Meeting Record
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Army Container Operations
FM 55-80 ARMY CONTAINER OPERATIONS DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited. HEADQUARTERS, DEPARTMENT OF THE ARMY FM 55-80 FIELD MANUAL HEADQUARTERS No. 55-80 DEPARTMENT OF THE ARMY Washington, DC, 13 August 1997 ARMY CONTAINER OPERATIONS TABLE OF CONTENTS Page PREFACE.......................................................................................................................... iv CHAPTER 1. INTRODUCTION TO INTERMODALISM .......................................... 1-1 1-1. Background.................................................................................... 1-1 1-2. Responsibilities Within the Defense Transportation System............. 1-1 1-3. Department of Defense ................................................................... 1-2 1-4. Assistant Deputy Under Secretary of Defense, Transportation Policy............................................................................................. 1-2 1-5. Secretary of the Army..................................................................... 1-2 1-6. Supported Commander in Chiefs..................................................... 1-2 1-7. Army Service Component Commander............................................ 1-2 1-8. Commanders .................................................................................. 1-2 1-9. United States Transportation Command .......................................... 1-3 1-10. Military Traffic Management Command ......................................... 1-3 1-11. Procurement and Leasing -

Railcars at Rocky Flats Community Final 11-04-04.Indd
Rocky Flats Fact Sheet Transporting low-level radioactive waste from Rocky Flats using railcars Transporting low-level radioactive waste from Rocky Flats using railcars The Rocky Flats Closure Project is one of the largest environmental cleanup operations in the world. Rocky Flats, located approximately 15 miles northwest of Denver, produced plutonium and uranium components for the U.S. nuclear weapons program from 1953 until 1989. The operations left a legacy of radioactive and hazardous waste contamination. Cleanup operations began in earnest in 1995. As part of closure, all radioactive and hazardous waste will be shipped from Rocky Flats to waste disposal sites in other states. No waste will be permanently stored or disposed of on site. Currently, all low-level radioactive waste leaving Rocky Flats is transported by truck. As the Rocky Flats Closure Project Cleaning up Rocky Flats will return thousands of acres to the citizens of Colorado. The nears completion, demolition of former site will become a national wildlife refuge. manufacturing buildings signifi cantly increases the volume of low-level radioactive waste. To improve effi ciency and worker safety, the project will use railcars to ship very low-level waste to the Envirocare disposal facility in Utah. Using rail may eliminate as many as 5,000 truck shipments. Background The complex job of cleaning up and closing down Rocky Flats involves removing massive quantities of radioactive waste. To date, after nine years of shipping, Rocky Flats has safely shipped approximately 260,000 cubic meters (65 percent) of the projected 400,000 cubic meters of radioactive waste that will be generated during closure. -

Analysis and Prospects of Container and Rail Transport
MATEC Web of Conferences 329, 01014 (2020) https://doi.org/10.1051/matecconf/202032901014 ICMTMTE 2020 Analysis and prospects of container and rail transport Sergey Vakulenko1,*, Pyotr Kurenkov1, Dmitry Romensky1 , Kirill Kalinin1, and Jozef Gašparík2 1Department of Transport business management and intelligent systems, Russian University of Transport, Moscow, Obraztsova str., 9, building 9, 127994. Russia 2Faculty of Operation and Economics of Transport and Communications, Zilina, Univerzitná 8215/1, 010 26, Republic of Slovakia Abstract. The article studies the main trends in the market of container transportation in rolling stock of various types, considers the process of transporting large-capacity containers in open wagons. The operational and economic aspects of removing administrative restrictions on the implementation of this type of transportation are noted. The dynamics of rental rates for rental of gondola cars and platforms in 2019-2020 is present. The summary characteristics of the gondola car fleet and fitting platforms on the Russian Railways network have been study. The analysis of the market share of the largest owners of gondola cars and fitting platforms was carry out. The advantages and disadvantages of using the technology of container transportation in open wagons are list. Solutions are propose to create a competitive environment in the container transportation segment of the transport services market. 1 Introduction Currently, containers are transport on fitting platforms, but theoretically, according to international rules, they can also be transport in open wagons: 40-feet - horizontally per piece, 20-feet - two each, and empty 20-feet - even three. From December 1, 2014, the local technical conditions (LTC) for the placement and fastening of universal containers in gondola cars with unloading hatches were cancel. -
Appendix I – Container/Equipment Description Codes
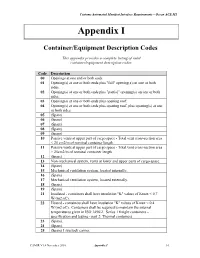
Customs Automated Manifest Interface Requirements – Ocean ACE M1 Appendix I Container/Equipment Description Codes This appendix provides a complete listing of valid container/equipment description codes. Code Description 00 Openings at one end or both ends. 01 Opening(s) at one or both ends plus "full" opening(s) on one or both sides. 02 Opening(s) at one or both ends plus "partial" opening(s) on one or both sides. 03 Opening(s) at one or both ends plus opening roof. 04 Opening(s) at one or both ends plus opening roof, plus opening(s) at one or both sides. 05 (Spare) 06 (Spare) 07 (Spare) 08 (Spare) 09 (Spare) 10 Passive vents at upper part of cargo space - Total vent cross-section area < 25 cm2/m of nominal container length. 11 Passive vents at upper part of cargo space - Total vent cross-section area > 25cm2/m of nominal container length. 12 (Spare) 13 Non-mechanical system, vents at lower and upper parts of cargo space. 14 (Spare) 15 Mechanical ventilation system, located internally. 16 (Spare) 17 Mechanical ventilation system, located externally. 18 (Spare) 19 (Spare) 21 Insulated - containers shall have insulation "K" values of Kmax < 0.7 W/(m2.oC). 22 Heated - containers shall have insulation "K" values of Kmax < 0.4 W/(m2.oC). Containers shall be required to maintain the internal temperatures given in ISO 1496/2. Series 1 freight containers – specification and testing - part 2: Thermal containers. 23 (Spare). 24 (Spare). 25 (Spare) Livestock carrier. CAMIR V1.4 November 2010 Appendix I I-1 Customs Automated Manifest Interface Requirements – Ocean ACE M1 Code Description 26 (Spare) Automobile carrier. -

An Inventory of Its Freight Car Specifications at the Minnesota
NP Mechanical Dept. Freight Car Specifications Spec. No. Description Dates C-O Hicks Double Deck Car 1886 C-l Standard Stock Car Body 1885 C-2 Standard Fruit Car 1890 c-3 Flat Bottom Gondola 1905 C-4 Standard Box Car 1883 c-21 Standard Box Car - Roller Bearing 1886-1889 C-22 Standard Caboose Truck 1888-1890 C-23 Standard Caboose Car Body 1886 C-23 40' flat car - S.P.&D. R.R. C-24 Boarding Cars C-25 Roller Bearing Iron Truck C-27 Swing Motion Roller Bearing Truck c-28 Truck No. 3 C-35 Standard Stock Car Body 1888 C-65 Refrigerator Car 1888 C-67 Roller Bearing Truck 1889 C-68 Truck 1889 C-74 Flat Car 1890 C-82 Refrigerator Car 1890 C-85 Wheels 1890 C-1l8 Street's Stable Car 1892 C-120 Stock Car Truck 1892 C-122 34' Box Car 1892 C-133 41' Flat Car 1892 C-135 Roller Bearing Truck 1892 C-139 Roller Bearing Truck 1892 C-141 36' Box Car 1892 C-144 36' Stock Car 1892 C-146 36' Flat Car 1893 C-148 Roller Bearing Stock Car Truck 1893 C-155 Truck, 4" x 7" Journal 1893 C-163 41' Flat Car 1894 C-169 37' Box Car 1895 C-171 Metal Frame Truck with Roller Bearing 1895 C-173 42' Box Car 1895 C-182 Bolsters and spring seats 1896 C-183 Bolsters and spring seats 1897 F-4 42' Hart Convertible 1918 F-5 30' Twin Hopper 1898 F-6 40' Box Car 1906 F-8 41' Flat Car 1895 F-9 Rubber gaskets on doors 1889 F-I0 33'8" Box Car undated F-ll Low roller bearing truck 1900 F-13 36' Box Car 1900 F-14 32' Twin Hopper Coal Car 1900 F-15 22' Caboose undated F-16 80,000-lb. -

Equipment Specifications
EQUIPMENT SPECIFICATIONS cn.ca/equipment AUTOMOTIVE Vehicle Parts These cars are specially designed and equipped to carry vehicle parts. The largest, with a capacity of over 10,000 cubic feet, have doors opening to 20 feet for convenient loading and unloading. CANADIAN NATIONAL CNA 795008 AUTO PARTS BOXCAR PARTS AUTO AUTOMOTIVE / VEHICLE PARTS / VEHICLE PARTS / AUTOMOTIVE AUTO PARTS BOXCAR Car Description Car Series Load Capacity Door Size Inside Dimensions Tons Tonnes Cu. Ft. m3 Width Height Length Width Height Auto Parts Boxcar (60 ft.) DTI 25900-25935 77-84 7,100 201 201 16' 0" 12' 8" 60' 9" 9' 2" 12' 9" GTW 125017-125304 76-84 6,000 170 170 16' 0" 10' 8" - 10' 9" 59' 7" - 60' 8" 9' 2" 11' 2" GTW 306839-306916 62-64 6,222-6,347 176-180 176-180 10' 0" 10' 11" - 11' 3" 60' 8" - 60' 9" 9' 2" - 9' 4" 11' 2" - 11' 4" GTW 375550-376005 78-84 6,347-6,650 180-188 180-188 16' 0" 11' 0" 59' 7" - 60' 9" 9' 1" - 9' 2" 11' 6" - 11' 7" GTW 384000-384699 16-83 7,373-7,596 209-215 209-215 10' 0" - 16' 0" 12' 4" - 12' 9" 60' 9" 9' 1" - 9' 2" 12' 10" - 13' 2" CNA 799309-799729 62-81 6,200-6,636 176-188 176-188 10' 0" - 16' 1" 10' 11" - 11' 3" 60' 8" - 60' 9" 9' 2" - 9' 4" 11' 5" - 11' 7" Auto Parts Boxcar (86 ft.) DTI 26017-26897 48-68 10,000 283 283 20' 0" 12' 9" 86' 6" 9' 2" 12' 9" GTW 105702-105773 48-69 10,000 283 283 20' 0" 12' 9" 86' 6" 9' 2" 12' 9" GTW 126000-127134 46-71 10,000 283 283 20' 0" 12' 9" 84' 2" - 86' 6" 9' 2" 12' 9" GTW 305700-306573 49-72 10,000 283 283 20' 0" 12' 9" 84' 2" - 86' 6" 9' 2" 12' 9" GTW 378001-378250 37-45 10,000 283 283 20' 0" 12' 9" 86' 6" 9' 2" 12' 9" IC/ICG 680004-680137 68-70 10,000-10,151 283-287 283-287 20' 0" 12' 9" 86' 6" 9' 2" 12' 9" CNA 795000-795403 44-72 10,000-10,600 283-300 283-300 20' 0" 12' 9" 86' 6" 9' 2" 12' 3" - 12' 9" AUTOMOTIVE Finished Vehicles The workhorse of the industry, these enclosed double-deck auto carriers are used to transport vans and trucks as well as cars to CN's network of auto compounds. -

New Designs of Wagon
New Design of Wagons AK Khosla Jindal Rail Infrastructure Ltd. Presentation Outline Wagon Holding on IR Type of Wagons on IR Max Moving Dimensions & Fixed structures Design Criteria Drivers for New Wagon Designs Brief on Jindal Rail Infrastructure Ltd. Presentation Outline Wagon Holding on IR Type of Wagons on IR Max Moving Dimensions & Fixed structures Design Criteria Drivers for New Wagon Designs Brief on Jindal Rail Infrastructure Ltd. Wagon Holding on Indian Railways TYPE OF WAGON WAGONS TOTAL QTY. OPEN WAGON BOXN,BOXNHS,BOXNHL,BOXNLW,BOY,BOST,BO 1,37,360 STHSM2,BOXNLW, BOXNS COVERED WAGON BCNA, BCNHL, BCNAHS 70,239 FLAT WAGON BFNS,BRNA,BRN22.9,BRHNEHS, 11,694 HOPPER WAGON BOBYN,BOBYN22.9,BOBRN,BOBRNHS,BCFC,BO 25,196 BRNHSM1,BOBRNAL,BOBSN BRAKE VAN WAGON BVZI,BVZC,BVCM 5,982 TANK WAGON BTPN,BTPGLN,BTFLN 14,066 CONTAINER WAGON BLC/BLL 14,891 SPECIAL PURPOSE BCACBM (A-CAR/B-CAR), BOM, BWT & Others 6,780 WAGON Total 2,86,208 Presentation Outline Wagon Holding on IR Wagon Types on IR Max Moving Dimensions & Fixed structures Design Criteria Drivers for New Wagon Designs Brief on Jindal Rail Infrastructure Ltd. Wagon Types on Indian Railways OPEN WAGONS BOXNHL WAGON BOXNHS WAGON SALIENT FEATURE BOXNHL BOXNHS BOXNS BOY Material of Construction IRS M44, CRF IS 2062 E250 IS 2062 E450 BR IS:2062E250 A CU & section A CU CU IRSM41 Type of Commodity Coal Coal Coal minerals/ore Loading Top loading Top loading Top loading Top loading Unloading Side doors & Side doors & Tippling operation Or Grabber Tippling Grabber Grabber operation Length over head stock (mm) 10034 9784 9784 11000 Length over couplers (mm) 10963 10713 10713 11929 Length inside (mm) 10034 9784 9784 10990 Width inside/Width Overall (mm) 3022/3250 2950/3200 3111/3135 2924/3134 Height inside/Height(max.)from RL. -

Rolling Stock: Locomotives and Rail Cars
Rolling Stock: Locomotives and Rail Cars Industry & Trade Summary Office of Industries Publication ITS-08 March 2011 Control No. 2011001 UNITED STATES INTERNATIONAL TRADE COMMISSION Karen Laney Acting Director of Operations Michael Anderson Acting Director, Office of Industries This report was principally prepared by: Peder Andersen, Office of Industries [email protected] With supporting assistance from: Monica Reed, Office of Industries Wanda Tolson, Office of Industries Under the direction of: Deborah McNay, Acting Chief Advanced Technology and Machinery Division Cover photo: Courtesy of BNSF Railway Co. Address all communication to Secretary to the Commission United States International Trade Commission Washington, DC 20436 www.usitc.gov Preface The United States International Trade Commission (USITC) has initiated its current Industry and Trade Summary series of reports to provide information on the rapidly evolving trade and competitive situation of the thousands of products imported into and exported from the United States. Over the past 20 years, U.S. international trade in goods and services has risen by almost 350 percent, compared to an increase of 180 percent in the U.S. gross domestic product (GDP), before falling sharply in late 2008 and 2009 due to the economic downturn. During the same two decades, international supply chains have become more global and competition has increased. Each Industry and Trade Summary addresses a different commodity or industry and contains information on trends in consumption, production, and trade, as well as an analysis of factors affecting industry trends and competitiveness in domestic and foreign markets. This report on the railway rolling stock industry primarily covers the period from 2004 to 2009, and includes data for 2010 where available. -

LINK-BELT SPEEDER CORPORATION Cover Photo Link-Belt Speed Corporation Plan Administrative Offices Looking Southeast December 1948
LINK-BELT SPEEDER CORPORATION Cover Photo Link-Belt Speed Corporation Plan Administrative Offices Looking Southeast December 1948. (Courtesy of Carl & Mark Koehler History Center) HISTORY OF LINK-BELT SPEEDER CORPORATION by Eric Barr THE Louis Berger Group, INC. Designed by To The Letter Type & Design, Marion, Iowa Printed by J&A Printing, Hiawatha With special thanks to: The Carl and Mary Koehler History Center Maryls Svendsen, Iowa Department of Homeland Security and Emergency Management This project was produced under the terms of a Memorandum of Agreement pursuant to Section 106 of the National Historic Preservation Act, among the U.S. Department of Homeland Security’s Federal Emergency Management Agency, the State Historical Society of Iowa, Iowa Department of Homeland Security and Emergency Management, the City of Cedar Rapids, Cedar Rapids Historic Preservation Commission, and Preservation Iowa, regarding adverse effects to historic properties in Cedar Rapids, Linn County, Iowa. FEMA administered Federal disaster assistance through FEMA’s Public Assistance Program pursuant to the Robert T. Stafford Disaster Relief and Emergency Assistance Act for the demolition of historic properties damaged as a result of flooding in July 2008 that resulted in declared disaster DR-1763-IA. 2 HISTORY OF LINK-BELT SPEEDER CORPORATION The Link-Belt Speeder Corporation factory Milwaukee, and St. Paul Railroad. The company originated as the Ewart complex manufactured cranes, power The facility served as the administrative Manufacturing Company in 1874, in shovels, excavators, draglines, hoes and headquarters and primary factory for the Belle Plaine, Iowa. Two other companies pile drivers with multiple applications company’s heavy machinery division. -

Caboose Progress the Freighthouse So It Could Accept Visitors
Issue Number 57 San Luis Obispo, California Fall 2016 www.slorrm.com Museum open every Saturday 10:00 to 4:00; other times for groups by arrangement. Contact [email protected]. Recognition for Major Supporters A new board mounted in the exhibit hall identifies Last in the Train – But First On the List those who made major contributions to upgrading Caboose Progress the Freighthouse so it could accept visitors. Volunteers have given high priority to restoring form- er Southern Pacific bay window caboose #1886 –seats, flooring, painting, hardware, and fixtures—aiming for public tours by the Railroad Festival in October. Work has progressed with the support of several Museum and community members. Brad LaRose, Dennis Lynch, Dan Manion, and Bob Wilson in particular have spent many hours returning the heavily used and somewhat abused interior to near original condition. Cabooses accommodated freight conductors and brakemen, who worked with waybills and switch lists, monitored brake-line air pressure, kept an eye on the whole train, and protected the rear of the train. The body of a bay window caboose was narrower than a typical car, with the bay’s slanted end windows allowing a clear view of the train on even gradual curves. SP used bay window cabooses from the late 1940s through the end of the Tank Car Arrives at the Museum “caboose era” in the 1980s. Three photos by Glen Matteson Several years of searching, negotiating, and planning paid off July 29 when this former Southern Pacific tank car arrived at the Museum. Thanks to Curator Brad LaRose’s diligence, it was donated by Union Pacific Railroad. -

Business Personal Property Categories
Personal Property Main Categories In Alpha Order 1 Inventory Report as: Inventory Report as: Inventory Report as: Inventory Report as: Inventory Report as: Inventory Report as:Inventory Report as: ABRASION MACH General Equip ATF PUMP General Equip BED General Equip BREATHALYZER General Equip CARGO CONTAINER General Equip CLOTHES CONVEYER General Equip CRASH MAT General Equip AC EQUIP General Equip ATHLETIC EQUIP General Equip BED GRINDER General Equip BREWERY EQ Brewery CARICATURES Art CLUBHOUSE EQUIP General Equip CRATES General Equip ACROBATIC MAT General Equip ATM General Equip BEDDING General Equip BRICK SETTING MACH General Equip CARNIVAL EQUIPMENT General Equip COAL MILL General Equip CREDENZA Fixture ACTIVATOR EQ General Equip AUDIO EQUIP Electrical BEDDING BOX General Equip BROADCASTING EQUIP General Equip CARPET CLEANING MACHINE General Equip COAL TANK General Equip CREEPER WHEELS General Equip ACTIVITY GYM General Equip AUDIO INTERFACE General Equip BELL EQ General Equip BROILER General Equip CARPET SAMPLE HOLDERS General Equip COFFEE BINS General Equip CREMATORY General Equip ADA EQUIP General Equip AUTO PLATE General Equip BELT DRYER Tool BROILER HOOD General Equip CARPET STRETCHER General Equip COFFEE EQUIP Appliance CREW LOCKERS General Equip ADAPTER HARNESS General Equip AUTO PROCESSOR General Equip BELT MACHINE General Equip BRONZE SCULPTURES Art CARRIAGE General Equip COIN MACH General Equip CRIB General Equip ADAPTER KIT General Equip AUTO REFRACTOR General Equip BENCH Furniture BRUSH CLIPPER General Equip CARVER MACHINE -

The Heath Telegraphic Cipher for the Use of Flouring Mills
149 Digitized by the Internet Archive in 2010 with funding from Duke University Libraries http://www.archive.org/details/heathtelegraphicOOheat HEATH'S TELEGRAPHIC GIPHER THE HEATH TELEGRAPHIC CIPHER FOR THE USE OF FLOURING MILLS AND FLOUR MERCHANTS AND THEIR TRAVELING SALESMEN FOR THE ECONOMICAL AND SECRET TRANSMISSION OF BUSINESS TELEGRAMS SOLD ONLY BY G . M . HEATH AUTHOR AND PROPRIETOR LA CROSSE, WISCONSIN '• v \J 1 No. i— THIS CODE BOOK I S T H K PROP E RTY OF LISTMAN MILL CO M P A N Y LA CROSSE WISCONSIN AND IS LOANED TO ,'i^0~Zr-&X2sf, G . / /O ^.<^t>c/ ^C^c-t^ Qr?t l£&C.ei In loaning- this Code to Correspondents it is with the distinct understanding that it is only to be used in the interests of our joint business and to be remailed to us when we request. ..LIST. IMPANY., — SZC'Y. COPYRIGHTED 1900 By G. M. HEATH INDEX About selling- 84 Instructions Barrels A bout sales 84 Mill Feed 90 No. in wood 1 " Shipping 95 " J^s cotton 6 " "49s " 10 Jute sacks " "98s " 14 No of Barrels in 98s 22 " " " " 140s 26 " " l-16s " 18 Letters received 80 " " 98s jute 22 Markets 84 " " 14()s " 26 and brands 79 " " 1-I6s paper 31 Marks Middlings, White " " i/ s " 35 8 carloads 56 " "49s " 39 Bulk " tons 66 Bran 200s carloads 59 Bulk carloads 55 " tons 66 " tons 61 100s carloads 59 200s carloads 57 " tons 67 " tons 62 Mill Feed instructions 90 100s carloads 57 M iscellaneous 100 '* tons 62 Mixed Feed Brands and marks 79 Bulk carloads 56 Carloads, number of 43 " tons..