Democratic Republic of the Congo
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Drc Integrated Hiv/Aids Project
DRC INTEGRATED HIV/AIDS PROJECT PROJET INTEGRE DE VIH/SIDA AU CONGO (PROVIC) YEAR 1 ANNUAL REPORT October 2009-September 2010 Contract #GHH-I-00-07-00061-00, Order No. 03 Photo s: ProVIC staff LIST OF ACRONYMS AIDS acquired immune deficiency syndrome AMITIE AIDS Mitigation Initiative to Enhance Care and Support in Bukavu, Lubumbashi, and Matadi AMO-Congo Avenir Meilleur pour les Orphelins au Congo ART antiretroviral therapy BCC behavior change communication BDOM Bureau Diocésain des Oeuvres Médicales C-Change Communication for Change CCLD/Midema Corporate Commitment for Local Development/Minoterie de Matadi CODILUSI Diocesan Committee in the Fight Against AIDS CoP Chief of Party COP Country Operational Plan COTR contracting officers’ technical representative CRS Catholic Relief Services CSR Centre de Santé de Reference DRC Democratic Republic of Congo DIVAS Division des Affaires Sociales ECC Eglise du Christ au Congo EGPAF Elizabeth Glaser Pediatric AIDS Foundation EID early infant diagnosis FFP Fondation Femme Plus FHI Family Health International HBMM Hôpital Biamba Marie Mutombo HCT HIV counseling and testing HGR Hopitale General de Reference HIV human immunodeficiency virus HSS health systems strengthening IHAA International HIV/AIDS Alliance IR intermediate result M&E monitoring and evaluation MARP most-at-risk population MINAS Ministère des Affaires Sociales MSH/SPS Management Sciences for Health/Strengthening Pharmaceutical Systems MSM men who have sex with men NGO nongovernmental organization OVC orphans and vulnerable children -
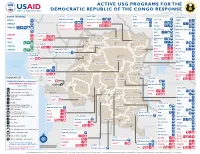
ACTIVE USG PROGRAMS for the DEMOCRATIC REPUBLIC of the CONGO RESPONSE Last Updated 07/27/20
ACTIVE USG PROGRAMS FOR THE DEMOCRATIC REPUBLIC OF THE CONGO RESPONSE Last Updated 07/27/20 BAS-UELE HAUT-UELE ITURI S O U T H S U D A N COUNTRYWIDE NORTH KIVU OCHA IMA World Health Samaritan’s Purse AIRD Internews CARE C.A.R. Samaritan’s Purse Samaritan’s Purse IMA World Health IOM UNHAS CAMEROON DCA ACTED WFP INSO Medair FHI 360 UNICEF Samaritan’s Purse Mercy Corps IMA World Health NRC NORD-UBANGI IMC UNICEF Gbadolite Oxfam ACTED INSO NORD-UBANGI Samaritan’s WFP WFP Gemena BAS-UELE Internews HAUT-UELE Purse ICRC Buta SCF IOM SUD-UBANGI SUD-UBANGI UNHAS MONGALA Isiro Tearfund IRC WFP Lisala ACF Medair UNHCR MONGALA ITURI U Bunia Mercy Corps Mercy Corps IMA World Health G A EQUATEUR Samaritan’s NRC EQUATEUR Kisangani N Purse WFP D WFPaa Oxfam Boende A REPUBLIC OF Mbandaka TSHOPO Samaritan’s ATLANTIC NORTH GABON THE CONGO TSHUAPA Purse TSHOPO KIVU Lake OCEAN Tearfund IMA World Health Goma Victoria Inongo WHH Samaritan’s Purse RWANDA Mercy Corps BURUNDI Samaritan’s Purse MAI-NDOMBE Kindu Bukavu Samaritan’s Purse PROGRAM KEY KINSHASA SOUTH MANIEMA SANKURU MANIEMA KIVU WFP USAID/BHA Non-Food Assistance* WFP ACTED USAID/BHA Food Assistance** SA ! A IMA World Health TA N Z A N I A Kinshasa SH State/PRM KIN KASAÏ Lusambo KWILU Oxfam Kenge TANGANYIKA Agriculture and Food Security KONGO CENTRAL Kananga ACTED CRS Cash Transfers For Food Matadi LOMAMI Kalemie KASAÏ- Kabinda WFP Concern Economic Recovery and Market Tshikapa ORIENTAL Systems KWANGO Mbuji T IMA World Health KWANGO Mayi TANGANYIKA a KASAÏ- n Food Vouchers g WFP a n IMC CENTRAL y i k -

Yellow Fever Outbreak — Kongo Central Province, Democratic Republic of the Congo, August 2016
Morbidity and Mortality Weekly Report Yellow Fever Outbreak — Kongo Central Province, Democratic Republic of the Congo, August 2016 John O. Otshudiema, MD1,2; Nestor G. Ndakala, MD3; Elande-taty K. Mawanda, MD4; Gaston P. Tshapenda, MD5; Jacques M. Kimfuta, MD4; Loupy-Régence N. Nsibu6, MD; Abdou S. Gueye, MD, PhD7; Jacob Dee, MPH8; Rossanne M. Philen, MD7; Coralie Giese, MPH7; Christopher S. Murrill, PhD9; Ray R. Arthur, PhD7; Benoit I. Kebela, MD5 On April 23, 2016, the Democratic Republic of the Congo’s divided by the most recent census estimates for the targeted (DRC’s) Ministry of Health declared a yellow fever outbreak. population). The CDC team visited Kongo Central Province As of May 24, 2016, approximately 90% of suspected yellow during August and September 2016, reviewed yellow fever fever cases (n = 459) and deaths (45) were reported in a single surveillance data reported in the DRC Integrated Disease province, Kongo Central Province, that borders Angola, where Surveillance and Response system, assessed health facilities a large yellow fever outbreak had begun in December 2015. and border ports of entry, interviewed health and border sur- Two yellow fever mass vaccination campaigns were conducted veillance officers, and made recommendations for prevention in Kongo Central Province during May 25–June 7, 2016 and and control. August 17–28, 2016. In June 2016, the DRC Ministry of A suspected yellow fever case was defined by the DRC Health requested assistance from CDC to control the outbreak. Ministry of Health (adapted from the World Health As of August 18, 2016, a total of 410 suspected yellow fever Organization’s standard case definition) as acute onset of cases and 42 deaths were reported in Kongo Central Province. -

EIES-Matadi.Pdf
i Public Disclosure Authorized REPUBLIQUE DEMOCRATIQUE DU CONGO Ministère de l’Energie et Ressources Hydrauliques ==================== CELLULE D’EXECUTION DES PROJETS EAU (CEP-O/REGIDESO) ================ PROJET D’ALIMENTATION EN EAU POTABLE EN MILIEU URBAIN-FINANCEMENT ADDITIONNEL Public Disclosure Authorized (PEMU-FA) Public Disclosure Authorized ETUDE D’IMPACT ENVIRONNEMENTALE ET SOCIALE DES INFRASTRUCTURES HYDRAULIQUES DE LA VILLE DE MATADI DANS LA PROVINCE DU KONGO CENTRAL VERSION FINALE Public Disclosure Authorized AVRIL 2018 ii Table des matières SIGLES ET ABREVIATIONS ................................................................................................. iv LISTE DES TABLEAUX .......................................................................................................... v LISTE DES CARTES ............................................................................................................... vi LISTE DES PHOTOS ............................................................................................................... vi LISTE DES ANNEXES ........................................................................................................... vii RESUME NON TECHNIQUE ............................................................................................... viii NON-TECHNICAL SUMMARY ............................................................................................ xv KINKUFI YA MALONGI .................................................................................................... -

The Human Right to Safe Drinking Water
The Human Right to Safe Drinking Water and Sanitation in the rural Bas-Fleuve region of the Democratic Republic of Congo: Exploring the local conceptions of human rights Pascal Sundi Mbambi Rachel Hammonds Localizing Human Rights Working Paper Series No. 5 (2017) General Editors: Koen De Feyter and Rachel Hammonds Antwerp: University of Antwerp 1 Localizing Human Rights Working Paper Series The Localizing Human Rights Working Paper Series consists of studies on the local relevance of human rights, particularly but not exclusively in non-Western contexts. They form part of a long-term interdisciplinary project, combining insights from law, political and social sciences. The Localizing Human Rights Research Programme is coordinated by the Law and Development Research Group at the University of Antwerp (Belgium). General Editors of the Series are Professor Koen De Feyter, Chair of International Law at the University of Antwerp, and Dr. Rachel Hammonds, University of Antwerp. The full reports are available online on the website of the Law and Development Research Group. The Localizing Human Rights Working Paper Series: No. 1: Vandenbogaerde, Arne (2015). The Human Rights Council from Below. A Case Study of the Declaration on the Rights of Peasants. No. 2: Destrooper, Tine (2015). An Analysis of the Human Rights-Based Approach to Development. UNICEF’s Role in the Villages Assainis Program in the Bas-Congo. No. 3: Chen, Jingrong, Desmet, Ellen and De Feyter, Koen (2016). The Right to Education of Rural-Urban Migrant Households in Chongqing, China. No. 4: De Feyter, Koen, Singh, Maheshwar, Kiekens, Dominique, Desguin, Noémi, Goel, Arushi and Saxena, Devanshi (2017). -

Colonialism and Its Socio-Politico and Economic Impact: a Case Study of the Colonized Congo Gulzar Ahmad & Muhamad Safeer Awan
Colonialism and its Socio-politico and Economic Impact: A Case study of the Colonized Congo Gulzar Ahmad & Muhamad Safeer Awan Abstract The exploitation of African Congo during colonial period is an interesting case study. From 1885 to 1908, it remained in the clutches of King Leopold II. During this period the Congo remained a victim of exploitation which has far sighted political, social and economic impacts. The Congo Free State was a large state in Central Africa which was in personal custody of King Leopold II. The socio-politico and economic study of the state reflects the European behaviour and colonial policy, a point of comparison with other colonial experiences. The analysis can be used to show that the abolition of the slave trade did not necessarily lead to a better experience for Africans at the hands of Europeans. It could also be used to illustrate the problems of our age. The social reformers, political leaders; literary writers and the champion of human rights have their own approaches and interpretations. Joseph Conrad is one of the writers who observed the situation and presented them in fictional and historical form in his books, Heart of Darkness, The Congo Diary, Notes on Life and Letters and Personal Record. In this paper a brief analysis is drawn about the colonialism and its socio-political and psychological impact in the historical perspectives. Keywords: Colonialism, Exploitation, Colonialism, Congo. Introduction The state of Congo, the heart of Africa, was colonized by Leopold II, king of the Belgium from 1885 to 1908. During this period it remained in the clutches of colonialism. -

Cycles Approved by OHRM for S
Consolidated list of duty stations approved by OHRM for rest and recuperation (R & R) (as of 1 July 2015) Duty Station Frequency R & R Destination AFGHANISTAN Entire country 6 weeks Dubai ALGERIA Tindouf 8 weeks Las Palmas BURKINA FASO Dori 12 weeks Ouagadougou BURUNDI Bujumbura, Gitega, Makamba, Ngozi 8 weeks Nairobi CENTRAL AFRICAN REPUBLIC Entire country 6 weeks Yaoundé CHAD Abeche, Farchana, Goré, Gozbeida, Mao, N’Djamena, Sarh 8 weeks Addis Ababa COLOMBIA Quibdo 12 weeks Bogota COTE D’IVOIRE Entire country except Abidjan and Yamoussoukro 8 weeks Accra DEMOCRATIC REPUBLIC OF THE CONGO Aru, Beni, Bukavu, Bunia, Butembo, Dungu, Goma, Kalemie, Mahagi, Uvira 6 weeks Entebbe Bili, Bandundu, Gemena, Kamina, Kananga, Kindu, Kisangani, Matadi, Mbandaka, Mbuji-Mayi 8 weeks Entebbe Lubumbashi 12 weeks Entebbe DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA Pyongyang 8 weeks Beijing ETHIOPIA Kebridehar 6 weeks Addis Ababa Jijiga 8 weeks Addis Ababa GAZA Gaza (entire) 8 weeks Amman GUINEA Entire country 6 weeks Accra HAITI Entire country 8 weeks Santo Domingo INDONESIA Jayapura 12 weeks Jakarta IRAQ Baghdad, Basrah, Kirkuk, Dohuk 4 weeks Amman Erbil, Sulaymaniah 8 weeks Amman KENYA Dadaab, Wajir, Liboi 6 weeks Nairobi Kakuma 8 weeks Nairobi KYRGYZSTAN Osh 8 weeks Istanbul LIBERIA Entire country 8 weeks Accra LIBYA Entire country 6 weeks Malta MALI Gao, Kidal, Tesalit 4 weeks Dakar Tombouctou, Mopti 6 weeks Dakar Bamako, Kayes 8 weeks Dakar MYANMAR Sittwe 8 weeks Yangon Myitkyina (Kachin State) 12 weeks Yangon NEPAL Bharatpur, Bidur, Charikot, Dhunche, -

Democratic Republic of Congo Round 7 – Service Delivery Point Questionnaire
Democratic Republic of Congo Round 7 – Service Delivery Point Questionnaire ◯ Yes 001a. Your ID: [NAME] Is this your ID? ◯ No 001b. Enter your ID below. Please record your ID Day: 002b. Record the correct date and time. Month: Year: ◯ KonGo Central 003a. Province ◯ KINSHASA ◯ BARUMBU ◯ BAS_FLEUVE ◯ BINZA_METEO ◯ BINZA_OZONE ◯ BIYELA ◯ BOMA ◯ BUMBU ◯ CATARACTES ◯ KALAMU_I ◯ KALAMU_II ◯ KIKIMI ◯ KIMBANSEKE ◯ KINGABWA ◯ KINGASANI ◯ KINSHASA 003b. District ◯ KINTAMBO ◯ KISENSO ◯ LEMBA ◯ LIMETE ◯ LINGWALA ◯ LUKAYA ◯ MASINA_I ◯ MASINA_II ◯ MATADI ◯ MATETE ◯ MONT_NGAFULA_I ◯ MONT_NGAFULA_II ◯ NGABA ◯ NGIRINGIRI ◯ SELEMBAO 1 ◯ BARUMBU ◯ BAS_FLEUVE ◯ BINZA_METEO ◯ BINZA_OZONE ◯ BIYELA ◯ BOMA ◯ BUMBU ◯ CATARACTES ◯ KALAMU_I ◯ KALAMU_II ◯ KIKIMI ◯ KIMBANSEKE ◯ KINGABWA ◯ KINGASANI ◯ KINSHASA 003b. Zone de Santé ◯ KINTAMBO ◯ KISENSO ◯ LEMBA ◯ LIMETE ◯ LINGWALA ◯ LUKAYA ◯ MASINA_I ◯ MASINA_II ◯ MATADI ◯ MATETE ◯ MONT_NGAFULA_I ◯ MONT_NGAFULA_II ◯ NGABA ◯ NGIRINGIRI ◯ SELEMBAO ◯ 17_MAI ◯ ASSOSSA_NGIRI_NGIRI ◯ BAKI_VILLE ◯ BAMBOMA ◯ BANA ◯ BANGU ◯ BETON ◯ BINZA_PIGEON 003c. Aire de Santé ◯ BITSHAKU_TSHAKU ◯ BOBA ◯ BUMBA ◯ BUNZI ◯ CAMP_PERMANENT ◯ CNECI ◯ CONGO ◯ CONGO_1 2 ◯ DIANGIENDA_I ◯ DINGI_DINGI ◯ ESSANGA ◯ HYGIENE_A ◯ IMBALI ◯ INGA ◯ KAPINGA ◯ KASAI_MASINA ◯ KASAI_BUMBU ◯ KAUKA_I ◯ KEMI ◯ KHAMI ◯ KHESA ◯ KIFUMA_NGIMBI ◯ KIKIMI ◯ KIMBANGU_A ◯ KIMBANZA ◯ KIMBATA___TUDI ◯ KIMBIANGA ◯ KIMBONDO1(_KINDELE) ◯ KIMUAKA ◯ KINGABWA ◯ KINKENGE ◯ KINSUKA_PECHEUR ◯ KINZAU_MVUE ◯ KIPASA ◯ KISANTU ◯ KISENSO_GARE ◯ KITOMESA ◯ KIVALA_TADI ◯ KIVEVE ◯ KIVUNDA ◯ KUMBI -

Mobile Money in the Democratic Republic of Congo: Market Insights on Consumer Needs and Opportunities in Payments and Financial Services
Mobile Money in the Democratic Republic of Congo: Market insights on consumer needs and opportunities in payments and financial services July 2013 MMU_DRCongo_Report_200613.indd 1 20/06/2013 17:33 Contents 3 Executive Summary 5 Project overview and introduction 7 Key findings 7 Market context: use of financial services limited in the DRC 8 Preference and prevalence of financial services in the DRC 8 — Insights from household decision-makers 18 — Insight from small business owners 20 Opportunities and challenges for mobile operators moving into mobile money 27 Conclusions and recommendations 29 Appendix 1. Household decision-makers’ survey: sample demographics 31 Appendix 2: Research methodology Figures 8 Figure 1 – Percentage who received a transfer in each province 9 Figure 2 – Destination of transfers sent and origins of transfers received 10 Figure 3 – Percentage who sent money for each reason “most often” 10 Figure 4 – Percentage who received money for each reason “most often” 11 Figure 5 – Percentage who used each method to send money in previous three months 12 Figure 6 – Reasons for using each transfer service (Percentage for each) 13 Figure 7 – Percentage who paid each type of bill in the previous three months 14 Figure 8 – Of those who had paid a bill, the percentage who had paid each type of bill in the previous three months, by province 15 Figure 9 – Percentage of each sector who received a salary or wage payment in the previous three months 16 Figure 10 – Reasons respondents save money 16 Figure 11 – Of the households who -
Kitona Operations: Rwanda's Gamble to Capture Kinshasa and The
Courtesy of Author Courtesy of Author of Courtesy Rwandan Patriotic Army soldiers during 1998 Congo war and insurgency Rwandan Patriotic Army soldiers guard refugees streaming toward collection point near Rwerere during Rwanda insurgency, 1998 The Kitona Operation RWANDA’S GAMBLE TO CAPTURE KINSHASA AND THE MIsrEADING OF An “ALLY” By JAMES STEJSKAL One who is not acquainted with the designs of his neighbors should not enter into alliances with them. —SUN TZU James Stejskal is a Consultant on International Political and Security Affairs and a Military Historian. He was present at the U.S. Embassy in Kigali, Rwanda, from 1997 to 2000, and witnessed the events of the Second Congo War. He is a retired Foreign Service Officer (Political Officer) and retired from the U.S. Army as a Special Forces Warrant Officer in 1996. He is currently working as a Consulting Historian for the Namib Battlefield Heritage Project. ndupress.ndu.edu issue 68, 1 st quarter 2013 / JFQ 99 RECALL | The Kitona Operation n early August 1998, a white Boeing remain hurdles that must be confronted by Uganda, DRC in 1998 remained a safe haven 727 commercial airliner touched down U.S. planners and decisionmakers when for rebels who represented a threat to their unannounced and without warning considering military operations in today’s respective nations. Angola had shared this at the Kitona military airbase in Africa. Rwanda’s foray into DRC in 1998 also concern in 1996, and its dominant security I illustrates the consequences of a failure to imperative remained an ongoing civil war the southwestern Bas Congo region of the Democratic Republic of the Congo (DRC). -

Broadcasting Board of Governors JUSTIFICATION for OTHER THAN FULL and OPEN COMPETITION Under FAR PART 13.5 1. Agency: Broadcas
Broadcasting Board of Governors JUSTIFICATION FOR OTHER THAN FULL AND OPEN COMPETITION under FAR PART 13.5 1. Agency: Broadcasting Board of Governors , OMS Office of Contracting 2. Description of Action Being Approved: This action will result in the issuance of a firm fixed price contract that will be for a one year base and 4 - one year options. 3. Description of Supplies or Services Required to Meet the Agency’s Need: The services being acquired are for Zaou Mouanda. This includes Backup Power Generator Maintenance, providing fuel, repair of the FM broadcast system to include satellite reception equipment. The services, for Uninterrupted 24 x 7 FM Broadcast Operations, are to be provided in Lubumbashi, Goma, Kisangani, Bukavu, Matadi, Kananga, and Mbuji Mayi in the Democratic Republic of the Congo (DRC). The estimated value is $434,700.00, to include all option years. 4. Identification of the Statutory Authority Permitting Other Than Full and Open Competition: This acquisition is being conducted under the authority of Federal Acquisition Regulation Part 13.5 and 41 U.S.C. 1901, which is implemented under the authority of Federal Acquisition Regulations (FAR) 6.303-2. Only one responsible source and no other supplies or services will satisfy Agency requirements. The contracting officer deems only one source reasonably available because Zaou Mouanda is the sole maintainer of BBG’s FM broadcast system, Backup Power Generator Maintenance, and fuel for uninterrupted 24 x 7 FM broadcast operations in Lubumbashi, Goma, Kisangani, Bukavu, Matadi, Kananga, and Mbuji Mayi in the Democratic Republic of the Congo (DRC). 5. -

1. RESUME 2. Surveillance Epidémiologique
RAPPORT DE SITUATION FIEVRE JAUNE EN RD CONGO Bureau du Représentant | 42, avenue des Cliniques, Kinshasa / Gombe | République Démocratique du Congo Sitrep du 25 mai 2016 1. RESUME Lancement ce jour de la campagne de vaccination contre la fièvre jaune dans les deux zones de santé ciblées de la Ville-Province de Kinshasa (N’djili et Masina). A N’djili, 138 sites de vaccination et à Masina, 193 sites de vaccination ont été mis en place. Au Kongo-central, le lancement officiel local a été organisé dans deux zones de santé (Boma et Kitona) par les autorités politico-administratives. Pas de nouveau cas de fièvre jaune confirmé depuis deux jours ; la plus récente date de début de la maladie chez un cas confirmé est le 10 mai 2016. A la date du 25 mai, au total 48 cas confirmé de fièvre jaune sont notifiés. Deux cas urbains confirmés dont un à N’djili (Kinshasa) et un à Matadi (Kongo central) sont autochtones. Deux (2) cas confirmés sont en attente de classification finale. Deux représentants de l’ambassade du Japon en RD Congo ont visité l’OMS pays pour discuter de leur implication dans la réponse à l’épidémie. 2. Surveillance Epidémiologique A la date du 24 mai 2016, un total de 649 cas suspects incluant 61 décès (létalité : 9,4 %) ont été rapportés par le système national de surveillance. Parmi ces cas, 48 ont été confirmés dans 19 zones de santé des cinq provinces suivantes : Bas-Uélé, Kwango (ex Bandundu), Tshuapa, Kongo- Central et Kinshasa. Parmi ces cas, quarante et un (41) sont classés comme importés de l’Angola et ont été notifiés dans les provinces du Kongo-Central (31 cas), Kinshasa (9 cas) et Kwango (1 cas).