Part I Biopharmaceuticals
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WADA Technical Letter – TL07 ANDARINE
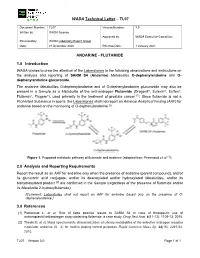
WADA Technical Letter – TL07 Document Number: TL07 Version Number: 3.0 Written by: WADA Science Approved by: WADA Executive Committee Reviewed by: WADA Laboratory Expert Group Date: 21 December 2020 Effective Date: 1 January 2021 ANDARINE - FLUTAMIDE 1.0 Introduction WADA wishes to draw the attention of the Laboratories to the following observations and instructions on the analysis and reporting of SARM S4 (Andarine) Metabolites O-dephenylandarine and O- dephenylandarine glucuronide. The andarine Metabolites O-dephenylandarine and of O-dephenylandarine glucuronide may also be present in a Sample as a Metabolite of the anti-androgen Flutamide (Drogenil®, Eulexin®, Euflex®, Flutamin®, Flugere®), used primarily in the treatment of prostate cancer [1]. Since flutamide is not a Prohibited Substance in sports, the Laboratories shall not report an Adverse Analytical Finding (AAF) for andarine based on the monitoring of O-dephenylandarine [2]. Figure 1. Proposed metabolic pathway of flutamide and andarine (adapted from Perrenoud et al. [1]). 2.0 Analysis and Reporting Requirements Report the result as an AAF for andarine only when the presence of andarine (parent compound), and/or its glucuronic acid conjugate, and/or its deacetylated and/or hydroxylated Metabolites, and/or its bishydroxylated product [2] are confirmed in the Sample (regardless of the presence of flutamide and/or its Metabolite 2-hydroxyflutamide); [Comment: Laboratories shall not report an AAF for andarine based only on the presence of O- dephenylandarine.] 3.0 References [1] Perrenoud L. et al. Risk of false positive results to SARM S4 in case of therapeutic use of antineoplastic/antiandrogen drug containing flutamide: a case study. -

New Rules Pertaining to the Banning of Anabolic Steroids in the Western Australian Harness Racing Industry to Be Introduced 1St September 2014
NEW RULES PERTAINING TO THE BANNING OF ANABOLIC STEROIDS IN THE WESTERN AUSTRALIAN HARNESS RACING INDUSTRY TO BE INTRODUCED 1ST SEPTEMBER 2014 Notice is hereby given that the Board of Racing and Wagering WA have resolved that the RWWA Rules of Harness Racing 2004 be amended. In accordance with section 45 (1) (b) of the Racing and Wagering Western Australia Act 2003 the Board of Racing and Wagering WA on the 10th April 2014 resolved that these amendments be adopted accordingly into the RWWA Rules of Harness Racing. The Harness Racing Board had advised of these amendments and the RWWA Board has determined that these amendments will come into effect on 1st September 2014. The details of the relevant rules pertaining to this ban of anabolic steroids for reference can be found following this advice. There are many implications arising from the introduction of these rules, and to assist trainers and veterinarians to comply with the new rules the following explanatory statement has been prepared. Which steroids are banned under these rules? The new rules ban the use of "anabolic androgenic steroids" in Standardbred horses at any time from birth until retirement. "Anabolic androgenic steroids" include those that are currently registered in Australia by the APVMA for use in horses, such as boldenone, ethylestrenol (in Nitrotain), methandriol, nandrolone, stanozolol and testosterone. Exogenous anabolic androgenic steroids that are banned also include but are not limited to those listed in the WADA prohibited list, such as 1-androstenediol; 1-androstenedione; -

IJCB 42B(1) 166-172.Pdf
Indian Journal of Chemistry Vol. 42B, January 2003, pp. 166-172 Synthesis and biological activity of 16-arylidene derivatives of estrone and estrone methyl ether Maninder Minu* & Dharam Paul lindal University In 5titutc of Pharmaceutical Sciences, Panjab University, Chandigarh 160014, India and G Leclercq & M Borras institut Jules Bordet, Association Hospitaliere de Bruxelles. Centre des Tumeurs de I'ULB, Rue Heger-Bordet 1- 1000, Belgiulll Received 24 April 200 I .. accepted (revised) 20 March 2002 The synthesis of 16-arylidene derivatives 3, 4, S, 6, 7. 8. 9, 10, 11, 12, 13, 14 and IS is described. These compounds have been tested at NCI, Bethesda, for their antineoplastic acti vity against the cell panel consisting of 60-ce!l lines and th e compounds 3, 4, S, 6 and 7 have also been tested for their ill vitro estrogenic / antiestrogenic activity; induction of ERE dependent luciferase inductio n was measured (MvLN celis). The formation of active steroids by aromatase has It was conceived that selective inhibitors of aroma been considered to play an important role in the de tase might be useful as a pharmacological tool to de velopment of human breast carcinoma t, at least one vice successful treatment approach for the hormonal third of all breast cancers establishing that. the estro dependent breast cancer. Our efforts were focused on gen-dependent carcinoma regresses following estro designing estrogen and estrogen methyl ether deriva 2 gen deprivation . In the postmenopausal women, the tives that might inhibit or possess antiestrogenic activ production of estrogen takes place in peripheral tissue ity. From these efforts, several 16-arylidine deriva 3 from inactive precursors by the action of aromatase . -

Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals
Journal of Clinical Medicine Review Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals Carlotta Cocchetti 1, Jiska Ristori 1, Alessia Romani 1, Mario Maggi 2 and Alessandra Daphne Fisher 1,* 1 Andrology, Women’s Endocrinology and Gender Incongruence Unit, Florence University Hospital, 50139 Florence, Italy; [email protected] (C.C); jiska.ristori@unifi.it (J.R.); [email protected] (A.R.) 2 Department of Experimental, Clinical and Biomedical Sciences, Careggi University Hospital, 50139 Florence, Italy; [email protected]fi.it * Correspondence: fi[email protected] Received: 16 April 2020; Accepted: 18 May 2020; Published: 26 May 2020 Abstract: Introduction: To date no standardized hormonal treatment protocols for non-binary transgender individuals have been described in the literature and there is a lack of data regarding their efficacy and safety. Objectives: To suggest possible treatment strategies for non-binary transgender individuals with non-standardized requests and to emphasize the importance of a personalized clinical approach. Methods: A narrative review of pertinent literature on gender-affirming hormonal treatment in transgender persons was performed using PubMed. Results: New hormonal treatment regimens outside those reported in current guidelines should be considered for non-binary transgender individuals, in order to improve psychological well-being and quality of life. In the present review we suggested the use of hormonal and non-hormonal compounds, which—based on their mechanism of action—could be used in these cases depending on clients’ requests. Conclusion: Requests for an individualized hormonal treatment in non-binary transgender individuals represent a future challenge for professionals managing transgender health care. For each case, clinicians should balance the benefits and risks of a personalized non-standardized treatment, actively involving the person in decisions regarding hormonal treatment. -

Classification and Pharmacology of Progestins
Maturitas 46S1 (2003) S7–S16 Classification and pharmacology of progestins Adolf E. Schindler a,∗, Carlo Campagnoli b, René Druckmann c, Johannes Huber d, Jorge R. Pasqualini e, Karl W. Schweppe f, Jos H. H. Thijssen g a Institut für Medizinische Forschung und Fortbildung, Universitätsklinikum, Hufelandstr. 55, Essen 45147, Germany b Ospedale Ginecologico St. Anna, Corso Spezia 60, 10126 Torino, Italy c Ameno-Menopause-Center, 12, Rue de France, 06000 Nice, France d Abt. für Gynäkologische Endokrinologie, AKH Wien, Währingergürtel 18-20, 1090 Wien, Austria e Institute de Puériculture26, Boulevard Brune, 75014 Paris, France f Abt. für Gynäkologie und Geburtshilfe, Ammerland Klinik, Langestr.38, 26622 Westerstede, Germany g Department of Endocrinology, Universitair Medisch Centrum Utrecht, P.O. Box 85090, 3508 AB Utrecht, The Netherlands Abstract Besides the natural progestin, progesterone, there are different classes of progestins, such as retroprogesterone (i.e. dydroges- terone), progesterone derivatives (i.e. medrogestone) 17␣-hydroxyprogesterone derivatives (i.e. chlormadinone acetate, cypro- terone acetate, medroxyprogesterone acetate, megestrol acetate), 19-norprogesterone derivatives (i.e. nomegestrol, promege- stone, trimegestone, nesterone), 19-nortestosterone derivatives norethisterone (NET), lynestrenol, levonorgestrel, desogestrel, gestodene, norgestimate, dienogest) and spironolactone derivatives (i.e. drospirenone). Some of the synthetic progestins are prodrugs, which need to be metabolized to become active compounds. Besides -

Medicines Regulations 1984 (SR 1984/143)
Reprint as at 1 July 2014 Medicines Regulations 1984 (SR 1984/143) David Beattie, Governor-General Order in Council At the Government House at Wellington this 5th day of June 1984 Present: His Excellency the Governor-General in Council Pursuant to section 105 of the Medicines Act 1981, and, in the case of Part 3 of the regulations, to section 62 of that Act, His Excellency the Governor-General, acting on the advice of the Minister of Health tendered after consultation with the organisations and bodies that ap- peared to the Minister to be representatives of persons likely to be substantially affected, and by and with the advice and consent of the Executive Council, hereby makes the following regulations. Contents Page 1 Title and commencement 5 Note Changes authorised by subpart 2 of Part 2 of the Legislation Act 2012 have been made in this official reprint. Note 4 at the end of this reprint provides a list of the amendments incorporated. These regulations are administered by the Ministry of Health. 1 Reprinted as at Medicines Regulations 1984 1 July 2014 2 Interpretation 5 Part 1 Classification of medicines 3 Classification of medicines 11 Part 2 Standards 4 Standards for medicines, related products, medical 11 devices, cosmetics, and surgical dressings 5 Pharmacist may dilute medicine in particular case 12 6 Colouring substances [Revoked] 12 Part 3 Advertisements 7 Advertisements not to claim official approval 13 8 Advertisements for medicines 13 9 Advertisements for related products 15 10 Advertisements for medical devices 15 11 Advertisements -

The In¯Uence of Medication on Erectile Function
International Journal of Impotence Research (1997) 9, 17±26 ß 1997 Stockton Press All rights reserved 0955-9930/97 $12.00 The in¯uence of medication on erectile function W Meinhardt1, RF Kropman2, P Vermeij3, AAB Lycklama aÁ Nijeholt4 and J Zwartendijk4 1Department of Urology, Netherlands Cancer Institute/Antoni van Leeuwenhoek Hospital, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands; 2Department of Urology, Leyenburg Hospital, Leyweg 275, 2545 CH The Hague, The Netherlands; 3Pharmacy; and 4Department of Urology, Leiden University Hospital, P.O. Box 9600, 2300 RC Leiden, The Netherlands Keywords: impotence; side-effect; antipsychotic; antihypertensive; physiology; erectile function Introduction stopped their antihypertensive treatment over a ®ve year period, because of side-effects on sexual function.5 In the drug registration procedures sexual Several physiological mechanisms are involved in function is not a major issue. This means that erectile function. A negative in¯uence of prescrip- knowledge of the problem is mainly dependent on tion-drugs on these mechanisms will not always case reports and the lists from side effect registries.6±8 come to the attention of the clinician, whereas a Another way of looking at the problem is drug causing priapism will rarely escape the atten- combining available data on mechanisms of action tion. of drugs with the knowledge of the physiological When erectile function is in¯uenced in a negative mechanisms involved in erectile function. The way compensation may occur. For example, age- advantage of this approach is that remedies may related penile sensory disorders may be compen- evolve from it. sated for by extra stimulation.1 Diminished in¯ux of In this paper we will discuss the subject in the blood will lead to a slower onset of the erection, but following order: may be accepted. -

Ranvet's Filybol
Ranvet's Filybol Ranvet Chemwatch Hazard Alert Code: 2 Chemwatch: 4787-83 Issue Date: 08/02/2016 Version No: 5.1.1.1 Print Date: 10/28/2016 Safety Data Sheet according to WHS and ADG requirements S.GHS.AUS.EN SECTION 1 IDENTIFICATION OF THE SUBSTANCE / MIXTURE AND OF THE COMPANY / UNDERTAKING Product Identifier Product name Ranvet's Filybol Chemical Name peanut oil Synonyms Not Available Other means of Not Available identification Relevant identified uses of the substance or mixture and uses advised against Relevant identified Non-virilising anabolic combination for fillies, mares, colts and stallions. uses Details of the supplier of the safety data sheet Registered company Ranvet name Address 10-12 Green Street Banksmeadow NSW 2019 Australia Telephone +61 2 9666 1744 Fax +61 2 9666 1755 Website https://www.ranvet.com.au/other_msds.htm Email [email protected] Emergency telephone number Association / Not Available Organisation Emergency telephone +61 425 061 584 numbers Other emergency Not Available telephone numbers SECTION 2 HAZARDS IDENTIFICATION Classification of the substance or mixture Poisons Schedule S4 Carcinogenicity Category 2, Reproductive Toxicity Category 2, Acute Aquatic Hazard Category 2, Chronic Aquatic Hazard Classification [1] Category 2 1. Classified by Chemwatch; 2. Classification drawn from HSIS ; 3. Classification drawn from EC Directive 1272/2008 - Annex Legend: VI Label elements GHS label elements SIGNAL WORD WARNING Continued... Chemwatch: 4787-83 Page 2 of 10 Issue Date: 08/02/2016 Version No: 5.1.1.1 Ranvet's Filybol Print Date: 10/28/2016 Hazard statement(s) H351 Suspected of causing cancer. H361 Suspected of damaging fertility or the unborn child. -

Effects of Androgenic-Anabolic Steroids on Apolipoproteins and Lipoprotein (A) F Hartgens, G Rietjens, H a Keizer, H Kuipers, B H R Wolffenbuttel
253 Br J Sports Med: first published as 10.1136/bjsm.2003.000199 on 21 May 2004. Downloaded from ORIGINAL ARTICLE Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a) F Hartgens, G Rietjens, H A Keizer, H Kuipers, B H R Wolffenbuttel ............................................................................................................................... Br J Sports Med 2004;38:253–259. doi: 10.1136/bjsm.2003.000199 Objectives: To investigate the effects of two different regimens of androgenic-anabolic steroid (AAS) administration on serum lipid and lipoproteins, and recovery of these variables after drug cessation, as indicators of the risk for cardiovascular disease in healthy male strength athletes. Methods: In a non-blinded study (study 1) serum lipoproteins and lipids were assessed in 19 subjects who self administered AASs for eight or 14 weeks, and in 16 non-using volunteers. In a randomised double blind, placebo controlled design, the effects of intramuscular administration of nandrolone decanoate (200 mg/week) for eight weeks on the same variables in 16 bodybuilders were studied (study 2). Fasting serum concentrations of total cholesterol, triglycerides, HDL-cholesterol (HDL-C), HDL2-cholesterol (HDL2- C), HDL3-cholesterol (HDL3-C), apolipoprotein A1 (Apo-A1), apolipoprotein B (Apo-B), and lipoprotein (a) (Lp(a)) were determined. Results: In study 1 AAS administration led to decreases in serum concentrations of HDL-C (from 1.08 (0.30) to 0.43 (0.22) mmol/l), HDL2-C (from 0.21 (0.18) to 0.05 (0.03) mmol/l), HDL3-C (from 0.87 (0.24) to 0.40 (0.20) mmol/l, and Apo-A1 (from 1.41 (0.27) to 0.71 (0.34) g/l), whereas Apo-B increased from 0.96 (0.13) to 1.32 (0.28) g/l. -

UFC PROHIBITED LIST Effective June 1, 2021 the UFC PROHIBITED LIST
UFC PROHIBITED LIST Effective June 1, 2021 THE UFC PROHIBITED LIST UFC PROHIBITED LIST Effective June 1, 2021 PART 1. Except as provided otherwise in PART 2 below, the UFC Prohibited List shall incorporate the most current Prohibited List published by WADA, as well as any WADA Technical Documents establishing decision limits or reporting levels, and, unless otherwise modified by the UFC Prohibited List or the UFC Anti-Doping Policy, Prohibited Substances, Prohibited Methods, Specified or Non-Specified Substances and Specified or Non-Specified Methods shall be as identified as such on the WADA Prohibited List or WADA Technical Documents. PART 2. Notwithstanding the WADA Prohibited List and any otherwise applicable WADA Technical Documents, the following modifications shall be in full force and effect: 1. Decision Concentration Levels. Adverse Analytical Findings reported at a concentration below the following Decision Concentration Levels shall be managed by USADA as Atypical Findings. • Cannabinoids: natural or synthetic delta-9-tetrahydrocannabinol (THC) or Cannabimimetics (e.g., “Spice,” JWH-018, JWH-073, HU-210): any level • Clomiphene: 0.1 ng/mL1 • Dehydrochloromethyltestosterone (DHCMT) long-term metabolite (M3): 0.1 ng/mL • Selective Androgen Receptor Modulators (SARMs): 0.1 ng/mL2 • GW-1516 (GW-501516) metabolites: 0.1 ng/mL • Epitrenbolone (Trenbolone metabolite): 0.2 ng/mL 2. SARMs/GW-1516: Adverse Analytical Findings reported at a concentration at or above the applicable Decision Concentration Level but under 1 ng/mL shall be managed by USADA as Specified Substances. 3. Higenamine: Higenamine shall be a Prohibited Substance under the UFC Anti-Doping Policy only In-Competition (and not Out-of- Competition). -

NINDS Custom Collection II
ACACETIN ACEBUTOLOL HYDROCHLORIDE ACECLIDINE HYDROCHLORIDE ACEMETACIN ACETAMINOPHEN ACETAMINOSALOL ACETANILIDE ACETARSOL ACETAZOLAMIDE ACETOHYDROXAMIC ACID ACETRIAZOIC ACID ACETYL TYROSINE ETHYL ESTER ACETYLCARNITINE ACETYLCHOLINE ACETYLCYSTEINE ACETYLGLUCOSAMINE ACETYLGLUTAMIC ACID ACETYL-L-LEUCINE ACETYLPHENYLALANINE ACETYLSEROTONIN ACETYLTRYPTOPHAN ACEXAMIC ACID ACIVICIN ACLACINOMYCIN A1 ACONITINE ACRIFLAVINIUM HYDROCHLORIDE ACRISORCIN ACTINONIN ACYCLOVIR ADENOSINE PHOSPHATE ADENOSINE ADRENALINE BITARTRATE AESCULIN AJMALINE AKLAVINE HYDROCHLORIDE ALANYL-dl-LEUCINE ALANYL-dl-PHENYLALANINE ALAPROCLATE ALBENDAZOLE ALBUTEROL ALEXIDINE HYDROCHLORIDE ALLANTOIN ALLOPURINOL ALMOTRIPTAN ALOIN ALPRENOLOL ALTRETAMINE ALVERINE CITRATE AMANTADINE HYDROCHLORIDE AMBROXOL HYDROCHLORIDE AMCINONIDE AMIKACIN SULFATE AMILORIDE HYDROCHLORIDE 3-AMINOBENZAMIDE gamma-AMINOBUTYRIC ACID AMINOCAPROIC ACID N- (2-AMINOETHYL)-4-CHLOROBENZAMIDE (RO-16-6491) AMINOGLUTETHIMIDE AMINOHIPPURIC ACID AMINOHYDROXYBUTYRIC ACID AMINOLEVULINIC ACID HYDROCHLORIDE AMINOPHENAZONE 3-AMINOPROPANESULPHONIC ACID AMINOPYRIDINE 9-AMINO-1,2,3,4-TETRAHYDROACRIDINE HYDROCHLORIDE AMINOTHIAZOLE AMIODARONE HYDROCHLORIDE AMIPRILOSE AMITRIPTYLINE HYDROCHLORIDE AMLODIPINE BESYLATE AMODIAQUINE DIHYDROCHLORIDE AMOXEPINE AMOXICILLIN AMPICILLIN SODIUM AMPROLIUM AMRINONE AMYGDALIN ANABASAMINE HYDROCHLORIDE ANABASINE HYDROCHLORIDE ANCITABINE HYDROCHLORIDE ANDROSTERONE SODIUM SULFATE ANIRACETAM ANISINDIONE ANISODAMINE ANISOMYCIN ANTAZOLINE PHOSPHATE ANTHRALIN ANTIMYCIN A (A1 shown) ANTIPYRINE APHYLLIC -

A Review of Mastalgia in Patients with Fibrocystic Breast Changes and the Non-Surgical Treatment Options
REVIEW ARTICLE A Review of Mastalgia in Patients with Fibrocystic Breast Changes and the Non-Surgical Treatment Options Khalid Rida Murshid FRCS(C), FACS Department of Surgery, College of Medicine, Taibah University, Al Madinah Al Munawwarah, Kingdom of Saudi Arabia Abstract Objectives The objectives of this study are to review fibrocystic changes of the breast, their causal and associated factors and their correlation to mastalgia, and then to review the available treatment options for mastalgia (caused by fibrocystic changes) short of surgery. Methods The author reviews all the articles obtained from a PubMed research on mastalgia and fibrocystic changes of the breast, published in English over the last 14 years. Results Fibrocystic changes of the breast are common and can be considered as a normal phase of breast development. These changes are sometimes asymptomatic; however, when painful, patients would seek medical advice. Lifestyle changes and the avoidance of certain dietary elements as well as the use of some non-pharmacological agents have shown some beneficiary effects. In severe cases, stronger pharmacological and hormonal agents are resorted to being more effective but are associated with greater side effects. Conclusion Fibrocystic changes of the breast are common and should not be considered a disease. When painful, reassurance and non-pharmacological measures should be used first as a treatment. Stronger pharmacological and hormonal agents hold more serious side effects. Some of these remedies are supported by good clinical evidence, while others are not. The ideal treatment for mastalgia caused by fibrocystic changes is to be identified by sound recent randomized controlled clinical studies on simple remedies before being performed on stronger ones.