseases in the EU 54 • Participants ……………………………………… 12 5.2 Fighting the fragmentation of research …… 55 A multi-disciplinary approach ………………… 55 THE EUROPEAN COMMISSION Funding of the conference ……………………… 14 Transfer of academic research towards • ------------------------------------------------- industrial development ………………………… 60 THE GOVERNEMENT OF LUXEMBOURG Speakers ……………………………………………… 16 Strengthening cooperation between academia -
Neurodegeneration in Accelerated Aging
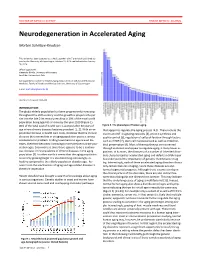
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

The Myotonic Dystrophies: Diagnosis and Management Chris Turner,1 David Hilton-Jones2
Review J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2008.158261 on 22 February 2010. Downloaded from The myotonic dystrophies: diagnosis and management Chris Turner,1 David Hilton-Jones2 1Department of Neurology, ABSTRACT asymptomatic relatives as well as prenatal and National Hospital for Neurology There are currently two clinically and molecularly defined preimplantation diagnosis can also be performed.7 and Neurosurgery, London, UK 2Department of Clinical forms of myotonic dystrophy: (1) myotonic dystrophy Neurology, The Radcliffe type 1 (DM1), also known as ‘Steinert’s disease’; and Anticipation Infirmary, Oxford, UK (2) myotonic dystrophy type 2 (DM2), also known as DMPK alleles greater than 37 CTG repeats in length proximal myotonic myopathy. DM1 and DM2 are are unstable and may expand in length during meiosis Correspondence to progressive multisystem genetic disorders with several and mitosis. Children of a parent with DM1 may Dr C Turner, Department of Neurology, National Hospital for clinical and genetic features in common. DM1 is the most inherit repeat lengths considerably longer than those Neurology and Neurosurgery, common form of adult onset muscular dystrophy whereas present in the transmitting parent. This phenomenon Queen Square, London WC1N DM2 tends to have a milder phenotype with later onset of causes ‘anticipation’, which is the occurrence of 3BG, UK; symptoms and is rarer than DM1. This review will focus increasing disease severity and decreasing age of onset [email protected] on the clinical features, diagnosis and management of in successive generations. The presence of a larger Received 1 December 2008 DM1 and DM2 and will briefly discuss the recent repeat leads to earlier onset and more severe disease Accepted 18 December 2008 advances in the understanding of the molecular and causes the more severe phenotype of ‘congenital’ pathogenesis of these diseases with particular reference DM1 (figure 2).8 9 A child with congenital DM 1 to new treatments using gene therapy. -

Diseases Transmitted Through the Food Supply
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention Diseases Transmitted through the Food Supply AGENCY: Centers for Disease Control and Prevention (CDC), Department of Health and Human Services (HHS). ACTION: Notice of annual update of list of infectious and communicable diseases that are transmitted through handling the food supply and the methods by which such diseases are transmitted. SUMMARY: Section 103 (d) of the Americans with Disabilities Act of 1990, Public Law 101–336, requires the Secretary to publish a list of infectious and communicable diseases that are transmitted through handling the food supply and to review and update the list annually. The Centers for Disease Control and Prevention (CDC) published a final list on August 16, 1991 (56 FR40897) and updates on September 8, 1992 (57 FR 40917); January 13, 1994 (59 FR 1949); August 15, 1996 (61 FR 42426); September 22, 1997 (62 FR 49518–9); September 15, 1998 (63 FR 49359); September 21, 1999 (64 FR 51127); September 27, 2000 (65 FR 58088); September 10, 2001 (66 FR 47030); September 27, 2002 (67 FR 61109); September 26, 2006 (71 FR 56152); November 17, 2008 (73 FR 67871); and November 29, 2009 (74 FR 61151). The final list has been reviewed in light of new information and has been revised as set forth below. DATES: Effective Date: January 31, 2014. FOR FURTHER INFORMATION CONTACT: Dr. Art Liang, Division of Foodborne Waterborne and Environment Diseases, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention (CDC), 1600 Clifton Road, NE., Mailstop G–24, Atlanta, Georgia 30333.