Georgia Health Cluster
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

World Bank Document
b Public Disclosure Authorized Roads Department of the Ministry of Regional Development and Infrastructure of Georgia Environmental and Social Impact Assessment of Construction Works for the Bakurtsikhe-Tsnori (16km) Public Disclosure Authorized Road Section Public Disclosure Authorized Public Disclosure Authorized Draft report October 2018 LIST OF ACRONIMS EIA - Environmental Impact Assessment EMP - Environmental Management Plan ESIA - Environmental and Social Impact Assessment ESMP - Environmental and Social Management Plan HSE - Health, Safety, Environment HS - Health and Safety GIS - Geographic Information System GoG - Government of Georgia IPPC - Integrated Pollution Prevention and Control KP - Kilometer Post MESD - Ministry of Economy and Sustainable Development of Georgia MEPA - Ministry of Environment Protection and Agriculture of Georgia MLHSA - Ministry of Labor, Health and Social Affairs of Georgia NGO - Non-Governmental Organization RD - Roads Department of the Ministry of Regional Development and Infrastructure of Georgia MRDI - Ministry of Regional Development and Infrastructure of Georgia ToR - Terms of Reference WB - The World Bank Table of Contents 2.1 Environmental Policies and Laws of Georgia ....................................................................................... 2 2.2 Laws and Regulations Related to Social Aspects and Land Ownership .............................................. 5 2.3 Labor Legislation ................................................................................................................................... -

USAID Zrda to Launch Small Grants Program in the Akhmeta Municipality
FOR IMMEDIATE RELEASE February 5, 2018 For additional information: Keti Rekhviashvili, Communications Manager Phone: 032 222 74 95 Email: [email protected] USAID Zrda to Launch Small Grants Program in the Akhmeta Municipality Akhmeta, Kakheti region - On February 5, 2018, USAID/Georgia Economic Growth Office Director Veronica Lee joined Akhmeta Municipality Head Ioseb Karumashvili, to meet with local communities and launch a Small Grants Program, initiated by USAID’s Zrda Activity. The Small Grants program is designed for nine target communities of the Akhmeta municipality (city Akhmeta, Kvemo Alvani, Zemo Alvani, Matani, Sakobiano, Duisi, Jokolo, Khalatsani and Omalo) to support business development through small grants assistance to micro and small enterprises. Within the Program, Zrda plans to award up to 60 grants for agriculture and tourism development activities in target communities. At least 35% of total project value is requested as a leverage from an entrepreneur. The Small Grants Program will build upon and diversify Zrda’s ongoing activities in the communities of the Akhmeta municipality. Through its agriculture interventions, Zrda established five 100-sq. m. greenhouse demonstration plots for seedling- and vegetable production, and today local farmers have an access to agriculture development programs offered by the government and international organizations. In tourism sector, Zrda supported guesthouse owners to boost their incomes through improving their marketing skills and helping them join well-known, international -

Economic Prosperity Initiative
USAID/GEORGIA DO2: Inclusive and Sustainable Economic Growth October 1, 2011 – September 31, 2012 Gagra Municipal (regional) Infrastructure Development (MID) ABKHAZIA # Municipality Region Project Title Gudauta Rehabilitation of Roads 1 Mtskheta 3.852 km; 11 streets : Mtskheta- : Mtanee Rehabilitation of Roads SOKHUMI : : 1$Mestia : 2 Dushet 2.240 km; 7 streets :: : ::: Rehabilitation of Pushkin Gulripshi : 3 Gori street 0.92 km : Chazhashi B l a c k S e a :%, Rehabilitaion of Gorijvari : 4 Gori Shida Kartli road 1.45 km : Lentekhi Rehabilitation of Nationwide Projects: Ochamchire SAMEGRELO- 5 Kareli Sagholasheni-Dvani 12 km : Highway - DCA Basisbank ZEMO SVANETI RACHA-LECHKHUMI rehabilitaiosn Roads in Oni Etseri - DCA Bank Republic Lia*#*# 6 Oni 2.452 km, 5 streets *#Sachino : KVEMO SVANETI Stepantsminda - DCA Alliance Group 1$ Gali *#Mukhuri Tsageri Shatili %, Racha- *#1$ Tsalenjikha Abari Rehabilitation of Headwork Khvanchkara #0#0 Lechkhumi - DCA Crystal Obuji*#*# *#Khabume # 7 Oni of Drinking Water on Oni for Nakipu 0 Likheti 3 400 individuals - Black Sea Regional Transmission ZUGDIDI1$ *# Chkhorotsku1$*# ]^!( Oni Planning Project (Phase 2) Chitatskaro 1$!( Letsurtsume Bareuli #0 - Georgia Education Management Project (EMP) Akhalkhibula AMBROLAURI %,Tsaishi ]^!( *#Lesichine Martvili - Georgia Primary Education Project (G-Pried) MTSKHETA- Khamiskuri%, Kheta Shua*#Zana 1$ - GNEWRC Partnership Program %, Khorshi Perevi SOUTH MTIANETI Khobi *# *#Eki Khoni Tskaltubo Khresili Tkibuli#0 #0 - HICD Plus #0 ]^1$ OSSETIA 1$ 1$!( Menji *#Dzveli -
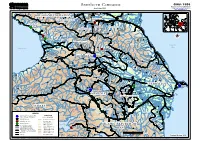
Southern Caucasus Geographic Information and Mapping Unit As of June 2003 Population and Geographic Data Section Email : [email protected]
GIMU / PGDS Southern Caucasus Geographic Information and Mapping Unit As of June 2003 Population and Geographic Data Section Email : [email protected] Znamenskoye)) )) Naurskaya Aki-Yurt ))) Nadterechnaya Dokshukino Malgobek Babayurt RUSSIANRUSSIAN FEDERATIONFEDERATION Chervlennaya ))Nalchik INGUSHETIAINGUSHETIAINGUSHETIA Gudermes KABARDINO-BALKARIAKABARDINO-BALKARIA Sleptsovskaya Grozny Khazavyurt )) Argun )) )) NazranNazran )) ))) NazranNazran )) Kizilyurt Ardon Achkhay-Martan ABKHAZIAABKHAZIA Urus-Martan Shali Alagir )) VladikavkazVladikavkaz CHECHNYACHECHNYA VladikavkazVladikavkaz CHECHNYACHECHNYA SOUTHERNCAUCASUS_A3LC.WOR SukhumiSukhumi )) SukhumiSukhumi )) )) NORTHNORTH OSSETIAOSSETIA )))Vedeno Kaspiysk Nizhniy Unal )) Buynaksk )) Itum-Kali)) Botlikh Shatili)) GaliGali Izberbash !!! ZugdidiZugdidi ZugdidiZugdidi Sergokala SOUTHSOUTH OSSETIAOSSETIA Levashi Tskhinvali Caspian Dagestanskiye Ogni Kareli Sea Black Sea )) Derbent Lanchkhuti )) AkhmetaAkhmeta Khashuri Gori AkhmetaAkhmeta Kvareli Telavi Lagodekhi Gurdzhaani TBILISITBILISI Belakan GEORGIAGEORGIA Kasumkent Batumi)) ADJARIAADJARIA Akhaltsikhe Tsnori Zaqatala Khudat Tsalka Tetri-Tskaro Rustavi Khryuk Khachmas Bolnisi Marneuli Tsiteli-Tskaro Akhalkalaki QAKH Kusary Hopa Shulaveri Kuba Dmanisi Bagdanovka Sheki Divichi Pazar Artvin Alaverdi Akstafa Cayeli Ardahan Oghus Siazan Rize Tauz Mingechaur Lake Tumanyan Gabala Idzhevan Dallyar Dzheir Lagich Kirovakan Shamkhor Gyumri Mingechaur Ismailly Dilizhan Dilmamedli Agdash Geokchay Artik Shamakha Nasosnyy Kars Goranboy Yevlakh Kedabek -
Daily Report for 21 August 2008
Emergency Operation in Georgia Daily Report for 21 August 2008 Displacements caused by recent conflict over South Ossetia Displacement within Georgia excl. South Ossetia 98,600 Displacement within South Ossetia 30,000 Sub Total Georgia 128,600 Displacement to Russian Federation 30,000 Displacements Total 158,600 In addition, Georgia has a caseload of 220,000 IDPs from previous crises. Western Georgian distribution in full swing In Western and Central Georgia, UNHCR estimates that there are between 20 000 and 25 000 persons in need of assistance. The first shipment of aid arrived on August 19 by plane to Batumi airport and after a swift transport to the warehouses, the distribution is already well on its way. Today the UNHCR team distributed non-food items for some 500 IDPs in the city of Senaki. These IDPs have been in the region already since 1992 – 1993 and are now facing a new catastrophe as their centres have been damaged by the bombings. The UNHCR team assessing the damages concluded that immediate reparations are needed to provide proper shelter before winter. At the same time, a coordination meeting was held in the city of Kutaisi which will serve as a distribution hub for the region. The meeting, assisted by the local authorities, IDP representatives and UNHCR, assessed the needs in the area and the distribution started immediately reaching close to the western border of South Ossetia, as close as the villages of Sachkhre and Chiatura. Furthermore, the urgently needed hygiene kits are being distributed by ICRC and NRC, upon request from UNHCR. -

World Bank Document
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: 66462-GE PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT IN THE AMOUNT OF SDR 25.8 MILLION Public Disclosure Authorized (US$40.00 MILLION EQUIVALENT) AND A PROPOSED LOAN IN THE AMOUNT OF US$30 MILLION TO GEORGIA Public Disclosure Authorized FOR THE SECOND SECONDARY AND LOCAL ROADS PROJECT (SLRP-II) FEBRUARY 21, 2012 Sustainable Development Department South Caucasus Country Unit Europe and Central Asia Region Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective January 1, 2012) Currency Unit = Georgian Lari (GEL) GEL 1.66 = US$ 1.00 US$1.551 = SDR 1.00 FISCAL YEAR January 1 – December 31 ABBREVIATIONS AND ACRONYMS AADT Average Annual Daily Traffic MCC Millennium Challenge Corporation ADB Asian Development Bank MENR Ministry of Environment and Natural Resources CPS Country Partnership Strategy MESD Ministry of Economy and Sustainable Development EA Environmental Assessment MRDI Ministry of Regional Development and Infrastructure EIB European Investment Bank NBG National Bank of Georgia EIRR Economic Internal Rate of Return NCB National Competitive Bidding EMP Environmental Management Plan NPV Net Present Value ESMF Environmental and Social Management Framework ORAF Operational Risk Assessment Framework FA Financing Agreement PAD -

Urban Development in Georgia
Key facts and figures relating to housing and urban development in Georgia Nino Gventsadze Head of spatial planning department Ministry of regional development and infrastructure of Georgia Housing in Georgia Current conditions Housing in Georgia is characterized with long and deep systematic crisis which are caused by the following reasons: non- existent policy, non-sufficient legislative base and non-adequate institutional set-up. Georgian government still doesn’t have a well-defined, clear policy in the field of Housing, also not a single office directly governs and works on Housing issues neither on legislation or enforcement level. Estimated future plan in Housing • To define short, medium and long term priorities Short term priority – should focus on how to fix homelessness, clearly define the terminology, exact identification of beneficiary groups and setting criteria for people who will receive the support, launching an institution, drafting legislation etc. Medium and long term - should focus on large number of people who will be able to afford the Housing (affordable Housing), provide an adequate Housing, improve policy making in regard of construction and urban development, solving demographic issues in the country etc. Improvements In 2018, Government of Georgia has taken a duty in implementing a “Housing policy documentation and strategic plan”, for that reason in 2019, April a special committee was established who will define a strategic plan. So far consultations are taking place. It is planned to make an amendments in legislation (In Georgian legislation there is the only law, which is dedicated to housing and needs a great deal of revise and improvement) The Ministry of Internally Displaced Persons from the Occupied Territories and Refugees of Georgia has realized several projects: • Ministry purchased 300 accommodations from the Chinese company “Hualing” • Throughout the country, ministry purchased several accommodations from developers, reconstructed, built new constructions etc. -
Scaling-Up Multi-Hazard Early Warning System and the Use of Climate Information in Georgia
Annex VI (b) – Environmental and Social Assessment Report Green Climate Fund Funding Proposal I Scaling-up Multi-Hazard Early Warning System and the Use of Climate Information in Georgia Environmental and Social Assessment Report FP-UNDP-5846-Annex-VIb-ENG 1 Annex VI (b) – Environmental and Social Assessment Report Green Climate Fund Funding Proposal I CONTENTS Contents ................................................................................................................................................. 2 Executive Summary ............................................................................................................................... 8 1 Introduction ................................................................................................................................ 10 1.1 Background ................................................................................................................................. 10 1.2 Description of the Project ............................................................................................................ 10 1.2.1 Summary of Activities .......................................................................................................... 11 1.3 Project Alternatives ..................................................................................................................... 27 1.3.1 Do Nothing Alternative ........................................................................................................ 27 1.3.2 Alternative Locations .......................................................................................................... -

Review of Fisheries and Aquaculture Development Potentials in Georgia
FAO Fisheries and Aquaculture Circular No. 1055/1 REU/C1055/1(En) ISSN 2070-6065 REVIEW OF FISHERIES AND AQUACULTURE DEVELOPMENT POTENTIALS IN GEORGIA Copies of FAO publications can be requested from: Sales and Marketing Group Office of Knowledge Exchange, Research and Extension Food and Agriculture Organization of the United Nations E-mail: [email protected] Fax: +39 06 57053360 Web site: www.fao.org/icatalog/inter-e.htm FAO Fisheries and Aquaculture Circular No. 1055/1 REU/C1055/1 (En) REVIEW OF FISHERIES AND AQUACULTURE DEVELOPMENT POTENTIALS IN GEORGIA by Marina Khavtasi † Senior Specialist Department of Integrated Environmental Management and Biodiversity Ministry of the Environment Protection and Natural Resources Tbilisi, Georgia Marina Makarova Head of Division Water Resources Protection Ministry of the Environment Protection and Natural Resources Tbilisi, Georgia Irina Lomashvili Senior Specialist Department of Integrated Environmental Management and Biodiversity Ministry of the Environment Protection and Natural Resources Tbilisi, Georgia Archil Phartsvania National Consultant Thomas Moth-Poulsen Fishery Officer FAO Regional Office for Europe and Central Asia Budapest, Hungary András Woynarovich FAO Consultant FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS Rome, 2010 The designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations (FAO) concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or products of manufacturers, whether or not these have been patented, does not imply that these have been endorsed or recommended by FAO in preference to others of a similar nature that are not mentioned. -

Ten-Year Development Plan for Georgian Gas Transmission Network 2018-2027
Ten-Year Development Plan for Georgian Gas Transmission Network 2018-2027 October 2017 1 The document represents a 10-year Georgian gas transmission and related infrastructure development plan. It was prepared on the basis of 2016 and 2017 year editions of “10-Year Development Plan for Georgian Gas Transmission Infrastructure)’’, considering the actual situation of current period. The 10-year Gas Network Development Plan was discussed with the Georgian Gas Transportation Company, presented to the Ministry of Energy of Georgia, the Georgian National Energy Regulatory Commission and other stakeholders. Consultations regarding the information used in and information on the project implementation of the 10-year Gas Network Development Plan can be obtained from GOGC Strategic Planning and Projects Department. Head of the Department: Teimuraz Gochitashvili, Dr. Sci, professor, Tel: +(995 32) 2244040 (414); E-mail: [email protected] 2 Contents Abbreviations ...........................................................................................................................4 Executive summary ..................................................................................................................5 1. Introduction .....................................................................................................................7 1.1. General provisions............................................................................................................ 7 1.2. Formal and methodological basis for preparing the plan .............................................. -

MUNICIPAL WATER and WASTEWATER SECTOR in GEORGIA Status Report
MUNICIPAL WATER AND WASTEWATER SECTOR IN GEORGIA Status Report By David Melua 2015 Municipal Water and Wastewater Sector in Georgia, status Report Table of Content Current situation page 3 Institutional Setting page 6 Legal framework page 16 Key findings and conclusions page 21 Abbreviations GWP – Georgian Water and Power GEL – Georgian Lari GUWSC – Georgian United Water Supply Company USAID – US agency for international Development EIB – European Investment Bank ADB – Asian Development Bank A.R. - Autonomous Republic KfW - Kreditanstalt für Wiederaufbau MDF – Municipal Development Fund WED – Water Framework Directive AA – association Agreement 2 Municipal Water and Wastewater Sector in Georgia, status Report 1. Current Situation About 95% of the urban and 35% of the rural population is supplied by centralised water service. This indicates high network coverage by international standards. The actual performance of this system is a problem, however. Poor quality of the distribution network results in a water loss rate of 10-51%, and 40% water loss in Tbilisi. All urban households suffer interrupted supply, receiving water much less than 24 hours a day, in some cities as little as 8-10 hours a day. In rural areas the supply system often does not function at all. This affects mainly people living on higher floors of buildings, because of low pressure in the sys- tem. The major reason for that is the shortage of electricity supply due to a lack of payment and also physical shortages. The majority of the connected urban households can have potentially good water quality, as the main source is groundwater. Groundwater sources provide about 90% of the water supply apart from Tbilisi. -

GEORGIA Second Edition March 2010
WHO DOES WHAT WHERE IN DISASTER RISK REDUCTION IN GEORGIA Second edition March 2010 Georgian National Committee of Disaster Risk Reduction & Environment Sustainable Development FOREWORD Georgia is a highly disaster-prone country, which frequently experiences natural hazards (e.g. earthquakes, floods, landslides, mudflows, avalanches, and drought) as well as man-made emergencies (e.g. industrial accidents and traffic accidents). Compounding factors such as demographic change, unplanned urbanization, poorly maintained infrastructure, lax enforcement of safety standards, socio-economic inequities, epidemics, environmental degradation and climate variability amplify the frequency and intensity of disasters and call for a proactive and multi-hazard approach. Disaster risk reduction is a cross-cutting and complex development issue. It requires political and legal commitment, public understanding, scientific knowledge, careful development planning, responsible enforcement of policies and legislation, people-centred early warning systems, and effective disaster preparedness and response mechanisms. Close collaboration of policy-makers, scientists, urban planners, engineers, architects, development workers and civil society representatives is a precondition for adopting a comprehensive approach and inventing adequate solutions. Multi-stakeholder and inter-agency platforms can help provide and mobilize knowledge, skills and resources required for mainstreaming disaster risk reduction into development policies, for coordination of planning and programmes,