MCSP Madagascar Annual Report Y4 01 October 2017 – 30 September 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Memoire : Master En Physique Et Applications
UNIVERSITE D’ANTANANARIVO DOMAINE SCIENCES ET TECHNOLOGIES MENTION PHYSIQUE ET APPLICATIONS PARCOUR S EN INGENIERIE EN ENERGIES RENOUVELABLES MEMOIRE : MASTER EN PHYSIQUE ET APPLICATIONS E LECTRIFICATION DU VILLAGE D ’ANTSATSAKA PAR ÉNERGIES RENOUVELABLES ET REALISATION DE COMMANDE D’ELECTRIFICATION PAR MICROCONTROLEUR Présenté par : NOVY FLAVIE Membres du jury Président de jury : Mme RANDRIAMANANTANY Zely Arivelo Professeur Titulaire Rapporteur : M. RAMANANTSOA Ravo Maître de Conférences Examinateur : Mme RAKOTO JOSEPH Onimihamina Maître de Conférences : M.RASAMIMANANA François de Salle Maître de Conférences 27 Octobre 2016 Mémoire pour l’obtention du diplôme de Master d’Ingénierie en Energie Renouvelable Mémoire pour l’obtention du diplôme de Master d’Ingénierie en Energie Renouvelable UNIVERSITE D’ANTANANARIVO DOMAINE SCIENCES ET TECHNOLOGIES MENTION PHYSIQUE ET APPLICATIONS PARCOUR S EN INGENIERIE EN ENERGIES RENOUVELABLES MEMOIRE : MASTER EN PHYSIQUE ET APPLICATIONS ELECTRIFICATION DU VILLAGE D ’ANTSATSAKA PAR ÉNERGIES RENOUVELABLES ET REALISATION DE COMMANDE D’ELECTRIFICATION PAR MICROCONTROLEUR Présenté par : NOVY FLAVIE Membres du jury Président de jury : Mme RANDRIAMANANTANY Zely Arivelo Professeur Titulaire Rapporteur : M. RAMANANTSOA Ravo Maître de Conférences Examinateur : Mme RAKOTO JOSEPH Onimihamina Maître de Conférences : M.RASAMIMANANA François de Salle Maître de Conférences RAZANAMANAMPISOA Harimalala Mémoire pour l’obtention du diplôme de Master d’Ingénierie en Energie Renouvelable REMERCIEMENTS Tout particulièrement, je tiens à exprimer mes vifs remerciements : A Monsieur RAHERIMANDIMBY Marson Professeur titulaire, Responsable de domaine science et technologie, de m’avoir acceptée en tant qu’étudiante au sein de la faculté des sciences. A Monsieur RAKOTONDRAMIHARANA Hery Tiana, Docteur Habilité à diriger des Recherches, Responsable de la mention. A Madame RAMANANTANY Zely Arivelo Professeur Titulaire, qui a bien voulu accorder l’honneur de présider le jury de ma soutenance. -

Description of 11 New Astiella (Spermacoceae, Rubiaceae) Species Endemic to Madagascar
European Journal of Taxonomy 312: 1–40 ISSN 2118-9773 https://doi.org/10.5852/ejt.2017.312 www.europeanjournaloftaxonomy.eu 2017 · GROENINCKX I. et al. This work is licensed under a Creative Commons Attribution 3.0 License. Research article Description of 11 new Astiella (Spermacoceae, Rubiaceae) species endemic to Madagascar Inge GROENINCKX 1, Steven JANSSENS 2, Erik SMETS 3 & Brecht VERSTRAETE 4,* 1 Plant Conservation and Population Biology, KU Leuven, Kasteelpark Arenberg 31, P.O. Box 2435, 3001 Leuven, Belgium. 2 Botanic Garden Meise, Nieuwelaan 38, 1860 Meise, Belgium. 3 Naturalis Biodiversity Center, P.O. Box 9517, 2300 RA Leiden, The Netherlands. 4 Natural History Museum of Denmark, University of Copenhagen, Sølvgade 83S, 1307 Copenhagen, Denmark. 1 Email: [email protected] 2 Email: [email protected] 3 Email: [email protected] * Corresponding author: [email protected] Abstract. Astiella is an herbaceous genus endemic to Madagascar, originally described with a single species A. delicatula Jovet. Molecular and morphological evidence place it in the tribe Spermacoceae s. lat. of Rubiaceae. During herbarium studies and fieldwork in Madagascar, 11 new Astiella species were identified and these are described here: A. antongilensis Groeninckx sp. nov., A. antsalovansis Groeninckx sp. nov., A. confusa Groeninckx sp. nov., A. deblockiae Groeninckx sp. nov., A. desseinii Groeninckx sp. nov., A. homolleae Groeninckx sp. nov., A. latifolia Groeninckx sp. nov., A. longifimbria Groeninckx sp. nov., A. perrieri Groeninckx sp. nov., A. pulla Groeninckx sp. nov., and A. tsaratanensis Groeninckx sp. nov. The genus Astiella now holds 12 species in total that are all endemic to Madagascar. -

Annual Report 2019
© Sam Cotton, Bristol Zoo Gardens ANNUAL REPORT 2019 A MESSAGE FROM THE AEECL PRESIDENT It seems strange to be looking back a year after the awful events that 2020 has seen so far and with the full horror of the coronavirus epidemic sweeping across the globe. However, this report focuses on the AEECL activities in 2019 so I will mainly concentrate on the progress we made last year within the Sahamalaza National Park. Our biggest challenge in 2019 was replacing the AEECL truck. For those of you who have been lucky enough to visit this area of Madagascar you would be only too aware of the severe restrictions on travelling due to the poor infrastructure of the roads between the villages and main cities. Without our trusty 4x4 to get AEECL team members from A to B we would not be able to carry out our vital work and with little funds available for such purchases we had no choice but to turn to our wonderful members and the wider zoo community. We were so delighted and grateful to get such a fantastic response and we are so indebted to those collections that have helped us keep mobile by funding a new truck. Thank you so much to Opel Zoo, Mulhouse Zoological & Botanical Park, Zoo La Palmyre, Zoo Heidelberg, Zoological Society of East Anglia, Parc Merveilleux, Zoological Society of Hertfordshire and to our major donator Wilhelma Zoo. 2019 also saw the continuation of the new Ankarafa Field Station construction. This will be an amazing upgrade to the facilities of the AEECL and is being generously supported by Bristol Zoo Gardens in the UK. -

Liste Candidatures Conseillers Diana
NOMBRE DISTRICT COMMUNE ENTITE NOM ET PRENOM(S) CANDIDATS CANDIDATS INDEPENDANT ROLIN TOMBORAVO (ROLIN AMBANJA AMBALAHONKO 1 ROLIN Tomboravo TOMBORAVO) INDEPENDANT IDAHO TSIAVIKY ERNEST (Idaho AMBANJA AMBALAHONKO 1 IDAHO Tsiaviky Ernest Tsiaviky Ernest) GROUPEMENT DE P.P IRK (Isika Rehetra AMBANJA AMBALAHONKO 1 RAMAROSON Soloniaina Justin Kaominina) AMBANJA AMBALIHA 1 SAIDALY SOFO (Saidaly Sofo) SAIDALY Sofo GROUPEMENT DE P.P ANTOKO MAITSO AMBANJA AMBALIHA 1 RIVOZARA (ANTOKO MAITSO) GROUPEMENT DE P.P MMM (Malagasy Miara AMBANJA AMBALIHA 1 ABDOUL Enzize Miainga) GROUPEMENT DE P.P IRK (Isika Rehetra AMBANJA AMBALIHA 1 TREFINDRAZANA Wilfried Jean Eduardo Jaoravo Kaominina) INDEPENDANT NASSIMO ABDOU (NASSIMO AMBANJA AMBANJA 1 NASSIMO Abdou ABDOU) INDEPENDANT INDEPENDANT RAZAFINIMANANA ANDRIAMAMPIONINA AMBANJA AMBANJA 1 RAZAFINIMANANA Andriamampionina Elysée ELYSEE (Razafimanana Andriamampianina Elysee) INDEPENDANT RANDRIANJAFY LUC PAUL AMBANJA AMBANJA 1 RANDRIANJAFY Paul Luc Winoc WINOC (Randrianjafy Luc Paul Winoc) GROUPEMENT DE P.P TIM (Tiako I AMBANJA AMBANJA 1 ALY Madagasikara) GROUPEMENT DE P.P IRK (Isika Rehetra AMBANJA AMBANJA 1 SAID HASSAN Ben Said Anoir Said Abdallah Kaominina) INDEPENDANT ABDOUL MAJIDY (Abdoul AMBANJA AMBANJA 1 ABDOUL Majidy Majidy) INDEPENDANT COUNIL DERBOIS (Counil AMBANJA AMBODIMANGA RAMENA 1 COUNIL Derbois Derbois) AMBANJA AMBODIMANGA RAMENA 1 INDEPENDANT REGIS JAORAZA (Regis Jaoraza) REGIS JAORAZA JAORAZA GROUPEMENT DE P.P ANTOKO MAITSO AMBANJA AMBODIMANGA RAMENA 1 FRANCISCO Jaomianko (Antoko Maitso) INDEPENDANT -

Floods in the Northern Part of the Country and Drought in the South Resulted in Nearly 500,000 People in Need of Assistance
ANNUAL REPORT OF THE HUMANITARIAN / RESIDENT COORDINATOR ON THE USE OF CERF GRANTS Country Madagascar Humanitarian / Resident Coordinator Mr. Xavier Leus Reporting Period 1 January 2007- 12 August 2007 I. Executive Summary On the 20 February 2007, the Malagasy Government declared a national state of emergency in Madagascar after a succession of particularly severe storms – including Bondo, Clovis, Favio and Gamede – had battered the island since December. By the end of March, the combined effects of extensive floods in the northern part of the country and drought in the south resulted in nearly 500,000 people in need of assistance. Against this backdrop, a new cyclone, Indlala, struck the north-eastern coast of Madagascar on 15th March, with winds of more than 230 km/h. Even after moving inland, it still registered gusts up to 125 km/h. The storm also continued to unleash torrential rains. Floods washed away villages in the northeast of the country, silted paddy fields and other large agricultural areas, damaged road infrastructure, washed away bridges and made it impossible to reach a number of remote villages where communities remained in dire need of immediate relief aid. These conditions contributed to extensive flooding in heavily populated and cultivated areas throughout the country, including the capital region, the northwest, the northeast, and the southeast. The food security situation deteriorated dramatically, and the risk of maternal and child mortality linked to lack of access to services, and water- and vector-borne diseases, increased. The situation threatened to deteriorate further were timely assistance not provided to address immediate needs and restore agricultural production and livelihoods before the next cyclone season. -

Partie 1 : Materiels Et Methodes
ECOLE SUPERIEURE DES SCIENCES AGRONOMIQUES DEPARTEMENT DES EAUX ET FORETS Mémoire de fin d’études pour l’obtention du Diplôme d’Ingénieur en Sciences Agronomiques et Environnementales au grade de Master en Foresterie et Environnement Parcours : Environnement, Territoire et Développement Promotion « ANDRISA » (2012 – 2017) Les paramètres affectant la demande en Bois Energie : cas des districts d’Ambanja et de Nosy be Présenté par : RABE Eliam Nathanaël Soutenu le 11 décembre 2017 Devant le jury composé de : . Président : Professeur RAMAMONJISOA Bruno Salomon, ESSA-Forêts . Rapporteur : Docteur-HDR RABEMANANJARA Zo Hasina, ESSA-Forêts . Examinateurs : Docteur RAKOTO RATSIMBA Harifidy, ESSA-Forêts Madame RANJEVASOA Mbolatiana, Chef de Service de l’exploitation durable du Bois Energie au Ministère de l’Eau, de l’Energie et des hydrocarbures ECOLE SUPERIEURE DES SCIENCES AGRONOMIQUES DEPARTEMENT DES EAUX ET FORETS Mémoire de fin d’études pour l’obtention du Diplôme d’Ingénieur en Sciences Agronomiques et Environnementales au grade de Master en Foresterie et Environnement Parcours : Environnement, Territoire et Développement Promotion « ANDRISA » (2012 – 2017) Les paramètres affectant la demande en Bois Energie : cas des districts d’Ambanja et de Nosy be Présenté par : RABE Eliam Nathanaël Soutenu le 11 décembre 2017 Devant le jury composé de : . Président : Professeur RAMAMONJISOA Bruno Salomon, ESSA-Forêts . Rapporteur : Docteur-HDR RABEMANANJARA Zo Hasina, ESSA-Forêts . Examinateurs : Docteur RAKOTO RATSIMBA Harifidy, ESSA-Forêts Madame RANJEVASOA Mbolatiana, Chef de Service de l’exploitation durable du Bois Energie au Ministère de l’Eau, de l’Energie et des hydrocarbures Remerciements Au terme de ce mémoire de fin d’études, nous aimerions remercier tout d’abord Dieu sans qui la concrétisation de cette étude n’aurait pu être. -

TONGAZARA Rupaulin ECO M1 10
UNIVERSITÉ DE TOAMASINA FACULTÉ DE DROIT, DES SCIENCES ÉCONOMIQUES ET DE GESTION DÉPARTEMENT D’ÉCONOMIE ************** MÉMOIRE DE MAÎTRISE ÈS SCIENCES ÉCONOMIQUES «ANALYSE DU SYSTÈME ÉDUCATIF ET PERSPECTIVES D’AMÉLIORATION» (Cas de l’enseignement général dans le district d’Ambanja) Présenté et soutenu par : Rupaulin TONGAZARA Promotion : 2007-2008 Sous la Direction de : Monsieur LEMIARY Monsieur Eric RAVANOMANANA Enseignant Chercheur à Ancien Chef CISCO d’Ambanja l’Université de Toamasina Encadreur Professionnel Encadreur Enseignant Date de soutenance : 04 Septembre 2010 1 UNIVERSITÉ DE TOAMASINA FACULTÉ DE DROIT, DES SCIENCES ÉCONOMIQUES ET DE GESTION DÉPARTEMENT D’ÉCONOMIE ************** MÉMOIRE DE MAÎTRISE ÈS SCIENCES ÉCONOMIQUES «ANALYSE DU SYSTÈME ÉDUCATIF ET PERSPECTIVES D’AMÉLIORATION» (Cas de l’enseignement général dans le district d’Ambanja) Présenté et soutenu par : Rupaulin TONGAZARA Promotion : 2007-2008 Sous la Direction de : Monsieur LEMIARY Monsieur Eric RAVANOMANANA Enseignant Chercheur à Ancien Chef CISCO d’Ambanja l’Université de Toamasina Encadreur Professionnel Encadreur Enseignant Date de soutenance 04 Septembre 2010 2 SOMMAIRE REMERCIEMENTS ......................................................................................................... 5 LISTE DES ABREVIATIONS, SIGLES ET ACRONYMES .............................................. 6 GLOSSAIRE .................................................................................................................... 8 INTRODUCTION ............................................................................................................ -

World Bank Document
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: PAD1090 INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT APPRAISAL DOCUMENT FOR A PROPOSED CREDIT IN THE AMOUNT OF SDR 33.8 MILLION (US$50 MILLION EQUIVALENT) Public Disclosure Authorized TO THE REPUBLIC OF MADAGASCAR FOR THE SECOND INTEGRATED GROWTH POLES AND CORRIDOR PROGRAM NOVEMBER 25, 2014 Public Disclosure Authorized Trade and Competitiveness Global Practice AFCS2 – Africa Region Public Disclosure Authorized This document is being made publicly available prior to Board consideration. This does not imply a presumed outcome. This document may be updated following Board consideration and the updated document will be made publicly available in accordance with the Bank’s policy on Access to information. CURRENCY EQUIVALENTS (Exchange Rate Effective September 30, 2014) Currency Unit = SDR SDR0,6745 = US$1 US$1.4826 = SDR 1 MGA2654.98473 = US$1 FISCAL YEAR January 1 – December 31 ABBREVIATIONS AND ACRONYMS ADAPS Association pour le Développement de l’Agriculture et du Paysannat du Sambirano ADEMA Aéroports de Madagascar AFD Agence Française de Développement AfDB African Development Bank AGOA African Growth and Opportunity Act APMF Agence Portuaire Maritime et Fluviale BIANCO Bureau Indépendant Anti-Corruption BOO Build, Own, Operate BoP Bottom of the Pyramid CAMM Chambre d’Arbitrage et de Médiation de Madagascar CAS Country Assistance Strategy CCI Chamber of Commerce and Industry CGA Centre de Gestion Agréé CIRAD Agricultural Research for Development -

World Bank Document
Plan de Passation de marchés I. Généralités 1. L'information sur le projet : Public Disclosure Authorized Pays : Madagascar ; Emprunteur : Non appliqué ; Nom de projet : Citizen Involvement in Municipal Service Improvement (CIMSI) ; Numéro du Projet : P162170 Numéro du Crédit : GPSA Trust Fund Grant No.TF0A4471 ; Agence d’exécution du Projet : ONG SAHA 2. Date d’approbation du Plan de passation de marchés par la Banque : 11 octobre 2017 3. Date de notification de l’Avis Général de Passation de marchés : Non appliquée Public Disclosure Authorized 4. Période couverte par le Plan de Passation de marchés : 18 mois II. Services autres que les services de consultants 1. Seuil de Revue préalable : Les décisions de passation de marchés sujet aux revues préalables de la Banque comme indiqué dans l'Annexe 1 des Directives de passation de marchés : NA 2. Pré-qualification Les soumissionnaires pour ______ seront pré- qualifiés selon les dispositions des paragraphes 2.9 et 2.10 des Directives. NA Public Disclosure Authorized 3. Procédures proposées pour les composantes CDD (selon le paragraphe. 3.17 des Directives : NA [se référer au document approprié d'exécution de projet de CDD approuvé par la Banque] NA 4. Référence (s’il y en a) au Manuel d’exécution du projet / Manuel de Passation de marchés : NA 5. Tout autre arrangement spécial en passation de marchés : [y compris Passation de marchés anticipée et financement rétroactif, si applicable] NA 6. Allotissement de services avec méthodes et calendrier : [Enumérer d’abord les allotissements qui nécessitent la revue préalable de la Banque, ensuite les autres allotissements] Public Disclosure Authorized 1 2 3 4 5 6 7 8 9 Revue de Date Méthode Pré- Préférence la Banque prévue Description Coût Réf. -

Polio Eradication Through Community Approaches
Polio Eradication through Community Approaches November 2018 MCSP’s Role in Eradicating Polio in Madagascar Since mid-2015, MCSP has provided technical assistance for polio campaigns, OBRAs, and routine immunization strengthening with the Ministry of Health, EPI, and partners at the national level and in 12 districts (red dots on map) in the following four regions where USAID provided support via MCSP and the USAID bilateral program, USAID Community Capacity for Health Program (locally known as Mahefa Miaraka): Diana, Sofia, Haute Matsiatra, and Amoron’i Mania (dark blue on the map). Technical assistance focused on the planning, supervision, Introduction independent review, and validation of national polio Between 2014 and 2015, Madagascar had 11 confirmed cases of campaigns, as well as on building vaccine- derived poliovirus (cVDPV),1 signifying challenges with the capacity at the district and health routine immunization system that urgently needed attention. facility levels to conduct acute flaccid paralysis (AFP) and In response to this polio outbreak, the national Expanded Program community based vaccine- on Immunization (EPI) and partners implemented 13 national and preventable disease (VPD) subnational supplemental polio immunization campaigns and surveillance. MCSP also targeted conducted a series of five external outbreak response assessments efforts to improve birth dose and (OBRAs) to identify and help the country address weaknesses in the routine oral polio vaccine (OPV) immunization system. coverage in USG-supported areas by strengthening routine As a result of these efforts and increased community and EPI polio immunization strategies, including the Reaching Every Child (REC) surveillance activities, Madagascar has not had further cVDPV cases approach and identification of and the country achieved Certification of Polio Eradication on target populations and missed June 21, 2018. -
Système Des Nations Unies
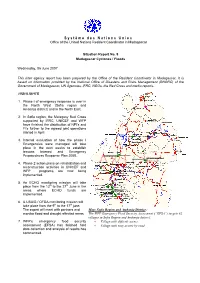
Système des Nations Unies Office of the United Nations Resident Coordinator in Madagascar Situation Report No. 9 Madagascar Cyclones / Floods Wednesday, 06 June 2007 This inter agency report has been prepared by the Office of the Resident Coordinator in Madagascar, It is based on information provided by the National Office of Disasters and Risks Management (BNGRC) of the Government of Madagascar, UN Agencies, IFRC, NGOs, the Red Cross and media reports. HIGHLIGHTS 1. Phase I of emergency response is over in the North West (Sofia region and Ambanja district) and in the North East. 2. In Sofia region, the Malagasy Red Cross supported by IFRC, UNICEF and WFP have finished the distribution of NFI’s and FI's further to the agreed joint operations started in April. 3. Internal evaluation of how the phase I Emergencies were managed will take place in the next weeks to establish lessons learned and Emergency Preparedness Response Plan 2008. 4. Phase 2 action plans on rehabilitation and reconstruction activities in UNICEF and WFP programs are now being implemented. 5. An ECHO monitoring mission will take place from the 13th to the 27th June in the areas where ECHO funds are implemented. 6. A USAID / OFDA monitoring mission will take place from the 9th to the 17th june. The expert will meet with partners and Map: Sofia Region and Ambanja District : monitor flood and drought affected areas. The WFP Emergency Food Security Assessment (“EFSA”) targets 82 villages in Sofia Region and Ambanja district: 7. WFP's emergency food security • Village with difficult access. assessment (EFSA) has finished field • Village with easy access by road data collection and analysis of results has commenced. -

Madagascar) - Région Picardie (France)
Centre International de Développement et de Recherche Coopération décentralisée Région Diana (Madagascar) - Région Picardie (France) Programmes de développement des pôles urbains de la Diana (PDPU -Diana) Tousdroits de reproduction réservés – AIDR © – 1128 Gaston Mananjara (T&D) Mickaël Niess (CIDR) Mars 2008 Publication UNGANA COOPERATION DECENTRALISEE REGION DIANA (MADAGASCAR) – REGION PICARDIE (FRANCE) PROGRAMME DE DEVELOPPEMENT DES POLES URBAINS DE LA DIANA (PDPU-DIANA) CIDR/Madagascar/PDPU-Diana/GM/MN/n° 2 Mars 2008 2 SOMMAIRE Partie I - Analyse du contexte et des enjeux du Programme ......... 7 1. Au niveau national ..................................................................... 8 1.1. Analyse des politiques nationales et de leur cohérence 8 1.1.1. Les différentes politiques nationales 8 1.1.2. Analyse de la cohérence des politiques et stratégies nationales 9 1.2. Analyse des évolutions institutionnelles 11 1.2.1. Les changements au niveau de l’organisation, du fonctionnement et des attributions du fokontany. 11 1.2.2. Les réformes en cours sur la fiscalité locale 13 1.2.3. La réforme en cours sur l’intercommunalité 15 1.2.4. La montée en puissance des transferts financiers de l’Etat au profit des collectivités locales, notamment des Régions 16 1.3. Analyse des dispositifs techniques et financiers d’accompagnement 16 1.3.1. Le dispositif technique : les Centres d’Appui aux Communes (CAC) 17 1.3.2. L’outil financier : le Fonds de Développement Local (FDL) 20 2. Au niveau régional et local ...................................................... 21 2.1. Région et décentralisation 21 2.1.1. Planification et aménagement du territoire 21 2.1.2. Maîtrise d’ouvrage régionale et prise en compte des programmes sectoriels et du PN2D 22 2.1.3.