Sub National Mortality Trajectory in Kenya: Examining the Role of HIV and AIDS Interventions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Western HIV/AIDS Network (WEHAK) to Participate in Strengthening
WESTERN HIV AIDS NETWORK HQ Responding to MCSP, HIV- SRHR & Malaria Telephone: +254-0729-080-676 Based 200m after Bridge Inter. Academy Kakamega Office mobile: +254-0733-648400 P. O. BOX 1443 - 50100 Kakamega Kenya East Africa http://www.westernhivaidsnetwork.ac.ke : “RESPONSE TO: MCSP, HIV-CANCER, ASTHMA, MALARIA & NEG.DISEASES” Date: April 15th. 2017. CONNECTING WITH (GHSP) - GLOBAL HEALTH SERVICE PARTNERSHIP , PEACE CORPS, PEPFAR & SEED. Western HIV/AIDS Network (WEHAK) to participate in Strengthening Medical and Nursing Education Supported by PEACE CORPS, PEPFAR, SEED & “Global Health Service Partnership” (GHSP). Email: [email protected] Standing still won’t stop #measles or get us to How Partnerships, Innovation, Entrepreneurships & amp: Technical are empowering today’s Youth Website: http://wwwt.co/QWgWGPWSKXvia@dolcigelati#socialgood Email: [email protected] Email:[email protected] Email: [email protected] Email: trib.al/[email protected] Email:[email protected] Email:[email protected] Email:[email protected] Dear Madam, RE: WESTERN HIV/AIDS NETWORK’S REQUEST FOR FUNDS FROM OFFICE OF THE GOVERNOR:- Western HIV/AIDS Network appreciates your letter of December 31st.2015, the letter serves as your confirmation of our organization’s collaborative request. Thank you for joining us in efforts of improving Global Health to save lives of mothers and their Children – MCSP- Maternal and Child Survival Program., HIV- CANCER, ASTHMA, SRHR, MALARIA & THE MOST NEGLECTED TROPICAL .DISEASES” and Training the next generation of doctors and nurses. Western HIV/AIDS Network (WEHAK) is also currently committed to HIV/AIDS Prevention, Treatment, Care and Support Initiative (The Youth, Women, MARPs –Most at Risk Persons, People Living with AIDS) The Network will continue responding to both the HIV/AIDS infected and affected persons to achieve HIV-zero New Infections in Kenya by the end of year 2017. -

Kenya Country Office
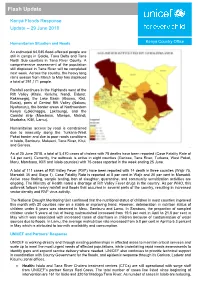
Kenya Country Office Flood Situation Report Report # 1: 24 November 2019 Highlights Situation in Numbers The National Disaster Operations Center (NDOC) estimates that at least 330,000 330,000 people are affected - 18,000 people have been displaced and 120 people affected people have died due to floods and landslides. (NDOC-24/11/2019) A total of 6,821 children have been reached through integrated outreach 31 services and 856 people have received cholera treatment through UNICEF-supported treatment centres. counties affected by flooding (NDOC-24/11/2019) A total of 270 households in Turkana County (out of 400 targeted) and 110 households in Wajir county have received UNICEF family emergency kits 120 (including 20-litre and 10-litre bucket), soap and water treatment tablets people killed from flooding through partnership with the Kenya Red Cross. (NDOC-24/11/2019) UNICEF has reached 55,000 people with WASH supplies consisting of 20- litre jerrycans, 10-litre buckets and multipurpose bar soap. 18,000 UNICEF has completed solarization of two boreholes reaching people displaced approximately 20,500 people with access to safe water in Garissa County. (NDOC-24/11/2019) Situation Overview & Humanitarian Needs Kenya has continued to experience enhanced rainfall resulting in flooding since mid-October, negatively impacting the lives and livelihoods of vulnerable populations. According to the National Disaster Operations Center (NDOC) 24 November 2019 updates, major roads have been cut off in 11 counties, affecting accessibility to affected populations for rapid assessments and delivery of humanitarian assistance, especially in parts of West Pokot, Marsabit, Mandera, Turkana, Garissa, Lamu, Mombasa, Tana River, Taita Taveta, Kwale and Wajir Counties. -
Kenya's Somali North East: Devolution and Security
Kenya’s Somali North East: Devolution and Security Crisis Group Africa Briefing N°114 Nairobi/Brussels, 17 November 2015 I. Overview Devolved government in Kenya’s newly formed north-eastern counties, designed to address decades of political marginalisation and underdevelopment, has been un- dermined by dominant clans monopolising power and growing corruption. Violent clan competition and antipathy between elected county elites and the remaining national administrative structures have allowed the violently extremist Al-Shabaab movement to expand and operate with relative impunity across large areas of the North East. Its attacks exposed security-service disarray and caused a sharp reversal of already stretched state services in this vast and poor region that shares a porous 680km border with Somalia. To end the violence and capitalise on devolution’s potential, county elites must be more inclusive of minorities, cooperate across local boundaries for inter-county peace and recognise the continued role for neutral nation- al institutions. National government should recognise where pragmatism can trump convention and back new security approaches that combine national and county responses. Rampant criminality, inter-clan animosities and small-arms proliferation stretch policing and render highly insecure the sprawling refugee camps that host more than 350,000 Somali nationals fleeing the conflict in their country. This is compounded by Al-Shabaab infiltration, radicalisation and recruitment – especially in a border- land region where the -
Flash Update
Flash Update Kenya Floods Response Update – 29 June 2018 Humanitarian Situation and Needs Kenya Country Office An estimated 64,045 flood-affected people are still in camps in Galole, Tana Delta and Tana North Sub counties in Tana River County. A comprehensive assessment of the population still displaced in Tana River will be completed next week. Across the country, the heavy long rains season from March to May has displaced a total of 291,171 people. Rainfall continues in the Highlands west of the Rift Valley (Kitale, Kericho, Nandi, Eldoret, Kakamega), the Lake Basin (Kisumu, Kisii, Busia), parts of Central Rift Valley (Nakuru, Nyahururu), the border areas of Northwestern Kenya (Lokichoggio, Lokitaung), and the Coastal strip (Mombasa, Mtwapa, Malindi, Msabaha, Kilifi, Lamu). Humanitarian access by road is constrained due to insecurity along the Turkana-West Pokot border and due to poor roads conditions in Isiolo, Samburu, Makueni, Tana River, Kitui, and Garissa. As of 25 June 2018, a total of 5,470 cases of cholera with 78 deaths have been reported (Case Fatality Rate of 1.4 per cent). Currently, the outbreak is active in eight counties (Garissa, Tana River, Turkana, West Pokot, Meru, Mombasa, Kilifi and Isiolo counties) with 75 cases reported in the week ending 25 June. A total of 111 cases of Rift Valley Fever (RVF) have been reported with 14 death in three counties (Wajir 75, Marsabit 35 and Siaya 1). Case Fatality Rate is reported at 8 per cent in Wajir and 20 per cent in Marsabit. Active case finding, sample testing, ban of slaughter, quarantine, and community sensitization activities are ongoing. -

Kenya Interagency Rapid Assessment Wajir County August
KENYA INTER AGENCY RAPID ASSESSMENT WAJIR COUNTY CONFLICT ASSESSMENT REPORT August 8 – August 25, 2014 Figure 1: Photo taken by KIRA Assessment Team in Gulani village, Wajir County KIRA – Wajir assessment – August 2014 1 1. OVERVIEW OF THE SITUATION AND CRISIS a. Background of the situation Wajir County is divided into 8 districts namely; Wajir East, Tarbaj, Wajir South, Habaswein, Wajir West, Eldas, Buna and Wajir North districts .There are 6 Sub – counties/constituencies currently that is, Tarbaj, Wajir East, Wajir South, Wajir West, Eldas and Wajir North. The current inter-ethnic clashes between the Degodia and Garre communities along Border areas of Mandera and Wajir began on May 13, 2014. There has been an escalation and repeated attacks in Gunana location in Tarbaj Sub – county at the border of the two counties that is in May and June, 2014 and many people were killed in the conflict. This had spillover effects in the entire Wajir County. The inter clan clashes between Garre and Degodia communities along the Wajir – Mandera Border has directly affected 10 locations in Tarbaj District namely; Lehely, Bojigaras, El Kutulo, Mansa, Burmayo, Ogoralle, Berjanai, Dunto, Basaneja and Gunana, as well as Batalu, Danaba, Gulani, Belowle, Bosicha and Ajawa in Wajir North. Similarly, Wagberi in Wajir Central in Wajir East Sub – County has been affected where many houses were torched and vandalized leading to displacement of residents to in El Ado in Wajir South Sub – county and Hodhan in Wajir East with many others displaced into Mandera County. The clashes in Wajir County further affected other areas that are hosting an influx of displaced persons which include Sarman, Elben, Tarbaj and Kutulo in Tarbaj Sub - county, and Waradey in Eldas Sub - county, and Batalu, Danaba, Quadama and Gulani in Wajir North Sub - county. -

Kenya and Somalia Joint Cross Border Health Coordination
KENYA AND SOMALIA JOINT CROSS BORDER HEALTH COORDINATION MEETING REPORT WAJIR PALACE HOTEL, WAJIR-KENYA. APRIL 4-6, 2018 Introduction The Horn of Africa (HOA) Technical Advisory Group (TAG) meetings noted that the risk of significant WPV outbreaks due to evidence of undetected circulation of WPV among the large number of High-Risk Mobile Populations (HRMP) in the HOA region. The TAG stressed the need for active cross-border health coordinations initiatives as a compelling strategy for polio eradication in the region. The objective of the cross-border coordination meetings is to coordinate efforts to strengthen surveillance, routine immunization, and supplemental immunization activities for polio eradication among bordering areas. Specifically, it aims to improve information sharing between countries on polio eradication, identifying and addressing surveillance and immunity gaps in HRMP along the borders, and planning for synchronized supplementary immunization activities along the borders. This report details April 4-6, 2018 meeting in Wajir county (Kenya). The meeting hosted representation from Kenya National MOH, Kenya border Counties MoH officials (Wajir,Turkana and Garissa), Jubaland State (Somalia), WHO representatives (Kenya & Somalia), UNICEF- Kenya, WHO Horn of Africa office, and CORE GROUP Polio Project (CGPP)-HOA Secretariat and CGPP-HOAS partners (American Refugee Committee(ARC), International Rescue Committee (IRC), World Visio- Kenya and Somali Aid. Objectives of the meeting 1. Review on the status of disease surveillance specifically AFP surveillance/VPDs activities. 2. Institutionalize sharing of information modalities between partners in international border regions 3. Discuss the implementation of the joint action plan for cross border collaborations to strengthen cross border disease AFP surveillance & other diseases, e.g. -

KENYA POPULATION SITUATION ANALYSIS Kenya Population Situation Analysis
REPUBLIC OF KENYA KENYA POPULATION SITUATION ANALYSIS Kenya Population Situation Analysis Published by the Government of Kenya supported by United Nations Population Fund (UNFPA) Kenya Country Oce National Council for Population and Development (NCPD) P.O. Box 48994 – 00100, Nairobi, Kenya Tel: +254-20-271-1600/01 Fax: +254-20-271-6058 Email: [email protected] Website: www.ncpd-ke.org United Nations Population Fund (UNFPA) Kenya Country Oce P.O. Box 30218 – 00100, Nairobi, Kenya Tel: +254-20-76244023/01/04 Fax: +254-20-7624422 Website: http://kenya.unfpa.org © NCPD July 2013 The views and opinions expressed in this report are those of the contributors. Any part of this document may be freely reviewed, quoted, reproduced or translated in full or in part, provided the source is acknowledged. It may not be sold or used inconjunction with commercial purposes or for prot. KENYA POPULATION SITUATION ANALYSIS JULY 2013 KENYA POPULATION SITUATION ANALYSIS i ii KENYA POPULATION SITUATION ANALYSIS TABLE OF CONTENTS LIST OF ACRONYMS AND ABBREVIATIONS ........................................................................................iv FOREWORD ..........................................................................................................................................ix ACKNOWLEDGEMENT ..........................................................................................................................x EXECUTIVE SUMMARY ........................................................................................................................xi -

Beneath the Dryland: Kenya Drought Gender Analysis
Beneath the Dryland Kenya Drought Gender Analysis Oxfam – December 2017 Maria Libertad Mella Dometita, Gender Adviser – Humanitarian Support Personnel Women in Wajir share their stories about how the drought affected their lives. It brought them anguish but at the same time hope, as it presented opportunities to perform new and non-traditional roles. Photo: Maria Libertad Dometita/Oxfam 1 Oxfam Research Reports Oxfam Research Reports are written to share research results, to contribute to public debate and to invite feedback on development and humanitarian policy and practice. They do not necessarily reflect Oxfam policy positions. The views expressed are those of the author and not necessarily those of Oxfam. For more information, or to comment on this report, email Maria Libertad Mella Dometita at [email protected]. © Oxfam International December 2017 This publication is copyright but the text may be used free of charge for the purposes of advocacy, campaigning, education, and research, provided that the source is acknowledged in full. The copyright holder requests that all such use be registered with them for impact assessment purposes. For copying in any other circumstances, or for re-use in other publications, or for translation or adaptation, permission must be secured and a fee may be charged. Email [email protected]. The information in this publication is correct at the time of going to press. Published by Oxfam GB for Oxfam International under ISBN 978-1-78748-154-1 in December 2017. OXFAM Oxfam is an international confederation of 20 organizations networked together in more than 90 countries, as part of a global movement for change, to build a future free from the injustice of poverty. -

Download List of Physical Locations of Constituency Offices
INDEPENDENT ELECTORAL AND BOUNDARIES COMMISSION PHYSICAL LOCATIONS OF CONSTITUENCY OFFICES IN KENYA County Constituency Constituency Name Office Location Most Conspicuous Landmark Estimated Distance From The Land Code Mark To Constituency Office Mombasa 001 Changamwe Changamwe At The Fire Station Changamwe Fire Station Mombasa 002 Jomvu Mkindani At The Ap Post Mkindani Ap Post Mombasa 003 Kisauni Along Dr. Felix Mandi Avenue,Behind The District H/Q Kisauni, District H/Q Bamburi Mtamboni. Mombasa 004 Nyali Links Road West Bank Villa Mamba Village Mombasa 005 Likoni Likoni School For The Blind Likoni Police Station Mombasa 006 Mvita Baluchi Complex Central Ploice Station Kwale 007 Msambweni Msambweni Youth Office Kwale 008 Lunga Lunga Opposite Lunga Lunga Matatu Stage On The Main Road To Tanzania Lunga Lunga Petrol Station Kwale 009 Matuga Opposite Kwale County Government Office Ministry Of Finance Office Kwale County Kwale 010 Kinango Kinango Town,Next To Ministry Of Lands 1st Floor,At Junction Off- Kinango Town,Next To Ministry Of Lands 1st Kinango Ndavaya Road Floor,At Junction Off-Kinango Ndavaya Road Kilifi 011 Kilifi North Next To County Commissioners Office Kilifi Bridge 500m Kilifi 012 Kilifi South Opposite Co-Operative Bank Mtwapa Police Station 1 Km Kilifi 013 Kaloleni Opposite St John Ack Church St. Johns Ack Church 100m Kilifi 014 Rabai Rabai District Hqs Kombeni Girls Sec School 500 M (0.5 Km) Kilifi 015 Ganze Ganze Commissioners Sub County Office Ganze 500m Kilifi 016 Malindi Opposite Malindi Law Court Malindi Law Court 30m Kilifi 017 Magarini Near Mwembe Resort Catholic Institute 300m Tana River 018 Garsen Garsen Behind Methodist Church Methodist Church 100m Tana River 019 Galole Hola Town Tana River 1 Km Tana River 020 Bura Bura Irrigation Scheme Bura Irrigation Scheme Lamu 021 Lamu East Faza Town Registration Of Persons Office 100 Metres Lamu 022 Lamu West Mokowe Cooperative Building Police Post 100 M. -

Bungoma County Council Hall)
Seattle University School of Law Seattle University School of Law Digital Commons The Truth, Justice and Reconciliation I. Core TJRC Related Documents Commission of Kenya 7-9-2011 Public Hearing Transcripts - Western - Bungoma - RTJRC09.07 (Bungoma County Council Hall) Truth, Justice, and Reconciliation Commission Follow this and additional works at: https://digitalcommons.law.seattleu.edu/tjrc-core Recommended Citation Truth, Justice, and Reconciliation Commission, "Public Hearing Transcripts - Western - Bungoma - RTJRC09.07 (Bungoma County Council Hall)" (2011). I. Core TJRC Related Documents. 133. https://digitalcommons.law.seattleu.edu/tjrc-core/133 This Report is brought to you for free and open access by the The Truth, Justice and Reconciliation Commission of Kenya at Seattle University School of Law Digital Commons. It has been accepted for inclusion in I. Core TJRC Related Documents by an authorized administrator of Seattle University School of Law Digital Commons. For more information, please contact [email protected]. ORAL SUBMISSIONS MADE TO THE TRUTH, JUSTICE AND RECONCILIATION COMMISSION HELD ON SATURDAY, 9 TH JULY, 2011 AT BUNGOMA COUNTY COUNCIL HALL PRESENT Gertrude Chawatama - The Presiding Chair, Zambia Berhanu Dinka - Commissioner, Ethiopia Ahmed Sheikh Farah - Commissioner, Kenya (The Commission commenced at 10.00 a.m.) (The Presiding Chair (Commissioner Chawatama) introduced herself and the other TJRC Commissioners) (Opening Prayers) The Presiding Chair (Commissioner Chawatama): Please, be seated. On behalf of the Truth, Justice and Reconciliation Commission (TJRC), I welcome you to our sittings on the second day here in Bungoma. The TJRC thanks you for the warm welcome. It was an honor and privilege to have heard witnesses yesterday who touched on various violations which included torture, murder, wrongful or unfair dismissal and the issue of land. -

Feed the Future Kenya Livestock Market Systems Activity
acdi FEED THE FUTURE KENYA LIVESTOCK MARKET SYSTEMS ACTIVITY Y1Q3 PROGRESS REPORT: APRIL JUNE 2018 1 FEED THE FUTURE KENYA LIVESTOCK MARKET SYSTEMS ACTIVITY Y1 Q3 PROGRESS REPORT LEADER AWARD PERIOD OF ACTIVITY: OCTOBER 1, 2017–SEPTEMBER 30, 2022 AGREEMENT NUMBER: AID-615-L-17-00001 AOR USAID: CHIEF OF PARTY: FEED THE FUTURE LIVESTOCK MARKET SYSTEMS: Expanding and Diversifying Viable Economic Opportunities in Kenya Award PERIOD OF ACTIVITY: OCTOBER 1, 2017–SEPTEMBER 30, 2022 AGREEMENT NUMBER: AID-615-LA-17-00001 AOR USAID: CHIEF OF PARTY: FEED THE FUTURE LIVESTOCK MARKET SYSTEMS: Strengthening the Community Capacities for Resilience and Growth Award PERIOD OF ACTIVITY: OCTOBER 1, 2017–SEPTEMBER 30, 2022 AGREEMENT NUMBER: AID-615-LA-17-00002 AOR USAID: CHIEF OF PARTY: DISCLAIMER This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of ACDI/VOCA and do not necessarily reflect the views of USAID or the United States Government. 2 Cover photo: Community sensitization for small grants at Raya in Garissa county. CONTENTS CONTENTS I ACRONYM LIST V EXECUTIVE SUMMARY 1 LEADER AWARD ACTIVITIES 2 Objective 1 - Effective Management and Quality Assurance 2 Objective 2: Grants Facilities Management 3 Objective 3: PREG Coordination and Backbone Support for Collective Impact and Learning 4 Collaborating, Learning, Adapting (CLA) 4 Objective 4: Central Operational Support Services 4 Monitoring, Evaluation, and Learning (MEL) 4 Human Resources | Finance | Procurement | Operations 5 Communications 5 Planned Activities for the Next Quarter 6 EXPANDING & DIVERSIFYING VIABLE ECONOMIC OPPORTUNITIES IN KENYA (AA1) 8 Objective 1: Expanded and Diversified Viable Economic Opportunities 8 Facilitate more competitive, resilient and inclusive livestock and related market systems to leverage end-market opportunities while insuring inclusion and poverty reduction. -
Security Dynamics in Conservancies in Kenya: the Case of Isiolo County
\ WORKING PAPER 3\ 2020 Security dynamics in conservancies in Kenya: The case of Isiolo County Kennedy Mkutu \ United States International University-Africa, Nairobi Collaborative Research Center 228 Future Rural Africa: Future-making and social-ecological transformation \ WORKING PAPER 3 \ 2020 SECURITY DYNAMICS IN CONSERVANCIES IN KENYA: THE CASE OF ISIOLO COUNTY\ K. MKUTU SUMMARY The community-based conservation model is an increasing phenomenon in Kenya, especially in northern pastoralist counties. This Working Paper, the result of empirical research over several years, considers dimensions of inclusion and exclusion and subsequent conflicts around community- based conservancies in Isiolo County. It finds that conservancies are sometimes established to protect a community’s interests in and access to community land, including formal claim-making over ancestral community land which may spatially exclude other groups. These dimensions are reinforced by the presence of rangers, of whom many are armed National Police Reservists. Spatial and political dimensions of exclusion also exist to some extent within conservancies due to the need to balance wildlife and grazing needs. Armed security forces in conservancies have important implications for state sovereignty and control over the use of force. Importantly, a powerful donor-funded umbrella organisation (the Northern Rangelands Trust) is significantly involved in training, equipping and deploying rangers. The presence of well-equipped armed ranger teams may then inadvertently play into resource-based conflict and alter power balances between ethnic groups as is most clearly high- lighted on the Samburu–Isiolo border. Sustainability is another concern where donor funding is an important source. Another concern for the future is Isiolo’s position at the centre of the country’s infrastructural and economic development plans which threaten to dispossess pastoralists of community land.