(COVID- 19) in Iran
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
IRN Population Movement Snapshot June 2021
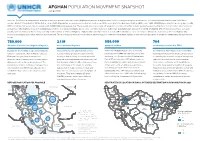
AFGHAN POPULATION MOVEMENT SNAPSHOT June 2021 Since the 1979 Soviet invasion and the subsequent waves of violence that have rocked Afghanistan, millions of Afghans have fled the country, seeking safety elsewhere. The Islamic Republic of Iran boasts 5,894 km of borders. Most of it, including the 921 km that are shared with Afghanistan, are porous and located in remote areas. While according to the Government of Iran (GIRI), some 1,400-2,500 Afghans arrive in Iran every day, recently GIRI has indicated increased daily movements with 4,000-5,000 arriving every day. These people aren’t necesserily all refugees, it is a mixed flow that includes people being pushed by the lack of economic opportunities as well as those who might be in need of international protection. The number fluctuates due to socio-economic challenges both in Iran and Afghanistan and also the COVID-19 situation. UNHCR Iran does not have access to border points and thus is unable to independently monitor arrivals or returns of Afghans. Afghans who currently reside in Iran have dierent statuses: some are refugees (Amayesh card holders), other are Afghans who posses a national passport, while other are undocumented. These populations move across borders in various ways. it is understood that many Afghans in Iran who have passports or are undocumented may have protection needs. 780,000 2.1 M 586,000 704 Amayesh Card Holders (Afghan refugees1) undocumented Afghans passport holders voluntarily repatriated in 2021 In 2001, the Government of Iran issues Amayesh Undocumented is an umbrella term used to There are 275,000 Afghans who hold family Covid-19 had a clear impact on the low VolRep cards to regularize the stay of Afghan refugees. -

Working Group on Dry Ports Dry Ports in Iran
Ministry of Roads Working Group on Dry Ports & Urban Development First Meeting Bangkok, 25 – 26 November 2015 Dry Ports in Iran: an essential need to facilitate regional transit and trade among Land locked countries Teymour Bashirgonbadi Deputy Director General, Intl. Office Ministry of Roads and Urban Development I. R. Iran: signatory (7 November 2013) Situation of Ratification: Under the procedure and progress of ratification. Hopefully in 2016 become a party to the agreement. Participant Signature Approval(AA), Acceptance(A), Accession(a), Ratification Armenia 7 Nov 2013 Bangladesh 25 Sep 2014 Cambodia 7 Nov 2013 China 7 Nov 2013 Indonesia 7 Nov 2013 Iran (Islamic Republic of) 7 Nov 2013 under process and procedures of adoption in Parliament Lao People's Democratic Republic 7 Nov 2013 Mongolia 7 Nov 2013 Myanmar 7 Nov 2013 Nepal 7 Nov 2013 Republic of Korea 7 Nov 2013 22 Apr 2014 Russian Federation 7 Nov 2013 Sri Lanka 16 May 2014 Tajikistan 7 Nov 2013 20 Nov 2015 AA Thailand 7 Nov 2013 7 Nov 2013 Turkey 15 Dec 2014 Viet Nam 7 Nov 2013 29 Oct 2014 AA Imam Khomeini International Airport, Tehran Province Motahari Rail Station, Mashhad, Khorasan Razavi Province Salafchegan Special Economic Zone, Qom Province Sirjan Special Economic Zone, Kerman Province [Arvand Free Industrial Zone, Khozestan Province] [Sahlan Special Economic Zone, Tabriz, East Azerbaijan Province ] [Sarakhs Special Economic Zone, Khorasan Razavi Province ] [Shahid Dastgheyb International Airport, Shiraz, Fars Province] [Zahedan Logistics Centre, Sistan and Bakluchestan Province ] Iran’s dry ports location in map Caspian Sea 6 7 1 2 3 4 5 8 9 1. -

Iran Stands up Against Transatlantic Bullying the Tabriz Based Club’S Officials Parted Company with the 49-Year-Old Coach on Tuesday
WWW.TEHRANTIMES.COM I N T E R N A T I O N A L D A I L Y 8 Pages Price 50,000 Rials 1.00 EURO 4.00 AED 42nd year No.13829 Wednesday DECEMBER 9, 2020 Azar 19, 1399 Rabi’ Al thani 23, 1442 Zarif advises regional Jordan Burroughs Iranian university Architect Amirali states to exclude West misses competing students runner-up Sardar-Afkhami in regional talks Page 2 in Iran Page 3 at IMC 2020 Page 7 dies at 91 Page 8 Iran completely self-sufficient in building freight wagons Iran stands up against TEHRAN – Iranian railway industry has systems for freight wagons. become completely self-reliant in man- “For the first time this year, national ufacturing freight wagons, Head of the (domestically-made) wheels will move on Islamic Republic of Iran Railways (known the national rail,” the official said. as RAI) Saeed Rasouli said. Mentioning the launch of a system for Speaking in an unveiling ceremony for introducing the needs of the country’s railway transatlantic bullying domestically-made wagon brake system industry to domestic manufacturers and and wheels on Tuesday, Rasouli announced companies producing parts for the railway that RAI is going to sign a contract with transportation industry, the official noted domestic manufacturers for the purchase that so far 4,600 parts have been requested See page 3 of 500 monoblock wheels and 500 brake on this website. Continued on page 4 Rouhani: Astana peace talks can protect Syrian territorial integrity TEHRAN — President Hassan Rouhani Rouhani said during a meeting with visiting on Tuesday hailed the Astana peace talks, Syrian Foreign Minister Faisal al-Mekdad. -

Elbrus 5642M (South) - Russia
Elbrus 5642m (South) - Russia & Damavand 5671m - Iran EXPEDITION OVERVIEW Mount Elbrus and Mount Damavand Combo In just two weeks this combo expedition takes you to the volcanoes of Damavand in Iran, which is Asia’s highest, and Elbrus in Russia, which is Europe’s highest. On Elbrus we gradually gain height and increase our chance of success by taking time to acclimatise in the Syltran-Su valley on Mount Mukal, which offers views across the beautiful valleys to Elbrus. Once acclimatised, we climb these sweeping snow slopes to the col between Elbrus’ twin summits before continuing easily to the true summit of Europe’s highest mountain in an ascent of about 1000m. A brief celebration and then we fly direct to Tehran where Mount Damavand may be little known outside its home nation of Iran but it is Asia’s highest volcano and provides a delightful challenge for mountaineers. It is located northeast of Tehran, close to the Caspian Sea and dominates the Alborz mountain range. Damavand is, with its near-symmetrical lines, a beautiful and graceful peak that has lain dormant for 10,000 years. On reaching the crater rim you walk around it to the true summit and it is possible to walk into the crater. It is technically easy but demands a good level of fitness. PLEASE NOTE – YOU WILL NEED TO BOOK THIS TRIP AT LEAST 3 MONTHS BEFORE THE DEPARTURE DATE, TO ALLOW TIME TO GET YOUR AUTHORISATION CODE AND VISA FOR IRAN. The Volcanic Seven Summits Challenge – your dream met, a worldwide journey to the seven continents with a unique challenge that has only been completed by a handful of people. -

Religious Tourism Development Strategies in Qom Province: Using and Comparing QSPM and Best Worst Methods
International Journal of Religious Tourism and Pilgrimage Volume 8 Issue 8 Article 4 2020 Religious Tourism Development Strategies in Qom Province: Using and Comparing QSPM and Best Worst Methods Hooshang Asheghi-Oskooee University of Qom, [email protected] Marzieh Ramezanzadeh University of Qom, [email protected] Mohammad Hasan Maleki University of Qom, Iran, [email protected] Follow this and additional works at: https://arrow.tudublin.ie/ijrtp Part of the Strategic Management Policy Commons, and the Tourism and Travel Commons Recommended Citation Asheghi-Oskooee, Hooshang; Ramezanzadeh, Marzieh; and Maleki, Mohammad Hasan (2020) "Religious Tourism Development Strategies in Qom Province: Using and Comparing QSPM and Best Worst Methods," International Journal of Religious Tourism and Pilgrimage: Vol. 8: Iss. 8, Article 4. doi:https://doi.org/10.21427/1k11-m644 Available at: https://arrow.tudublin.ie/ijrtp/vol8/iss8/4 Creative Commons License This work is licensed under a Creative Commons Attribution-Noncommercial-Share Alike 4.0 License. © International Journal of Religious Tourism and Pilgrimage ISSN : 2009-7379 Available at: http://arrow.tudublin.ie/ijrtp/ Volume 8(viii) 2020 Religious Tourism Development Strategies in Qom Province: Using and Comparing QSPM and Best Worst Methods Hooshang Asheghi-Oskooee University of Qom, Iran [email protected] Marzieh Ramezanzadeh University of Qom, Iran [email protected] Mohammad Hasan Maleki University of Qom, Iran [email protected] After Mashhad county, Qom province has the most valuable religious, cultural, historical and natural potential as the second Iranian pilgrimage centre. This study was conducted to formulate strategies for the development of religious tourism in Qom province using the most influential view of the strategy-formation process named design school. -

Fluoride Concentration of Drinking-Water of Qom, Iran
Iranian Journal of Health Sciences 2016; 4(1): 37-44 http://jhs.mazums.ac.ir Original Article Fluoride Concentration of Drinking-Water of Qom, Iran Ahmad Reza Yari 1 *Shahram Nazari 1 Amir Hossein Mahvi 2 Gharib Majidi 1, Soudabeh Alizadeh Matboo 3 Mehdi Fazlzadeh 3 1- Department of Environmental Health Engineering, School of Public Health, Qom University of Medical Sciences, Qom, Iran 2- Department of Environmental Health Engineering, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran 3- Department of Environmental Health Engineering, School of Public Health, Ardabil University of Medical Sciences, Ardabil, Iran *[email protected] (Received: 4 Jul 2015; Revised: 22 Oct 2015; Accepted: 27 Dec 2015) Abstract Background and Purpose: Fluoride is a natural element essential for human nutrition due to its benefits for dental enamel. It is well-documented that standard amounts of fluoride in drinking- water can decrease the rate of dental caries. This study was conducted with the aim of measuring fluoride concentration of drinking-water supplies and urban distribution system in Qom, Iran. Materials and Methods: Results were subsequently compared against national and international standards. All sources of drinking-water of rural and urban areas were examined. To measure fluoride, the standard SPADNS method and a DR/4000s spectrophotometer were used . Results: Results showed that the mean of fluoride concentration in rural areas, mainly supplied with groundwater sources, was 0.41 mg/L, that of the urban distribution system 0.82 mg/L, that of Ali-Abad station 0.11 mg/L, and that of the private water desalination system 0.24 mg/L. -

Investigation of Qom Rural Area Water Network Accident in 2010 and Minimization Approaches of Accident Frequencies
•Arch Hyg Sci 2016;5(1): 33-38. RESEARCH ARTICLE •Journal Homepage: http://jhygiene.muq.ac.ir Investigation of Qom Rural Area Water Network Accident in 2010 and Minimization Approaches of Accident Frequencies Hossein Jafari Mansooriana,b, Ahmad Reza Yaric, Mohsen Ansarid, Shahram Nazarie, Mohamad Saberi Bidgolid, Gharib Majidid* aEnvironmental Health Engineering Research Center, Department of Environmental Health, Kerman University of Medical Sciences, Kerman, Iran. bYoung Researchers and Elite Club, Hamedan Branch, Islamic Azad University, Hamedan, Iran. cResearch Center for Environmental Pollutants, Qom University of Medical Sciences, Qom, Iran. dDepartment of Environmental Health Engineering, School of Public Health, Qom University of Medical Sciences, Qom, Iran. eSchool of Khalkhal Medical, Ardabil University of Medical Sciences, Ardabil, Iran. *Correspondence should be addressed to Mr. Gharib Majidi, Email: [email protected] A-R-T-I-C-L-EI-N-F-O A-B-S-T-R-A-C-T Article Notes: Background & Aims of the Study: Accidents in water networks can lead to increase the Received: Oct 25, 2015 uncounted water, costs of repair, maintenance, restoration and enter water contaminants to water network. The aim of this study is to survey the accidents of Qom rural water network Received in revised form: and choose the right approaches to reduce the number of accidents. Dec 2, 2015 Materials & Methods: In this cross-sectional study, four sector of Qom province Accepted: Dec 23, 2015 (Markazi, Dastjerd, Kahak and Qahan), were assessed over a period of 8 months (July – Available Online: Jun 1, January 2010). This study was conducted through questionnaire of Ministry of Energy. 2016 Results: The total number of accidents was 763. -

UNIVERSITY of KWAZULU-NATAL the Provision of Efficient Transport
UNIVERSITY OF KWAZULU-NATAL The Provision of Efficient Transport Services in the Iranian Maritime and Land Transport Interface By Farhad Razkhaneh 206525761 A dissertation submitted in fulfillment of the requirements for the degree of Doctor of Philosophy in Economics School of Accounting, Economics and Finance College of Law & Management Studies Supervisor: Professor Trevor Jones 2014 ii Acknowledgements I extend my sincere gratitude to all those who helped me through the process and preparation of this Doctoral Thesis. My sincere gratitude goes to my supervisor, Professor Trevor Jones, who meticulously read through the drafts and provided me with valuable editorial suggestions and guided me with technical comments, criticisms, guidance and support through the various stages of the writing and completion of this thesis. His efforts, knowledge and experience in international trade and transportation, ports and maritime, and merchant shipping transport related issues, have contributed towards the success of this thesis. The research and writing of this thesis, whilst at times difficult and challenging, has contributed towards my academic knowledge development, with which I hope to humbly contribute, through further writing, teaching and research, back to society. Special thanks to Professor Geoff Harris for reading earlier chapters of this thesis and providing the valuable suggestions and guidance to me. I extend my thanks to friends in the School of Accounting, Economics and Finance at the University of KwaZulu-Natal, Professor Dev Tewari and Post Doc Mr. O.B. Saiedo for their help. In addition, I am grateful for support and interest shown by colleagues in the Islamic Republic of Iran Shipping lines and individuals in the freight industry, in particular Mr. -

Geopolitics of the Iranian Nuclear Energy Program
Geopolitics of the Iranian Nuclear Energy Program But Oil and Gas Still Matter CENTER FOR STRATEGIC & CSIS INTERNATIONAL STUDIES A Report of the CSIS Energy and National Security Program 1800 K Street, NW | Washington, DC 20006 author Tel: (202) 887-0200 | Fax: (202) 775-3199 Robert E. Ebel E-mail: [email protected] | Web: www.csis.org March 2010 ISBN 978-0-89206-600-1 CENTER FOR STRATEGIC & Ë|xHSKITCy066001zv*:+:!:+:! CSIS INTERNATIONAL STUDIES Geopolitics of the Iranian Nuclear Energy Program But Oil and Gas Still Matter A Report of the CSIS Energy and National Security Program author Robert E. Ebel March 2010 About CSIS In an era of ever-changing global opportunities and challenges, the Center for Strategic and International Studies (CSIS) provides strategic insights and practical policy solutions to decision- makers. CSIS conducts research and analysis and develops policy initiatives that look into the future and anticipate change. Founded by David M. Abshire and Admiral Arleigh Burke at the height of the Cold War, CSIS was dedicated to the simple but urgent goal of finding ways for America to survive as a nation and prosper as a people. Since 1962, CSIS has grown to become one of the world’s preeminent public policy institutions. Today, CSIS is a bipartisan, nonprofit organization headquartered in Washington, D.C. More than 220 full-time staff and a large network of affiliated scholars focus their expertise on defense and security; on the world’s regions and the unique challenges inherent to them; and on the issues that know no boundary in an increasingly connected world. -

See the Document
IN THE NAME OF GOD IRAN NAMA RAILWAY TOURISM GUIDE OF IRAN List of Content Preamble ....................................................................... 6 History ............................................................................. 7 Tehran Station ................................................................ 8 Tehran - Mashhad Route .............................................. 12 IRAN NRAILWAYAMA TOURISM GUIDE OF IRAN Tehran - Jolfa Route ..................................................... 32 Collection and Edition: Public Relations (RAI) Tourism Content Collection: Abdollah Abbaszadeh Design and Graphics: Reza Hozzar Moghaddam Photos: Siamak Iman Pour, Benyamin Tehran - Bandarabbas Route 48 Khodadadi, Hatef Homaei, Saeed Mahmoodi Aznaveh, javad Najaf ...................................... Alizadeh, Caspian Makak, Ocean Zakarian, Davood Vakilzadeh, Arash Simaei, Abbas Jafari, Mohammadreza Baharnaz, Homayoun Amir yeganeh, Kianush Jafari Producer: Public Relations (RAI) Tehran - Goragn Route 64 Translation: Seyed Ebrahim Fazli Zenooz - ................................................ International Affairs Bureau (RAI) Address: Public Relations, Central Building of Railways, Africa Blvd., Argentina Sq., Tehran- Iran. www.rai.ir Tehran - Shiraz Route................................................... 80 First Edition January 2016 All rights reserved. Tehran - Khorramshahr Route .................................... 96 Tehran - Kerman Route .............................................114 Islamic Republic of Iran The Railways -

English/Persian
0156900008 Le i 27 N- L~ ^^^ Islamic Republic of Iran Emblem Thé Présidents Office Thelranian Cultural Héritage, Handicrafts and Tourism Organhation In thé Name of God In Compliance with Article 12 to thé International Convention on thé Safeguarding of thé Intangible Cultural Héritage, and referring to thé Rule of thé Islamic Republic of Iran's Joining thé mentioned Convention approved in 2005, at thé Iranian Islamic Consultative Assembly, as well as thé Rules of Procédures thereof, and Article 3 of thé Articles of Association of thé Iranian Cultural Héritage, Handicrafts and Tourism Organizatîon approved in 1988, at thé Iranian Islamic Consultative Assembly, intangible Cultural Héritage Elément titled UThe Art ofCrafting and Playing Oud" in Iran with thé following particulars: Domain of thé Intangible Cultural Héritage Elément: National Wide Is, hereby, inscribed on this date of 20 Feb. 2019 as No. 1763, on thé Iranian National List ofthé Intangible Cultural Héritage. Mohammad Hassan Talebian AU Asghar Mounesan Vice Président & Cultural Héritage Deputy Head of Thé Iranian Cultural Héritage, (Signed) Handicrafts and Tourism Organization (Signed) (CÎJ) ^fw^t^ ^/fe^'^pgîî-^9"r\ï1^ (J^^ ^V.^iJ^^!j^^iu'^^^Ar'^i/}if^^^^^^ « »a* t»- - -. '. '^ . ~ »! N w * ^f^^^U^v^i(^^^C^'Tfi(/^^^^^fJi * v ^ ^ »1« ^^^^. t^^^^^^^^^ip^ *1 *. * »* * » ^^^^<» â^^^^ ^J^(j'/C(/^^j^{J'^^^ nv/ff/^ ^ùw^f ^f, c/^7^ .0^^^ ^U/(^u>4f<^r'>$^^ ,/^^^^ . H/ 7^. ...... çy^S...... -^ -< J Extract ICH National Inventory of thé IR of Iran Title: Crafting and Playing thé Oud Thé Iranian Cultural Héritage, Handicrafts and Tourism Organization (ICHHTO) had this élément inscribed on thé National ICH Inventory of thé Islamic Republic ofIran on 20 Feb. -

MIDDLE EAST, NORTH AFRICA India Evacuates Its Citizens from Iran OE Watch Commentary: When COVID-19 Hit Iran, Qom Quickly Became Its Initial Epicenter
MIDDLE EAST, NORTH AFRICA India Evacuates its Citizens from Iran OE Watch Commentary: When COVID-19 hit Iran, Qom quickly became its initial epicenter. Close to Tehran, Qom is the site of pilgrimage to the Shrine of Fatima Masumeh, the second most sacred site inside Iran for Shi’ite Muslims after the tomb of Imam Reza in Mashhad. Beyond pilgrimage, however, Qom is a center for study, second only to Najaf in Iraq. Thousands of foreigners study in its religious seminaries. The excerpted article from the Mehr News Agency, an outlet owned by the Islamic Ideology Dissemination Organization, details a meeting between India’s ambassador to Iran and the governor of Qom as the two governments sought to evacuate the 1,200 Indian pilgrims and students stranded in Qom during Nowruz and after the coronavirus lockdown. In early March, Indian Foreign Minister Subrahmanyam Jaishankar Indian pilgrims in Tehran demand evacuation against the backdrop of the Coronavirus pandemic. reported 6,000 Indian nationals were in Iran, including 1,100 Source: Idat.ir, https://idat.ir/upload/attach/573/20200312-1840070.jpeg from Ladakh, Jammu and Kashmir, and Maharshtra, 300 students from Jammu and Kashmir, and 1,000 fishermen from Kerala, Tamil Nadu, and Gujarat. The article highlights the many special measures that authorities in Qom took for the safety of Indian citizens and notes that the Indian Ambassador “praised the management of the province in hosting and treating Indian citizens...” India and Iran have always maintained close cultural links. Persian is an Indo-European language and was for centuries the lingua franca across the Indian subcontinent; it was the official language of the Mughal Empire until 1835, when the British Empire imposed English in its stead.