Anti-Doping Convention
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WADA Technical Letter – TL07 ANDARINE
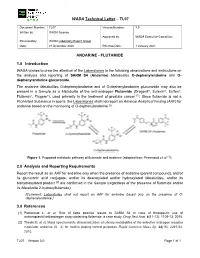
WADA Technical Letter – TL07 Document Number: TL07 Version Number: 3.0 Written by: WADA Science Approved by: WADA Executive Committee Reviewed by: WADA Laboratory Expert Group Date: 21 December 2020 Effective Date: 1 January 2021 ANDARINE - FLUTAMIDE 1.0 Introduction WADA wishes to draw the attention of the Laboratories to the following observations and instructions on the analysis and reporting of SARM S4 (Andarine) Metabolites O-dephenylandarine and O- dephenylandarine glucuronide. The andarine Metabolites O-dephenylandarine and of O-dephenylandarine glucuronide may also be present in a Sample as a Metabolite of the anti-androgen Flutamide (Drogenil®, Eulexin®, Euflex®, Flutamin®, Flugere®), used primarily in the treatment of prostate cancer [1]. Since flutamide is not a Prohibited Substance in sports, the Laboratories shall not report an Adverse Analytical Finding (AAF) for andarine based on the monitoring of O-dephenylandarine [2]. Figure 1. Proposed metabolic pathway of flutamide and andarine (adapted from Perrenoud et al. [1]). 2.0 Analysis and Reporting Requirements Report the result as an AAF for andarine only when the presence of andarine (parent compound), and/or its glucuronic acid conjugate, and/or its deacetylated and/or hydroxylated Metabolites, and/or its bishydroxylated product [2] are confirmed in the Sample (regardless of the presence of flutamide and/or its Metabolite 2-hydroxyflutamide); [Comment: Laboratories shall not report an AAF for andarine based only on the presence of O- dephenylandarine.] 3.0 References [1] Perrenoud L. et al. Risk of false positive results to SARM S4 in case of therapeutic use of antineoplastic/antiandrogen drug containing flutamide: a case study. -

DHEA | Medchemexpress
Inhibitors Product Data Sheet DHEA • Agonists Cat. No.: HY-14650 CAS No.: 53-43-0 Molecular Formula: C₁₉H₂₈O₂ • Molecular Weight: 288.42 Screening Libraries Target: Androgen Receptor; Endogenous Metabolite Pathway: Others; Metabolic Enzyme/Protease Storage: Please store the product under the recommended conditions in the Certificate of Analysis. SOLVENT & SOLUBILITY In Vitro DMSO : 50 mg/mL (173.36 mM; Need ultrasonic) Ethanol : 50 mg/mL (173.36 mM; Need ultrasonic) H2O : 1 mg/mL (3.47 mM; Need ultrasonic) Mass Solvent 1 mg 5 mg 10 mg Concentration Preparing 1 mM 3.4672 mL 17.3358 mL 34.6717 mL Stock Solutions 5 mM 0.6934 mL 3.4672 mL 6.9343 mL 10 mM 0.3467 mL 1.7336 mL 3.4672 mL Please refer to the solubility information to select the appropriate solvent. In Vivo 1. Add each solvent one by one: Cremophor EL Solubility: 14.29 mg/mL (49.55 mM); Clear solution; Need ultrasonic 2. Add each solvent one by one: 10% DMSO >> 40% PEG300 >> 5% Tween-80 >> 45% saline Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 3. Add each solvent one by one: 10% DMSO >> 90% (20% SBE-β-CD in saline) Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 4. Add each solvent one by one: 10% DMSO >> 90% corn oil Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 5. Add each solvent one by one: 10% EtOH >> 90% (20% SBE-β-CD in saline) Solubility: ≥ 2.5 mg/mL (8.67 mM); Clear solution 6. -

Benfluorex: What Use? a SECOND LOOK POOR ASSESSMENT FILE
New products necessitating blood transfusions 3- “Paclitaxel” Prescr Intern 1994; 3 (14): 164-165. Literature 4- Rowisky EK et al. “Phase I and pharmacolog- occurred in 37% of patients (9). ic study of topotecan: a novel topoisomerase I The most frequent non haematologi- Our literature search was based on systematic inhibitor” J Clin Oncol 1992; 10: 647-656. cal side effects were nausea (68.1% of scrutiny of contents listings of the main inter- 5- Verweij L et al. “Phase I and pharmacokinet- ics study of topotecan, a new topoisomerase I patients, severe in 6.1% of patients), national journals and Current Contents at inhibitor” Ann Oncol 1993; 4: 673-678. vomiting (44.3%, severe in 4.5%), hair the Prescrire library, and on reference texts 6- Saltz L et al. “Phase I clinical and pharmacol- in clinical pharmacology (Martindale The ogy study of topotecan given daily for 5 consecu- loss (56.9%), fatigue (44.5%, severe in Extra Pharmacopoeia 31st ed., etc.). We also tive days to patients with advanced solid tumors, 6%), diarrhoea (26.1%, severe in 3.4%), consulted CD-ROM versions of Medline (1981- with attempt at dose intensification using recom- and stomatitis (20.2%, severe in 2%) (9). March 1998), Embase Drugs and binant granulocyte colony-stimulating factor” J Pharmacology (1991-January 1998), Cochrane Natl Cancer Inst 1993; 85 (18): 1499-1507. Paclitaxel solution contains a solvent, 7- Kudelka AP et al. “Phase II study of intravenous Cremophor EL°, that is incompatible with (1998, issue 1), Medidoc (1991-1994) and topotecan as a 5-day infusion for refractory epithe- Reactions (1983-June 1997), and the Minitel lial ovarian carcinoma” J Clin Oncol 1996; 14: the use of PVC infusion devices and war- version of the Pascal database up to 1552-1557. -

AO-Klasifikácia Faktúr →Zlomeniny
AO-klasifikácia faktúr →zlomeniny. AOP-syndróm – skr. syndroma adipositas–oligomenorrhoea–parotis. aorta – [g. aorté srdcovnica] srdcovnica. Začína sa z ľavej komory a vystupuje kraniálne aţ do výšky 2. pravého sternokostálneho kĺbu ako aorta ascendens, pokračovaním je oblúk arcus aortae, aorta descendens, aorta thoracia a aorta abdominalis. Aorta ascendens – začína sa v ľavej komore nad polmesiačikovitými chlopňami a skoro celá sa nachádza v perikarde. Je dlhá asi 4 – 5 cm, jej priemer je 22 – 30 mm. Ihneď nad chlop-ňami je následkom spätných nárazov krvi mierne vydutá do tzv. sinus aortae, výraznejšie u starších osôb. Oddiely a. obsahujúce sinus aortae sa nazývajú bulbus aortae. U starších osôb býva následkom nárazov krvi širší aj koncový úsek vzostupnej a. pred jej prechodom do oblúka, tzv. sinus maximus (quartus) aortae. Tu býva u starších osôb a. často rozširená. A. ascendens, ako aj začiatok arcus aortae majú špeciálne vasa vasorum pochádzajúce z vencovitých tepien (aa. cardiaortales). Tento úsek osobitne patogeneticky rizikový. Začiatok aorta ascendens je ešte obalený vo vagina serosa arteriarum, kt. tvorí na ventrálnom obvode a. priečnu krkvu podloţenú subseróznym tukovým väzivom (Concatova-Bacceli tuková krkva). Vnútri vagina arteriarum je aorta ascendens a začiatrok a. pulmonalis spojené tuhým väzivom (vincula aortae Rindfleischi). Výstup aorta ascendens kryje spredu začiatok a. pulmonalis, ventrálne a vpravo je auricula dextra, dorzálne je uloţený r. dexter a. pulmonalis. Kraniálne vpravo od a. je v. cava superior, vľavo kmeň a. pulmonalis. Z ventrálneho a ľavého sinus aortae sa začína a. coronaria cordis dextra et sinistra. Aorta ascendens a arcus aortae Arcus aortae – je dlhý asi 6 cm, začína sa za sternom vo výške úponu 2. -

Effects of the Ghrelin Receptor Agonist Anamorelin
Garcia et al. Cancer & Metabolism 2014, 2(Suppl 1):P19 http://www.cancerandmetabolism.com/content/2/S1/P19 Cancer & Metabolism POSTERPRESENTATION Open Access Effects of the ghrelin receptor agonist anamorelin on lean body mass in cancer patients with cachexia; results from a Phase II randomized, double blind, multicenter study Jose M Garcia1,2, Ying Yan3, Elizabeth Manning-Duus3*, John Friend3 From Metabolism, Diet and Disease 2014: Cancer and metabolism Washington DC, USA. 28-30 May 2014 Background LBM and TBM in anamorelin-treated patients were Cancer anorexia-cachexia is a frequent, debilitating and strongly correlated (r2=0.7249, p< 0.0001). Anamorelin life-threatening condition in which altered metabolism treatment improvements in HGS and QoL were previously and reduced food intake contribute to weight loss presented [1]. Anamorelin was well tolerated, and types (mainly due to lean body mass [LBM] loss), which can- and prevalence of AEs were similar between treatment not be reverted by conventional nutritional support. arms. Safe/effective treatments for cancer cachexia remain an unmet need. The hunger hormone ghrelin has been Conclusion shown to activate key pathways in the regulation of Decreased body weight and LBM are poor prognostic fac- body composition. Anamorelin (ANAM) is a novel, tors in cancer cachexia patients. This study demonstrates selective, oral ghrelin receptor agonist with appetite- that 50mg anamorelin treatment for 12 weeks significantly enhancing and anabolic activity. Anamorelin is currently increased LBM, which largely contributed to the increases being investigated in phase III studies for the treatment in total body mass. Together with its appetite-enhancing of anorexia-cachexia in advanced non-small cell lung activity, these results support the further development of cancer (also known as the ROMANA program). -

Campro Catalog Stable Isotope
Introduction & Welcome Dear Valued Customer, We are pleased to present to you our Stable Isotopes Catalog which contains more than three thousand (3000) high quality labeled compounds. You will find new additions that are beneficial for your research. Campro Scientific is proud to work together with Isotec, Inc. for the distribution and marketing of their stable isotopes. We have been working with Isotec for more than twenty years and know that their products meet the highest standard. Campro Scientific was founded in 1981 and we provide services to some of the most prestigious universities, research institutes and laboratories throughout Europe. We are a research-oriented company specialized in supporting the requirements of the scientific community. We are the exclusive distributor of some of the world’s leading producers of research chemicals, radioisotopes, stable isotopes and environmental standards. We understand the requirements of our customers, and work every day to fulfill them. In working with us you are guaranteed to receive: - Excellent customer service - High quality products - Dependable service - Efficient distribution The highly educated staff at Campro’s headquarters and sales office is ready to assist you with your questions and product requirements. Feel free to call us at any time. Sincerely, Dr. Ahmad Rajabi General Manager 180/280 = unlabeled 185/285 = 15N labeled 181/281 = double labeled (13C+15N, 13C+D, 15N+18O etc.) 186/286 = 12C labeled 182/282 = d labeled 187/287 = 17O labeled 183/283 = 13C labeleld 188/288 = 18O labeled 184/284 = 16O labeled, 14N labeled 189/289 = Noble Gases Table of Contents Ordering Information.................................................................................................. page 4 - 5 Packaging Information .............................................................................................. -

Download Product Insert (PDF)
Product Information Boldenone Cypionate Item No. 15158 CAS Registry No.: 106505-90-2 O Formal Name: 17β-hydroxy-androsta-1,4-dien-3-one O cyclopentanepropionate MF: C27H38O3 FW: 410.6 H Purity: ≥95% Stability: ≥2 years at -20°C H H Supplied as: A crystalline solid λ O UV/Vis.: max: 244 nm Laboratory Procedures For long term storage, we suggest that boldenone cypionate be stored as supplied at -20°C. It should be stable for at least two years. Boldenone cypionate is supplied as a crystalline solid. A stock solution may be made by dissolving the boldenone cypionate in the solvent of choice. Boldenone cypionate is soluble in organic solvents such as ethanol, DMSO, and dimethyl formamide, which should be purged with an inert gas. The solubility of boldenone cypionate in these solvents is approximately 15, 5, and 25 mg/ml, respectively. Boldenone cypionate is sparingly soluble in aqueous buffers. For maximum solubility in aqueous buffers, boldenone cypionate should first be dissolved in ethanol and then diluted with the aqueous buffer of choice. Boldenone cypionate has a solubility of approximately 0.3 mg/ml in a 1:2 solution of ethanol:PBS (pH 7.2) using this method. We do not recommend storing the aqueous solution for more than one day. Boldenone is an anabolic androgenic steroid and synthetic derivative of testosterone that was originally developed for veterinary use.1 It can increase nitrogen retention, protein synthesis, and appetite, and also stimulates the release of erythropoietin in the kidneys.1 Boldenone cypionate was synthesized as an ester of boldenone in an attempt to alter boldenone’s very long half-life.2 Anabolic androgenic steroid compounds such as boldenone cypionate have been used illicitly by bodybuilders and other athletes.3 This compound is intended for forensic and research purposes only. -

Prohibited Substances Shall Be Considered As “Specified Substances” Except Substances in Classes S1, S2, S.4.4, S.4.5, S6.A, and Prohibited Methods M1, M2 and M3
BGBl. III - Ausgegeben am 27. Dezember 2019 - Nr. 237 1 von 8 THE 2020 PROHIBITED LIST - WORLD ANTI-DOPING CODE DATE OF ENTRY INTO FORCE: 1 JANUARY 2020 SUBSTANCES AND METHODS PROHIBITED AT ALL TIMES (IN- AND OUT-OF-COMPETITION) IN ACCORDANCE WITH ARTICLE 4.2.2 OF THE WORLD ANTI-DOPING CODE, ALL PROHIBITED SUBSTANCES SHALL BE CONSIDERED AS “SPECIFIED SUBSTANCES” EXCEPT SUBSTANCES IN CLASSES S1, S2, S.4.4, S.4.5, S6.A, AND PROHIBITED METHODS M1, M2 AND M3. PROHIBITED SUBSTANCES Androstenediol (androst-5-ene-3β,17β-diol); Androstenedione (androst-4-ene-3,17-dione); S0. NON-APPROVED SUBSTANCES Bolasterone; Boldenone; Any pharmacological substance which is not Boldione (androsta-1,4-diene-3,17-dione); addressed by any of the subsequent sections of Calusterone; the List and with no current approval by any Clostebol; governmental regulatory health authority for Danazol ([1,2]oxazolo[4',5':2,3]pregna-4-en- human therapeutic use (e.g. drugs under pre- 20-yn-17α-ol); clinical or clinical development or discontinued, Dehydrochlormethyltestosterone (4-chloro- designer drugs, substances approved only for 17β-hydroxy-17α-methylandrosta-1,4-dien-3- veterinary use) is prohibited at all times. one); Desoxymethyltestosterone (17α-methyl-5α- S1. ANABOLIC AGENTS androst-2-en-17β-ol); Drostanolone; Anabolic agents are prohibited. Epiandrosterone (3β-hydroxy-5α-androstan- …………………………………………………… 17-one); 1. ANABOLIC ANDROGENIC STEROIDS Epi-dihydrotestosterone (17β-hydroxy-5β- (AAS) androstan-3one); Epitestosterone; when administered exogenously, including but -

Drug Testing Program
DRUG TESTING PROGRAM Copyright © 2021 CrossFit, LLC. All Rights Reserved. CrossFit is a registered trademark ® of CrossFit, LLC. 2021 DRUG TESTING PROGRAM 2021 DRUG TESTING CONTENTS 1. DRUG-FREE COMPETITION 2. ATHLETE CONSENT 3. DRUG TESTING 4. IN-COMPETITION/OUT-OF-COMPETITION DRUG TESTING 5. REGISTERED ATHLETE TESTING POOL (OUT-OF-COMPETITION DRUG TESTING) 6. REMOVAL FROM TESTING POOL/RETIREMENT 6A. REMOVAL FROM TESTING POOL/WATCH LIST 7. TESTING POOL REQUIREMENTS FOLLOWING A SANCTION 8. DRUG TEST NOTIFICATION AND ADMINISTRATION 9. SPECIMEN ANALYSIS 10. REPORTING RESULTS 11. DRUG TESTING POLICY VIOLATIONS 12. ENFORCEMENT/SANCTIONS 13. APPEALS PROCESS 14. LEADERBOARD DISPLAY 15. EDUCATION 16. DIETARY SUPPLEMENTS 17. TRANSGENDER POLICY 18. THERAPEUTIC USE EXEMPTION APPENDIX A: 2020-2021 CROSSFIT BANNED SUBSTANCE CLASSES APPENDIX B: CROSSFIT URINE TESTING PROCEDURES - (IN-COMPETITION) APPENDIX C: TUE APPLICATION REQUIREMENTS Drug Testing Policy V4 Copyright © 2021 CrossFit, LLC. All Rights Reserved. CrossFit is a registered trademark ® of CrossFit, LLC. [ 2 ] 2021 DRUG TESTING PROGRAM 2021 DRUG TESTING 1. DRUG-FREE COMPETITION As the world’s definitive test of fitness, CrossFit Games competitions stand not only as testaments to the athletes who compete but to the training methodologies they use. In this arena, a true and honest comparison of training practices and athletic capacity is impossible without a level playing field. Therefore, the use of banned performance-enhancing substances is prohibited. Even the legal use of banned substances, such as physician-prescribed hormone replacement therapy or some over-the-counter performance-enhancing supplements, has the potential to compromise the integrity of the competition and must be disallowed. With the health, safety, and welfare of the athletes, and the integrity of our sport as top priorities, CrossFit, LLC has adopted the following Drug Testing Policy to ensure the validity of the results achieved in competition. -

UFC PROHIBITED LIST Effective June 1, 2021 the UFC PROHIBITED LIST
UFC PROHIBITED LIST Effective June 1, 2021 THE UFC PROHIBITED LIST UFC PROHIBITED LIST Effective June 1, 2021 PART 1. Except as provided otherwise in PART 2 below, the UFC Prohibited List shall incorporate the most current Prohibited List published by WADA, as well as any WADA Technical Documents establishing decision limits or reporting levels, and, unless otherwise modified by the UFC Prohibited List or the UFC Anti-Doping Policy, Prohibited Substances, Prohibited Methods, Specified or Non-Specified Substances and Specified or Non-Specified Methods shall be as identified as such on the WADA Prohibited List or WADA Technical Documents. PART 2. Notwithstanding the WADA Prohibited List and any otherwise applicable WADA Technical Documents, the following modifications shall be in full force and effect: 1. Decision Concentration Levels. Adverse Analytical Findings reported at a concentration below the following Decision Concentration Levels shall be managed by USADA as Atypical Findings. • Cannabinoids: natural or synthetic delta-9-tetrahydrocannabinol (THC) or Cannabimimetics (e.g., “Spice,” JWH-018, JWH-073, HU-210): any level • Clomiphene: 0.1 ng/mL1 • Dehydrochloromethyltestosterone (DHCMT) long-term metabolite (M3): 0.1 ng/mL • Selective Androgen Receptor Modulators (SARMs): 0.1 ng/mL2 • GW-1516 (GW-501516) metabolites: 0.1 ng/mL • Epitrenbolone (Trenbolone metabolite): 0.2 ng/mL 2. SARMs/GW-1516: Adverse Analytical Findings reported at a concentration at or above the applicable Decision Concentration Level but under 1 ng/mL shall be managed by USADA as Specified Substances. 3. Higenamine: Higenamine shall be a Prohibited Substance under the UFC Anti-Doping Policy only In-Competition (and not Out-of- Competition). -

Pharmacological Modulation of Ghrelin to Induce Weight Loss: Successes and Challenges
Current Diabetes Reports (2019) 19:102 https://doi.org/10.1007/s11892-019-1211-9 OBESITY (KM GADDE, SECTION EDITOR) Pharmacological Modulation of Ghrelin to Induce Weight Loss: Successes and Challenges Martha A. Schalla1 & Andreas Stengel1,2 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of Review Obesity is affecting over 600 million adults worldwide and has numerous negative effects on health. Since ghrelin positively regulates food intake and body weight, targeting its signaling to induce weight loss under conditions of obesity seems promising. Thus, the present work reviews and discusses different possibilities to alter ghrelin signaling. Recent Findings Ghrelin signaling can be altered by RNA Spiegelmers, GHSR/Fc, ghrelin-O-acyltransferase inhibitors as well as antagonists, and inverse agonists of the ghrelin receptor. PF-05190457 is the first inverse agonist of the ghrelin receptor tested in humans shown to inhibit growth hormone secretion, gastric emptying, and reduce postprandial glucose levels. Effects on body weight were not examined. Summary Although various highly promising agents targeting ghrelin signaling exist, so far, they were mostly only tested in vitro or in animal models. Further research in humans is thus needed to further assess the effects of ghrelin antagonism on body weight especially under conditions of obesity. Keywords Antagonist . Ghrelin-O-acyl transferase . GOAT . Growth hormone . Inverse agonist . Obesity Abbreviations GHRP-2 Growth hormone–releasing peptide-2 ACTH Adrenocorticotropic hormone GHRP-6 Growth hormone–releasing peptide 6 AZ-GHS-22 Non-CNS penetrant inverse agonist 22 GHSR Growth hormone secretagogue receptor AZ-GHS-38 CNS penetrant inverse agonist 38 GOAT Ghrelin-O-acyltransferase BMI Body mass index GRLN-R Ghrelin receptor CpdB Compound B icv Intracerebroventricular CpdD Compound D POMC Proopiomelanocortin DIO Diet-induced obesity sc Subcutaneous GH Growth hormone SPM RNA Spiegelmer WHO World Health Organization. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used