Yellow Fever 12 May 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
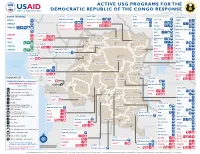
ACTIVE USG PROGRAMS for the DEMOCRATIC REPUBLIC of the CONGO RESPONSE Last Updated 07/27/20
ACTIVE USG PROGRAMS FOR THE DEMOCRATIC REPUBLIC OF THE CONGO RESPONSE Last Updated 07/27/20 BAS-UELE HAUT-UELE ITURI S O U T H S U D A N COUNTRYWIDE NORTH KIVU OCHA IMA World Health Samaritan’s Purse AIRD Internews CARE C.A.R. Samaritan’s Purse Samaritan’s Purse IMA World Health IOM UNHAS CAMEROON DCA ACTED WFP INSO Medair FHI 360 UNICEF Samaritan’s Purse Mercy Corps IMA World Health NRC NORD-UBANGI IMC UNICEF Gbadolite Oxfam ACTED INSO NORD-UBANGI Samaritan’s WFP WFP Gemena BAS-UELE Internews HAUT-UELE Purse ICRC Buta SCF IOM SUD-UBANGI SUD-UBANGI UNHAS MONGALA Isiro Tearfund IRC WFP Lisala ACF Medair UNHCR MONGALA ITURI U Bunia Mercy Corps Mercy Corps IMA World Health G A EQUATEUR Samaritan’s NRC EQUATEUR Kisangani N Purse WFP D WFPaa Oxfam Boende A REPUBLIC OF Mbandaka TSHOPO Samaritan’s ATLANTIC NORTH GABON THE CONGO TSHUAPA Purse TSHOPO KIVU Lake OCEAN Tearfund IMA World Health Goma Victoria Inongo WHH Samaritan’s Purse RWANDA Mercy Corps BURUNDI Samaritan’s Purse MAI-NDOMBE Kindu Bukavu Samaritan’s Purse PROGRAM KEY KINSHASA SOUTH MANIEMA SANKURU MANIEMA KIVU WFP USAID/BHA Non-Food Assistance* WFP ACTED USAID/BHA Food Assistance** SA ! A IMA World Health TA N Z A N I A Kinshasa SH State/PRM KIN KASAÏ Lusambo KWILU Oxfam Kenge TANGANYIKA Agriculture and Food Security KONGO CENTRAL Kananga ACTED CRS Cash Transfers For Food Matadi LOMAMI Kalemie KASAÏ- Kabinda WFP Concern Economic Recovery and Market Tshikapa ORIENTAL Systems KWANGO Mbuji T IMA World Health KWANGO Mayi TANGANYIKA a KASAÏ- n Food Vouchers g WFP a n IMC CENTRAL y i k -

Colonialism and Its Socio-Politico and Economic Impact: a Case Study of the Colonized Congo Gulzar Ahmad & Muhamad Safeer Awan
Colonialism and its Socio-politico and Economic Impact: A Case study of the Colonized Congo Gulzar Ahmad & Muhamad Safeer Awan Abstract The exploitation of African Congo during colonial period is an interesting case study. From 1885 to 1908, it remained in the clutches of King Leopold II. During this period the Congo remained a victim of exploitation which has far sighted political, social and economic impacts. The Congo Free State was a large state in Central Africa which was in personal custody of King Leopold II. The socio-politico and economic study of the state reflects the European behaviour and colonial policy, a point of comparison with other colonial experiences. The analysis can be used to show that the abolition of the slave trade did not necessarily lead to a better experience for Africans at the hands of Europeans. It could also be used to illustrate the problems of our age. The social reformers, political leaders; literary writers and the champion of human rights have their own approaches and interpretations. Joseph Conrad is one of the writers who observed the situation and presented them in fictional and historical form in his books, Heart of Darkness, The Congo Diary, Notes on Life and Letters and Personal Record. In this paper a brief analysis is drawn about the colonialism and its socio-political and psychological impact in the historical perspectives. Keywords: Colonialism, Exploitation, Colonialism, Congo. Introduction The state of Congo, the heart of Africa, was colonized by Leopold II, king of the Belgium from 1885 to 1908. During this period it remained in the clutches of colonialism. -

Cycles Approved by OHRM for S
Consolidated list of duty stations approved by OHRM for rest and recuperation (R & R) (as of 1 July 2015) Duty Station Frequency R & R Destination AFGHANISTAN Entire country 6 weeks Dubai ALGERIA Tindouf 8 weeks Las Palmas BURKINA FASO Dori 12 weeks Ouagadougou BURUNDI Bujumbura, Gitega, Makamba, Ngozi 8 weeks Nairobi CENTRAL AFRICAN REPUBLIC Entire country 6 weeks Yaoundé CHAD Abeche, Farchana, Goré, Gozbeida, Mao, N’Djamena, Sarh 8 weeks Addis Ababa COLOMBIA Quibdo 12 weeks Bogota COTE D’IVOIRE Entire country except Abidjan and Yamoussoukro 8 weeks Accra DEMOCRATIC REPUBLIC OF THE CONGO Aru, Beni, Bukavu, Bunia, Butembo, Dungu, Goma, Kalemie, Mahagi, Uvira 6 weeks Entebbe Bili, Bandundu, Gemena, Kamina, Kananga, Kindu, Kisangani, Matadi, Mbandaka, Mbuji-Mayi 8 weeks Entebbe Lubumbashi 12 weeks Entebbe DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA Pyongyang 8 weeks Beijing ETHIOPIA Kebridehar 6 weeks Addis Ababa Jijiga 8 weeks Addis Ababa GAZA Gaza (entire) 8 weeks Amman GUINEA Entire country 6 weeks Accra HAITI Entire country 8 weeks Santo Domingo INDONESIA Jayapura 12 weeks Jakarta IRAQ Baghdad, Basrah, Kirkuk, Dohuk 4 weeks Amman Erbil, Sulaymaniah 8 weeks Amman KENYA Dadaab, Wajir, Liboi 6 weeks Nairobi Kakuma 8 weeks Nairobi KYRGYZSTAN Osh 8 weeks Istanbul LIBERIA Entire country 8 weeks Accra LIBYA Entire country 6 weeks Malta MALI Gao, Kidal, Tesalit 4 weeks Dakar Tombouctou, Mopti 6 weeks Dakar Bamako, Kayes 8 weeks Dakar MYANMAR Sittwe 8 weeks Yangon Myitkyina (Kachin State) 12 weeks Yangon NEPAL Bharatpur, Bidur, Charikot, Dhunche, -

Mobile Money in the Democratic Republic of Congo: Market Insights on Consumer Needs and Opportunities in Payments and Financial Services
Mobile Money in the Democratic Republic of Congo: Market insights on consumer needs and opportunities in payments and financial services July 2013 MMU_DRCongo_Report_200613.indd 1 20/06/2013 17:33 Contents 3 Executive Summary 5 Project overview and introduction 7 Key findings 7 Market context: use of financial services limited in the DRC 8 Preference and prevalence of financial services in the DRC 8 — Insights from household decision-makers 18 — Insight from small business owners 20 Opportunities and challenges for mobile operators moving into mobile money 27 Conclusions and recommendations 29 Appendix 1. Household decision-makers’ survey: sample demographics 31 Appendix 2: Research methodology Figures 8 Figure 1 – Percentage who received a transfer in each province 9 Figure 2 – Destination of transfers sent and origins of transfers received 10 Figure 3 – Percentage who sent money for each reason “most often” 10 Figure 4 – Percentage who received money for each reason “most often” 11 Figure 5 – Percentage who used each method to send money in previous three months 12 Figure 6 – Reasons for using each transfer service (Percentage for each) 13 Figure 7 – Percentage who paid each type of bill in the previous three months 14 Figure 8 – Of those who had paid a bill, the percentage who had paid each type of bill in the previous three months, by province 15 Figure 9 – Percentage of each sector who received a salary or wage payment in the previous three months 16 Figure 10 – Reasons respondents save money 16 Figure 11 – Of the households who -
Kitona Operations: Rwanda's Gamble to Capture Kinshasa and The
Courtesy of Author Courtesy of Author of Courtesy Rwandan Patriotic Army soldiers during 1998 Congo war and insurgency Rwandan Patriotic Army soldiers guard refugees streaming toward collection point near Rwerere during Rwanda insurgency, 1998 The Kitona Operation RWANDA’S GAMBLE TO CAPTURE KINSHASA AND THE MIsrEADING OF An “ALLY” By JAMES STEJSKAL One who is not acquainted with the designs of his neighbors should not enter into alliances with them. —SUN TZU James Stejskal is a Consultant on International Political and Security Affairs and a Military Historian. He was present at the U.S. Embassy in Kigali, Rwanda, from 1997 to 2000, and witnessed the events of the Second Congo War. He is a retired Foreign Service Officer (Political Officer) and retired from the U.S. Army as a Special Forces Warrant Officer in 1996. He is currently working as a Consulting Historian for the Namib Battlefield Heritage Project. ndupress.ndu.edu issue 68, 1 st quarter 2013 / JFQ 99 RECALL | The Kitona Operation n early August 1998, a white Boeing remain hurdles that must be confronted by Uganda, DRC in 1998 remained a safe haven 727 commercial airliner touched down U.S. planners and decisionmakers when for rebels who represented a threat to their unannounced and without warning considering military operations in today’s respective nations. Angola had shared this at the Kitona military airbase in Africa. Rwanda’s foray into DRC in 1998 also concern in 1996, and its dominant security I illustrates the consequences of a failure to imperative remained an ongoing civil war the southwestern Bas Congo region of the Democratic Republic of the Congo (DRC). -

Broadcasting Board of Governors JUSTIFICATION for OTHER THAN FULL and OPEN COMPETITION Under FAR PART 13.5 1. Agency: Broadcas
Broadcasting Board of Governors JUSTIFICATION FOR OTHER THAN FULL AND OPEN COMPETITION under FAR PART 13.5 1. Agency: Broadcasting Board of Governors , OMS Office of Contracting 2. Description of Action Being Approved: This action will result in the issuance of a firm fixed price contract that will be for a one year base and 4 - one year options. 3. Description of Supplies or Services Required to Meet the Agency’s Need: The services being acquired are for Zaou Mouanda. This includes Backup Power Generator Maintenance, providing fuel, repair of the FM broadcast system to include satellite reception equipment. The services, for Uninterrupted 24 x 7 FM Broadcast Operations, are to be provided in Lubumbashi, Goma, Kisangani, Bukavu, Matadi, Kananga, and Mbuji Mayi in the Democratic Republic of the Congo (DRC). The estimated value is $434,700.00, to include all option years. 4. Identification of the Statutory Authority Permitting Other Than Full and Open Competition: This acquisition is being conducted under the authority of Federal Acquisition Regulation Part 13.5 and 41 U.S.C. 1901, which is implemented under the authority of Federal Acquisition Regulations (FAR) 6.303-2. Only one responsible source and no other supplies or services will satisfy Agency requirements. The contracting officer deems only one source reasonably available because Zaou Mouanda is the sole maintainer of BBG’s FM broadcast system, Backup Power Generator Maintenance, and fuel for uninterrupted 24 x 7 FM broadcast operations in Lubumbashi, Goma, Kisangani, Bukavu, Matadi, Kananga, and Mbuji Mayi in the Democratic Republic of the Congo (DRC). 5. -

Urban Population Map Gis Unit, Monuc 12°E 14°E 16°E 18°E 20°E 22°E 24°E 26°E 28°E 30°E
DEMOCRATIC REPUBLIC OF CONGO Map No- KINSUB1614 AFRICA URBAN POPULATION MAP GIS UNIT, MONUC 12°E 14°E 16°E 18°E 20°E 22°E 24°E 26°E 28°E 30°E CENTRAL AFRICAN REPUBLIC SUDAN CAMEROON Mobayi-Mbongo Zongo Bosobolo Ango N Gbadolite N ° ° 4 Yakoma 4 Niangara Libenge Bondo Dungu Gemena Mombombo Bambesa Poko Isiro Aketi Bokungu Buta Watsa Aru r e v i Kungu R i g Dimba n a b Binga U Lisala Bumba Mahagi Wamba Nioka N N ° C ° 2 o 2 ng o Djugu R i v Lake Albert Bongandanga er Irumu Bomongo Bunia Basankusu Basoko Bafwasende Yahuma Kituku Yangambi Bolomba K ii s a n g a n ii Beni Befale Lubero UGANDA Katwa N M b a n d a k a N ° ° 0 0 Butembo Ingende Ubundu Lake Edward Kayna GABON Bikoro Opala Lubutu Kanyabayonga CONGO Isangi Boende Kirumba Lukolela Rutshuru Ikela Masisi Punia Kiri WalikaleKairenge Monkoto G o m a Inongo S S ° Lake Kivu ° 2 RWANDA 2 Bolobo Lomela Kamisuku Shabunda B u k a v u Walungu Kutu Mushie B a n d u n d u Kamituga Ilebo K ii n d u Oshwe Dekese Lodja BURUNDI Kas Katako-Kombe ai R Uvira iver Lokila Bagata Mangai S Kibombo S ° ° 4 4 K ii n s h a s a Dibaya-Lubwe Budja Fizi Bulungu Kasongo Kasangulu Masi-Manimba Luhatahata Tshela Lubefu Kenge Mweka Kabambare TANZANIA Idiofa Lusambo Mbanza-Ngungu Inkisi ANGOLA Seke-Banza Luebo Lukula Kinzau-Vuete Lubao Kongolo Kikwit Demba Inga Kimpese Boma Popokabaka Gungu M b u j i - M a y i Songololo M b u j i - M a y i Nyunzu S S ° M a tt a d ii ° 6 K a n a n g a 6 K a n a n g a Tshilenge Kabinda Kabalo Muanda Feshi Miabi Kalemie Kazumba Dibaya Katanda Kasongo-Lunda Tshimbulu Lake Tanganyika Tshikapa -

Configurations of Authority in Kongo Central Province: Governance, Access to Justice, and Security in the Territory of Muanda
JSRP Paper 35 Configurations of Authority in Kongo Central province: governance, access to justice, and security in the territory of Muanda Tatiana Carayannis, José Bazonzi, Aaron Pangburn (Social Science Research Council) February 2017 © Tatiana Carayannis, José Bazonzi, Aaron Pangburn (2017) Although every effort is made to ensure the accuracy and reliability of material published in this paper, the Justice and Security Research Programme and the LSE accept no responsibility for the veracity of claims or accuracy of information provided by contributors. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means without the prior permission of the publisher, nor be issued to the public or circulated in any form other than that in which it is published. Requests for permission to reproduce any part of this paper should be sent to: The Editor, Justice and Security Research Programme, International Development Department, LSE, Houghton Street, London WC2A 2AE Or by email to: [email protected] Contents Introduction ............................................................................ 4 A History of Public Authority in Kongo Central ....................... 5 Justice, security, and public protection ................................ 12 Competition for Public Authority .......................................... 17 External Interventions .......................................................... 24 Conclusion ............................................................................ 26 Configurations of authority in Kongo Central province: Governance, access to justice and security in the territory of Muanda Tatiana Carayannis, Jose Bazonzi, and Aaron Pangburn Introduction One of the objectives of the Justice and Security Research Program (JSRP) is to analyze both formal and informal governance and authority structures in conflict affected areas in Central Africa and to examine security and justice practices provided by these structures. -

The Red Rubber Regime
INTRODUCTION The Red Rubber Regime Prior to 1880, the countries ofEurope claimed relatively few territorial possessions in Africa. The British occupied several coastal pockets in West Africa, including Gambia, Sierra Leone, and Lagos; the French held territory along the North African coast in Algiers, and in Senegal and Gabon in West Africa; and Portuguese rule was extended to portions ofAngola along the west coast and Mozambique along the east coast. Except for the Afrikaner penetration into the South and Turkish claims in North Africa, Egypt, and the Nile region, the vast interior of the continent was largely unexplored and remained under the control of African government. However, all this would change during the next twenty years. By the beginning ofthe twentieth century the continent would be divided into forty states under the control ofvarious European countries. The colonial partition ofAfrica was initiated by King Leopold II of Belgium, whose greed and exploitation in the Congo knew no bounds, and by the sudden territorial claims made by Germany from 1883 to 1885. Leopold used the newly created International African Association to carry out his secret ambitions in central Africa. The African Association was organized in Brussels in 1876 at a meeting of explorers, geographers, and other delegates, lavishly hosted by the Belgian king. Although the stated purpose of the association was to further scientific and commercial development, to eradicate the slave trade, and to aid the work ofChristian missions, in reality it was used by Leopold as a cover for his colonial activities. The actions ofLeopold and Germany opened the floodgates for other European nations to rush in and stake their own claims. -

Annex 14: Governance Plan
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: 53053-ZR PROJECT APPRAISAL DOCUMENT ON A PROPOSED GRANT IN THE AMOUNT OF SDR 168.8 MILLION Public Disclosure Authorized (US$255.0 MILLION EQUIVALENT) TO THE DEMOCRATIC REPUBLIC OF THE CONGO FOR A MULTIMODAL TRANSPORT PROJECT Public Disclosure Authorized MAY 26, 2010 Transport Sector Country Department AFCC2 Africa Region This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without Public Disclosure Authorized World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective April 30, 2010) Currency Unit = Franc Congolais CDF1 = 0.00108 US$ US$1 = 0.66176 SDR FISCAL YEAR January 1 – December 31 ABBREVIATIONS AND ACRONYMS ADS-B Automated Dependent Surveillance–Broadcast AFD Agence Française de Développement (French Agency for Development) AfDB African Development Bank ANR Agence Nationale de Renseignements (National Intelligence Agency) ATS Air Traffic System BCECO Bureau Central de Coordination (Central Coordination Office) BIVAC Bureau d’Inspection, d’Evaluation, d’Estimation et de Contrôle (Bureau of Inspection, Valuation, Assessment and Control) BTC Belgian Technical Cooperation CAC Commissaire Aux Comptes (Auditor) CAS Country Assistance Strategy CEEC Centre d’Evaluation, d’Expertise et de Certification des substances minérales, précieuses et semi-précieuses (Evaluation, Expertise and Certification of Minerals, Precious and Semi-Precious -

Download Africa
30˚ 20˚ 10˚ 0˚ 10˚ 20˚ 30˚ 40˚ 50˚ 60˚ 70˚ Ireland Manchester Minsk Orenburg Arqalyq 50˚ Dublin United Vilnius Tula Penza Kingdom Amsterdam Berlin Bug Novotroitsk Swansea Neth. Germany Belarus Homyel' Russia Kazakhstan Poland Ural Aqtobe Bel. The Hague Voronezh London Warsaw Temir Zhezqazghan Atlantic Guernsey Prague Brussels L'viv Kharkiv Don Jersey Lux. Czech Rep. Volga Shalqar Aral Ukraine Kiev Makat North Aral Sea Ocean Paris Slovakia Dnieper Donets'k Atyrau Nantes Munich Vienna Karaton Qyzylorda Bay of Loire Bratislava Moldova Bern Liech. Austria Chisinau Aral Sea Biscay Hungary Budapest Beyneu Lausanne Switz. LjubljanaSlovenia Romania Odesa Rostov-na-Donu Bordeaux France Zagreb La Coruna Lyon Croatia Belgrade Simferopol' Kungrad Nukus Oviedo Toulouse Milan Verona Bosnia & Vladikavkaz Uzbekistan San Marino Herz. Serbia Bucharest Amu 40˚ Dar SarajevoMontenegro Black Sea K'ut'aisi Urganch Bilbao Marseille Sofia y 40˚ Valladolid Andorra Kosovo Bulgaria Tbilisi a Corsica Podgorica Georgia Portugal Italy Azerbaijan Baku Turkmenistan Azores Madrid Albania Skopje Istanbul VanadzoArrmenia Spain Barcelona Rome Macedonia Sardinia Mary Lisbon Ankara Araks Ashgabat San Vito Naples Bari Tirana Yerevan Caspian Sea Valencia Balearic Greece Izmir Malatya Tabriz Gorgan Setubal Islands Palermo Afyon Turkey Seville Malaga Annaba Sicily Adana Messina Athens Mosul Tehran Mashhad Oran Siracusa Algiers Tunis Northern Cyprus Aleppo Kirkuk Tabas Madeira Rabat Malta Syria Islands Nicosia Cyprus Qom Casablanca Oujda Iraklion Crete Iran Fes El Oued Damascus -

Secretariat 1 January 2017
United Nations ST/IC/2017/10 Secretariat 1 January 2017 Information circular* To: Members of the staff From: The Assistant Secretary-General for Human Resources Management Subject: Designation of duty stations for purposes of rest and recuperation 1. In accordance with administrative instruction ST/AI/2011/7 and Amend.1 and 2, on rest and recuperation, and following inter-agency consultations, the Office of Human Resources Management approves the Secretariat duty stations that qualify for rest and recuperation, the frequencies thereof and the designation of rest and recuperation destinations. The annex to the present circular contains the list of duty stations approved for rest and recuperation purposes effective 1 January 2017. 2. In duty stations where the rest and recuperation frequency has been reduced, the new cycle takes effect immediately. In duty stations where the frequency of rest and recuperation has been prolonged (from 4 to 6 weeks, from 6 to 8 weeks or from 8 to 12 weeks) or where it has been discontinued, staff members or eligible individuals who have already started accruing qualifying service prior to 1 January 2017 may avail themselves of rest and recuperation after completing the period of qualifying service previously in effect. Upon the return of the staff member or other eligible individuals to the duty station, the new frequency shall apply. 3. Should security or severe hardship conditions improve or deteriorate at specific duty stations during the course of the year, the duration of the period of qualifying service (frequency) may be adjusted by the Office of Human Resources Management following inter-agency consultations.