Recognition and Management of Oral Health Problems in Older Adults by Physicians: a Pilot Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
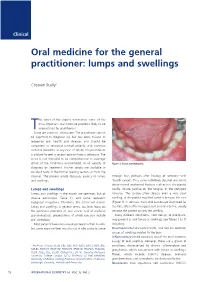
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
CHILDHOOD DEVELOPMENTAL SCREENING 2020 https://doi.org/10.33591/sfp.46.5.up1 FINDING A MASS WITHIN THE ORAL CAVITY: WHAT ARE THE COMMON CAUSES AND 4-7 GAINING INSIGHT: WHAT ARE THE ISSUES? In Figure 2 below, a list of masses that could arise from each site Figure 3. Most common oral masses What are the common salivary gland pathologies Salivary gland tumours (Figure 7) commonly present as channel referrals to appropriate specialists who are better HOW SHOULD A GP MANAGE THEM? of the oral cavity is given and elaborated briey. Among the that a GP should be aware of? painless growing masses which are usually benign. ey can equipped in centres to accurately diagnose and treat these Mr Tan Tai Joum, Dr Marie Stella P Cruz CDR had a slow-growing mass in the oral cavity over one year more common oral masses are: torus palatinus, torus occur in both major and minor salivary glands but are most patients, which usually involves surgical excision. but sought treatment only when he experienced a sudden acute mandibularis, pyogenic granuloma, mucocele, broma, ere are three pairs of major salivary glands (parotid, commonly found occurring in the parotid glands. e most 3) Salivary gland pathology may be primary or secondary to submandibular and sublingual) as well as hundreds of minor ABSTRACT onset of severe pain and numbness. He was fortunate to have leukoplakia and squamous cell carcinoma – photographs of common type of salivary gland tumour is the pleomorphic systemic causes. ese dierent diseases may present with not sought treatment as it had not caused any pain. -

Prevalence of Oral Lesions in Complete Denture Wearers- an Original Research
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 20, Issue 1 Ser.3 (January. 2021), PP 29-33 www.iosrjournals.org Prevalence of oral lesions in complete denture wearers- An original research Prenika Sharma1*, Reecha Gupta2 1- MDS, Oral medicine and radiology 2- Professor and HOD Department of Prosthodontics, Indira Gandhi Govt. Dental College, Jammu (J&K) Abstract: Background: Complete denture patients are often associated with the various denture-related oral mucosallesions. The purpose of this study is to evaluate the prevalence ofdenture-related oral mucosal lesions in complete denture patients. Materials and Methods: The study was consisted of 225 patientshaving various denture-induced oral mucosal lesions from theoutpatient department of the department out of the 395 completedenture patients examined. Data related to gender, age, length ofdenture use, hygiene care were obtained. All the data were tabulated and analyzed. Results: In 225 complete denture patients. Denture stomatitis (60.23%) was the most commonlesion present, followed by Epulis fissuratum and angularcheilitis. The denture-induced oral mucosal lesions werefound more common in age >40 years (59.78%) and in female(52.70%) complete denture wearer patients. Conclusion: The present studies showed that oral lesions associated with wearing denture are prevalent and create health problems that impact the quality of life of dental patients. Key Words: Complete denture, denture stomatitis, Epulis fissuratum, oralmucosal lesions. --------------------------------------------------------------------------------------------------------------------------------------- Date of Submission: 26-12-2020 Date of Acceptance: 07-01-2021 --------------------------------------------------------------------------------------------------------------------------------------- I. Introduction Edentulism may be the last sequel of periodontal diseases and dental caries. In case of older adults, edentulism is essential as a correlate of self-esteem and quality of life. -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -

Application of Lasers in Treatment of Oral Premalignant Lesions
Symbiosis www.symbiosisonline.org www.symbiosisonlinepublishing.com Review article Journal of Dentistry, Oral Disorders & Therapy Open Access Application of Lasers in Treatment of Oral Premalignant Lesions Amaninder Singh*1, Akanksha Zutshi2, Preetkanwal Singh Ahluwalia3, Vikas Sharma4 and Vandana Razdan5 1,4oral and maxillofacial surgery, reader, National Dental College and Hospital, Dera Bassi, Punjab 2oral and maxillofacial surgery, senior lecturer, National Dental College and Hospital, Dera Bassi, Punjab 3oral and maxillofacial surgery, professor, National Dental College and Hospital, Dera Bassi, Punjab 5Pharmacology, professor, Govt. Medical College and Hospital, Jammu Received: April 03, 2018; Accepted: June 04, 2018; Published: June 11, 2018 *Corresponding author: Amaninder Singh, House No- 620, Phase- 6, mohali, 160055, E-mail address: [email protected] Abstract radiation. Laser systems and their application in dentistry and especially the basis of energy of the beam and wavelength of the emitted oral surgery are rapidly improving today. Lasers are being used as a niche tool as direct replacement for conventional approaches ClassificationGas lasers of lasers [6] CO advantages of lasers are incision of tissues, coagulation during Argon like scalpel, blades, electro surgery, dental hand piece. The specific Liquid Dyes2 canoperation be used and for treatmentpostoperative of conditions benefits likesuch lowas premalignant postoperative lesions, pain, better wound healing. For soft tissue oral surgical procedures lasers Solid -
Management of Epulis Fissuratum Using Cryosurgery - a Case Report
CASE REPORT Management of Epulis Fissuratum Using Cryosurgery - A Case Report Pradeep Sharma, Daksh Goel, Rajarshi Ghosh, Balram Garg Department of Oral and Maxillofacial Surgery, I.T.S Dental College, Ghaziabad, Uttar Pradesh, India Email for correspondence: [email protected] ABSTRACT The aim of the present case report is to present a case showing the treatment of Epulis fissuratum in relation to an ill-fitting denture treated with nitrous oxide cryosurgery. Epulis fissuratum associated with an ill-fitting denture greatly hinders mastication and produces discomfort and pain to the patient. The nitrous oxide cryosurgery can be used effectively in its management, due to its excellent hemorrhage control and post-operative healing. A 64-year- old male reported with Epulis fissuratum in the maxillary anterior vestibular sulcus, which was associated with an ill-fitting denture. Nitrous oxide cryosurgery was used for the treatment of the lesion. During the procedure, nil hemorrhage was achieved, and the post-operative healing was satisfactory. Nitrous oxide cryosurgery, hence, can be used effectively as it has the boon of achieving excellent hemostasis, good healing with minimal post-operative edema and pain, and maintaining an aseptic environment. This technique can be effectively used in the treatment of Epulis fissuratum besides it can also be used in the treatment of other oral soft tissue pathologies achieving a plethora of benefits. Key words: Epulis fissuratum, hemorrhage control, nitrous oxide cryosurgery, soft tissue lesion INTRODUCTION dentures have potential to cause oral carcinoma.[2] A poorly fitted prosthesis can give rise to a Hence, ill-fitting dentures and its sequelae should plethora of problems, notably Epulis fissuratum, not be overlooked. -

Oral Cancer in Its Early Stage, When Treatment May Be Most Effective
Clinical Showcase This month’s Clinical Showcase highlights common oral conditions that should be included in the differential diagnosis for squamous cell carcinoma or salivary gland tumours. The author sounds a cautionary note about the dangers of misdiagnosing oral lesions and reminds oral health professionals that they can detect oral cancer in its early stage, when treatment may be most effective. Clinical Showcase is a new section that features case demonstrations of clinical problems encountered in dental practice. If you would like to propose a case or recommend a clinician who could contribute to Clinical Showcase, contact editor-in-chief Dr. John O’Keefe at [email protected]. Oral Cancer John G.L. Lovas, DDS, MSc, FRCD(C) Practising dentists should concentrate on competently morbidity. Instead, radiation therapy was curative, leaving diagnosing and treating routine conditions like caries, minimal local scarring. Patients can remain completely gingivitis, periodontitis, malocclusion and tooth loss. unaware of surprisingly large intraoral lesions if the lesions However, dentists and dental hygienists are also in the best are slow-growing and asymptomatic. Unfortunately, even position to detect and diagnose relatively rare and life- when patients become aware of an intraoral lesion, they threatening oral lesions such as carcinoma. The dental team often erroneously assume that if it’s painless, it’s not danger- should therefore always maintain a high index of suspicion. ous. The patient with the mucoepidermoid carcinoma in The cases presented here highlight some of the key factors Fig. 4 had been aware of the asymptomatic swelling for essential for the early detection and most effective treat- 18 months. -

Epulis Fissuratum
Clinical Image World Journal of Oral and Maxillofacial Surgery Published: 03 Dec, 2018 Epulis Fissuratum Acevedo Ocana R1, Amez Descalzo S1, Cortes-Breton Brinkmann J2*, Delgado Gregori J1 and Sanchez Jorge MI1 1Department of Oral Surgery and Implantology, Alfonso X EI Sabio University, Spain 2Department of Oral Surgery and Implantology, Hospital Virgen de la Paloma, Spain Clinical Image A female patient aged 78 years attended the clinic pertaining to the Master’s Program in Oral Surgery, Implant Dentistry, and Periodontics at the Alfonso X Ei Sabio University (Madrid, Spain), presenting a tumor over the mandibular alveolar ridge at the midline (Figure 1). The patient did not report any family or personal antecedents of relevance. The development of the tumor appeared to be related to recent rehabilitation with implant retained overdentures retained with locator attachments (Figure 2). During intraoral exploration, a pedunculated lesion was found of fibrous consistency and whitish color with an ulcerated surface, which the patient found painful during function. It was decided to perform excisional biopsy. After obtaining informed consent from the patient, local anesthesia was applied with a supraperiosteal and perilesional infiltration technique, excision of the lesion by cold knife cone technique was performed, followed by cauterization with an electric scalpel (Figure 3 and 4). The sample was placed in a 10% formal saline for histopathological analysis. The anatomopathological report described the entity microscopically as a lesion with densely fibrous paucellular connective stroma around a vascular axis. The polypoid structure showed a covering of non-keratinized mature squamous epithelium. No signs of malignancy were observed. The pathologist’s diagnosis was of traumatic (fibroepithelial polyp) fibroma/epulis fissuratum. -

Oral Health and Disease
Downloaded from bmj.com on 19 August 2005 ABC of oral health: Oral health and disease Ruth Holt, Graham Roberts and Crispian Scully BMJ 2000;320;1652-1655 doi:10.1136/bmj.320.7250.1652 Updated information and services can be found at: http://bmj.com/cgi/content/full/320/7250/1652 These include: Rapid responses One rapid response has been posted to this article, which you can access for free at: http://bmj.com/cgi/content/full/320/7250/1652#responses You can respond to this article at: http://bmj.com/cgi/eletter-submit/320/7250/1652 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at service the top right corner of the article Topic collections Articles on similar topics can be found in the following collections Dentistry and Oral Medicine (79 articles) Notes To order reprints of this article go to: http://www.bmjjournals.com/cgi/reprintform To subscribe to BMJ go to: http://bmj.bmjjournals.com/subscriptions/subscribe.shtml Clinical review Downloaded from bmj.com on 19 August 2005 ABC of oral health Oral health and disease Ruth Holt, Graham Roberts, Crispian Scully A healthy dentition and mouth is important to both quality of life and nutrition, and oral disease may affect systemic health, as Enamel covering crown Gingival crevice discussed in later articles in this series. (gingival sulcus) Dentine Development of the dentition Gingiva Pulp chamber Teeth form mainly from neuroectoderm and comprise a crown of insensitive enamel surrounding sensitive dentine and a root Periodontal ligament that has no enamel covering. -

Oral Mucosal Disorders
IN THE NAME OF GOD DR MARYAM BASIRAT ASSISTANT PROFESSOR OF GUILAN UNIVERSITY OF MEDICAL SCIENCES Oral Mucosal lesions in old adult Changes of oral mucosa in old adults Etiology: Trauma Mucosal disease Habits Salivary gland hypofunction Oral mucosal disorders Declining immunologic responsiveness oral and systemic disorders use of medications Oral epithelium in old adults thinner loses elasticity atrophies with age Most common oral lesions among elderly Traumatic lesions lichen planus and lichenoid reactions inflammatory lesions candidiasis vesiculobullous conditions Premalignant and malignant lesions Traumatic ulcer Most common lesions in old patients the labial and buccal mucosa Cause: habits, motor dysfunction, pressure necrosis, improper hygiene shallow ulcerations with a necrotic center Treatment: identifying the etiology and removing it Palliation with topical emollients and anesthetics no resolution occurs within a two-week time period: incisional biopsy lichen planus and lichenoid reactions common ulcerative disorders of the oral mucosa etiology : OLP: idiopathic or virally induced LR: medication, dental material T-cell–mediated chronic inflammatory response malignant transformation: chronic OLP more frequent recalls in patients with desquamative gingivitis Desquamative gingivitis Inflammatory lesions often as a result of poorly fitting dentures Papillary hyperplasia: cobble stone appearance Epulis fissuratum :hyperplastic granulation tissue surrounds the denture flange Candidiasis Due to systemic -

Intro to OMFS
OMFS I Course Review Enoch Ng, DDS 2014 Intro to OMFS Dentoalveolar surgery - Basic – GP able - Advanced – OMFS specialist o Extraction of erupted o Surgical extraction impacted teeth o Minor preprosthetic surgeries o Advanced preprosthetic surgeries Preprosthetic surgeries Anesthesia - Alveoloplasty - Local - Tori removal - Nitrous oxide - Vestibuloplasty – usually increase denture flange - Moderate sedation - Epulis fissuratum removal o Requires additional training for the GP - Tuberosity reduction - Deep sedation and general anesthesia – specialist - Sinus augmentation (pre-implant surgeries) o Residency in OMFS or dental anesthesia Pathology - Benign – fibroma, dentigerous cyst - Benign aggressive – OMFS only – ameloblastoma, reconstruction via bone grafting, etc - Malignant – OMFS oncology subspecialist only – squamous cell carcinoma Trauma - Dentoalveolar – related to teeth and surrounding structures - Craniofacial – trauma to mandible, maxilla/midface (zygoma), orbits, frontal bones/sinus – OMFS only - Mandibular - Midface - Upper facial Surgeries Orthognathic – move Mx, Mn, or both TMJ - Mx – lefort Class I - Arthroscopy – scope in joint, inject steroids, etc - Mn – bilateral saggital split ramus osteotomy - Arthroplasty - Total joint replacement CLP Cosmetic - Cleft lip closure, secondary cleft lip closure - Blepharoplasty – eye lid surgery - Alveolar/primary palatal cleft closure - Brow lifting - Nasal surgeries - Botox/fillers - Adjunct procedures – orthognathic surgery, - Face/neck lifting implant reconstruction - Rhinoplasty