WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
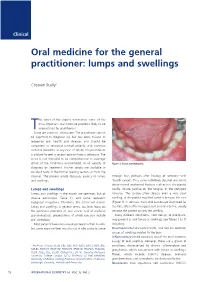
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Salivary Gland Tumours in Tanzania M. I. Masanja, B. M
August 2003 EAST AFRICAN MEDICAL JOURNAL 429 East African Medical Journal Vol. 80 No. 8. August 2003 SALIVARY GLAND TUMOURS IN TANZANIA M.I. Masanja, DDS, B. M. Kalyanyama, DDS, PhD and E. N. M. Simon, DDS, Dipl. (Oral Radiol.), Faculty of Dentistry, Muhimbili University College of Health Sciences, P.O. Box 65014, Dar es Salaam, Tanzania Requests for reprints to: Dr. E. N. M. Simon, Faculty of Dentistry, Muhimbili University College of Health Sciences, P.O. Box 65014, Dar es Salaam, Tanzania SALIVARY GLAND TUMOURS IN TANZANIA M. I. MASANJA, B. M. KALYANYAMA and E. N. M. SIMON ABSTRACT Objective: To determine the pattern of occurrence of salivary gland tumours in Tanzania over a period of twenty years. Design: Cross-sectional retrospective study. Setting: Two referral centres; Muhimbili National Hospital (MNH) and Kilimanjaro Christian Medical Centre (KCMC). Methods: Medical records of patients who presented with tumours of the salivary glands in the two major referral centres over a period of twenty years from 1982 to 2001 were reviewed. Data regarding demographic, clinical and histologic information was analysed. Results: Salivary gland tumours constituted 6.3% of all oral-facial tumours and tumour like lesions. Among the salivary gland tumours, 54% were benign and 46% malignant, which occurred in 80 males and 53 females. Peak age was between 20 and 49 years, with a male- female ratio of 1.5:1 (p< 0.05). Pleomorphic adenoma was the commonest occurring tumour (44.4%) followed by adenoid cystic carcinoma (24.8%), mucoepidermoid carcinoma (9.8%) and adenocarcinoma (6.5%). Among the benign tumours, pleomorphic adenoma dominated (83.9%), followed by adenoma (9.9%). -
ACATS Code Book 2019-2021
Contact [email protected] with questions or comments ACATS Alberta Coding Access Targets for Surgery Go-live date: April 1, 2021 Facing us: Dr. Wynn James, orthopedic surgeon, Edmonton. ACATS Code Book Viewer – ACATS codes at your fingertips with smart-search capability. To link to the viewer, please visit the at ACATS website https://www.albertahealthservices.ca/scns/Page12961.aspx Next scheduled revision release April 1, 2023 514781 ACATS Cover.indd 1 2/22/2021 3:09:47 PM Alberta Coding Access Targets for Surgery 2/23/2021 2:42:10 PM2/23/2021 2:42:10 PM ACATS Codes 2021-2023 The 2019-2021 ACATS code review cycle resulted in the largest update of codes in the nine-year history. This was a considerable change tracking effort with great surgeon engagement from all five zones in the province. ACATS strives to be a scheduled surgery coding system for surgeons, built by surgeons. I, and all the ACATS Leads across the province thank everyone for their efforts. This code review cycle brought in new oversight to the ACATS code review. The Provincial Surgical Operations Committee (PSOC) provided guidance in the development of the ACATS priority description framework for the code review, finding code review surgeon designates for each service, and the final approval of all the ACATS code changes. PSOC membership includes the surgical leadership Bryan Atwood ACATS Provincial Lead from each zone (Clinical Operations, Surgical Zone Lead, Anaesthesia Zone Lead). A Why so many changes this time around? The ACATS priority description tool was updated and used by all services to review the codes. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Characteristics of Salivary Gland Tumours in the United Arab Emirates
Characteristics of salivary gland tumours in the United Arab Emirates Yasir Al Sarraj1, Satish Chandrasekhar Nair2, Ammar Al Siraj3 and Maher AlShayeb4 1, 4Ajman University of Science and Technology, Department of Oral and Maxillofacial Surgery, Post Box 346, United Arab Emirates 2Tawam Hospital- Johns Hopkins Medicine International Affiliate, Department of Academic Affairs-Medical Research, Post Box 15258, Al Ain, United Arab Emirates 3Mawi Medical Centre, Post Box 55510, Dubai, United Arab Emirates Correspondence to: Satish Chandrasekhar Nair. Email: [email protected] Abstract Salivary gland tumours (SGT) are relatively rare cancers characterised by striking morphological diversity and wide variation in the global distribution of SGT incidence. Given the proximity to the head and neck structures, management of SGT has been clinically difficult. To the best of our knowledge, there are no epidemiological studies on SGT from the United Arab Emirates (UAE) or the Gulf Cooperation Council Countries (GCC). Patient charts (N = 314) and associated pathological records were systematically reviewed between the years 1998–2014. Predominance of benign (74%) compared with malignant (26%) SGT was observed. Among the 83 malignant SGT identified, frequency was higher in males (61%) than in females (39%) and peak occurrence was in the fifth decade of life. Mucoepidermoid carcinoma was the most common type of tumour (35%) followed by adenoid cystic carcinoma (18.1%) and acinar cell carcinoma (10.8%). A similar pattern of tumour distribution was seen in patients from GCC, Asian, and Middle East countries. This is the first report to address the distri- Research bution of salivary gland tumours in a multiethnic, multicultural population of the Gulf. -

Oral Mucocele – Diagnosis and Management
Journal of Dentistry, Medicine and Medical Sciences Vol. 2(2) pp. 26-30, November 2012 Available online http://www.interesjournals.org/JDMMS Copyright ©2012 International Research Journals Review Oral Mucocele – Diagnosis and Management Prasanna Kumar Rao 1, Divya Hegde 2, Shishir Ram Shetty 3, Laxmikanth Chatra 4 and Prashanth Shenai 5 1Associate Professor, Department of Oral Medicine and Radiology, Yenepoya Dental College, Yenepoya University, Deralakatte, Nithyanandanagar Post, Mangalore, Karnataka, India. 2Assistant Professor, Department of Obstetrics and Gynecology, AJ Institute of Medical Sciences, Mangalore, Karnataka, India. 3Reader, Department of Oral Medicine and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Mangalore, Karnataka, India. 4Senior Professor and Head, Department of Oral Medicine and Radiology, Yenepoya Dental College, Yenepoya University, Deralakatte, Nithyanandanagar Post, Mangalore, Karnataka, India. 5Senior Professor, Department of Oral Medicine and Radiology, Yenepoya Dental College, Yenepoya University, Deralakatte, Nithyanandanagar Post, Mangalore, Karnataka, India. ABSTRACT Mucocele are common salivary gland disorder which can be present in the oral cavity, appendix, gall bladder, paranasal sinuses or lacrimal sac. Common location for these lesions in oral cavity is lower lip however it also presents on other locations like tongue, buccal mucosa, soft palate, retromolar pad and lower labial mucosa. Trauma and lip biting habits are the main cause for these types of lesions. These are painless lesions which can be diagnosed clinically. In this review, a method used for searching data includes various internet sources and relevant electronic journals from the Pub Med and Medline. Keywords: Mucocels, Lower lip, Retention cyst. INTRODUCTION Mucocele is defined as a mucus filled cyst that can Types appear in the oral cavity, appendix, gall bladder, paranasal sinuses or lacrimal sac (Baurmash, 2003; Clinically there are two types, extravasation and retention Ozturk et al., 2005). -
Mandibular Tori
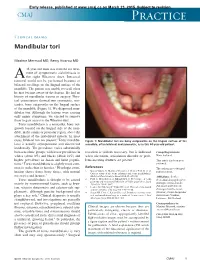
Early release, published at www.cmaj.ca on March 23, 2015. Subject to revision. CMAJ Practice Clinical images Mandibular tori Maxime Mermod MD, Remy Hoarau MD 44-year-old man was referred for treat- ment of symptomatic sialolithiasis in A the right Wharton duct. Intraoral removal could not be performed because of bilateral swellings on the lingual surface of the mandible. The patient was unable to recall when he first became aware of the lesions. He had no history of mandibular trauma or surgery. Phys- ical examination showed two symmetric, non- tender, bony outgrowths on the lingual surface of the mandible (Figure 1). We diagnosed man- dibular tori. Although the lesions were causing only minor symptoms, we elected to remove them to gain access to the Wharton duct. Torus mandibularis is a nontender, bony out- growth located on the lingual side of the man- dible, in the canine or premolar region, above the attachment of the mylohyoid muscle. In most 1 cases, bilateral tori are present. Torus mandibu- Figure 1: Mandibular tori are bony outgrowths on the lingual surface of the laris is usually asymptomatic and discovered mandible, often bilateral and symmetric, as in this 44-year-old patient. incidentally. The prevalence varies substantially between ethnic groups, with lower prevalence in resection is seldom necessary, but is indicated Competing interests: whites (about 8%) and blacks (about 16%) and when ulceration, articulation disorder or prob- None declared. higher prevalence in Asian and Inuit popula- lems inserting dentures are present.3 This article has been peer tions.2 Torus mandibularis is slightly more com- reviewed. -

Gene Expression Helps to Characterise Benign And
Winter et al. BMC Cancer 2012, 12:465 http://www.biomedcentral.com/1471-2407/12/465 RESEARCH ARTICLE Open Access Human α-defensin (DEFA) gene expression helps to characterise benign and malignant salivary gland tumours Jochen Winter1, Annette Pantelis2, Dominik Kraus3, Jan Reckenbeil4, Rudolf Reich4, Soeren Jepsen1, Hans-Peter Fischer5, Jean-Pierre Allam6, Natalija Novak6 and Matthias Wenghoefer4* Abstract Background: Because of the infrequence of salivary gland tumours and their complex histopathological diagnosis it is still difficult to exactly predict their clinical course by means of recurrence, malignant progression and metastasis. In order to define new proliferation associated genes, purpose of this study was to investigate the expression of human α-defensins (DEFA) 1/3 and 4 in different tumour entities of the salivary glands with respect to malignancy. Methods: Tissue of salivary glands (n=10), pleomorphic adenomas (n=10), cystadenolymphomas (n=10), adenocarcinomas (n=10), adenoidcystic carcinomas (n=10), and mucoepidermoid carcinomas (n=10) was obtained during routine surgical procedures. RNA was extracted according to standard protocols. Transcript levels of DEFA 1/3 and 4 were analyzed by quantitative realtime PCR and compared with healthy salivary gland tissue. Additionally, the proteins encoded by DEFA 1/3 and DEFA 4 were visualized in paraffin-embedded tissue sections by immunohistochemical staining. Results: Human α-defensins are traceable in healthy as well as in pathological altered salivary gland tissue. In comparison with healthy tissue, the gene expression of DEFA 1/3 and 4 was significantly (p<0.05) increased in all tumours – except for a significant decrease of DEFA 4 gene expression in pleomorphic adenomas and a similar transcript level for DEFA 1/3 compared to healthy salivary glands. -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -
Sublingual Epidermoid Cyst Resembling Sublingual Ranula: a Case Report
Archives of Orofacial Sciences The Journal of the School of Dental Sciences Universiti Sains Malaysia Arch Orofac Sci (2015), 10(1). Article No. 0204. 6 pages. Case Report Sublingual epidermoid cyst resembling sublingual ranula: a case report Tan Shi Nee a, Roszalina Ramli b, Primuharsa Putra Sabir Husin Athar c* a Dept. of Otorhinolarygology-Head & Neck Surgery, School of Medicine, KPJ Healthcare University College, Malaysia. b Department of Oral & Maxillofacial Surgery, Universiti Kebangsaan Malaysia. c Ear, Nose & Throat-Head & Neck Consultant Clinic, KPJ Seremban Specialist Hospital/ KPJ Healthcare University College, Negeri Sembilan, Malaysia. * Corresponding author: [email protected] Submitted: 18/11/2014. Revised edition: 23/02/2015. Accepted: 12/05/2015. Published online: 13/05/2015. Abstract Dermoid cysts are anatomic embryonic abnormalities that are rarely seen in the oral cavity. Histologically, they are further classified as epidermoid, dermoid or teratoid. We report a case in which an 18- year-old girl who developed an epidermoid cyst presenting as a large sublingual swelling occupying the entire floor of the mouth causing snoring and speech difficulty. We emphasized on the clinical steps in achieving an accurate diagnosis, possible differential diagnosis, necessary imaging techniques and management of epidermoid cyst. Keywords: enucleation, epidermoid cyst, ranula, sublingual. Introduction Dermoid cyst can be classified as congenital or acquired. A lot of Dermoid cyst is a benign cystic malformation etiopathogenesis theories have been that is rarely seen in the oral cavity (Jham et reported which includes dysontogenetic, al., 2007). It represents less than 0.01% of traumatic, and thyroglossal anomaly (Jham all oral cavity cysts (Verma et al., 2012; De et al., 2007; Verma et al., 2012). -

Recognition and Management of Oral Health Problems in Older Adults by Physicians: a Pilot Study
J Am Board Fam Pract: first published as 10.3122/jabfm.11.6.474 on 1 November 1998. Downloaded from BRIEF REPORTS Recognition and Management of Oral Health Problems in Older Adults by Physicians: A Pilot Study Thomas V. Jones, MD, MPH, Mitchel J Siegel, DDS, andJohn R. Schneider, A1A Oral health problems are among the most com of the nation's current and future health care mon chronic health conditions experienced by needs, the steady increase in the older adult popu older adults. Healthy People 2000, an initiative to lation, and the generally high access elderly per improve the health of America, has selected oral sons have to medical care provided by family health as a priority area. l About 11 of 100,000 physicians and internists.s,7,8 Currently there is persons have oral cancer diagnosed every year.2 very little information about the ability of family The average age at which oral cancer is diagnosed physicians or internists, such as geriatricians, to is approximately 65 years, with the incidence in assess the oral health of older patients. We con creasing from middle adulthood through the sev ducted this preliminary study to determine how enth decade of life. l-3 Even though the mortality family physicians and geriatricians compare with rate associated with oral cancer (7700 deaths an each other and with general practice dentists in nually)4 ranks among the lowest compared with their ability to recognize, diagnose, and perform other cancers, many deaths from oral cancer initial management of a wide spectrum of oral might be prevented by improved case finding and health problems seen in older adults.