Are Today's Implantable Devices Better Than Conventional Solutions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NORE OG UVDAL KOMMUNE Næring, Miljø Og Kommunalteknikk
NORE OG UVDAL KOMMUNE Næring, miljø og kommunalteknikk LANDBRUKS- OG MATDEPARTEMENTET Postboks 8007 Dep 0030 OSLO Deres ref: Vår ref: Saksbeh: Arkivkode: Dato: 2017/1059 SLB - 31024613 V31 18.10.2017 Høringsuttalelse - Endringer i reglene om nydyrking - Forbud mot nydyrking av myr Vi viser til deres høringsbrev datert 11.7.2017. Hovedutvalg for næring, miljø og kommunalteknikk behandlet høringen i møte 12.10.2017 sak 74/17. Vedtak Hovedutvalg for næring, miljø og kommunalteknikk – 12.10.2017: «Generelt: Nore og Uvdal kommune stiller spørsmålstegn ved den strukturdrivende landbrukspolitikken som har blitt ført de siste årene, spesielt i forhold til at driftsbygninger bør ha tilstrekkelig arealgrunnlag. Det foreslåtte forbudet mot nydyrking av myr passer ikke inn i denne sammenhengen. Det påpekes også at den samfunnsøkonomiske besparelsen ved et slikt forbud bare er på kr 1 million for hele landet, og at dette er lite i forhold til den ulempen enkelte gårdbrukere får. Det meste av det dyrkbare arealet, inkludert dyrkbar myr, ligger i klimasoner som uansett ikke egner seg for kornproduksjon. Et forbud mot nydyrking av myr vil derfor i stor grad få negativ betydning for husdyrholdet og matproduksjonen i Norge. Dette momentet bør fremstilles bedre når Stortingsproposisjonen skal utarbeides. Jordlova: § 11 Drift av jordbruksareal, nydyrking og driftsvegar Ingen merknad. Nydyrkingsforskrifta: § 1 Formål Det vil være uheldig at § 3 fjerde ledd annet punktum om adkomst til bakenforliggende areal, ikke videreføres etter denne flyttingen. Dette er et viktig moment i vurderingen av søknader om godkjenning av plan for nydyrking, for å hindre at eksisterende ferdselsveier og større stier blir avskåret av innmark. -

Forskrift Om Skolerute for Viken Skoleåret 2021-2022
Forskrift om skolerute for Viken skoleåret 2021-2022 Forskrift gitt med hjemmel i opplæringslovens §3-2. Vedtatt av fylkestinget i Viken fylkeskommune dato 21.oktober 2020 Skoleruta for skoleåret 2021-2022 for skoler i Hurdal, Eidsvoll, Nes, Aurskog-Høland, Marker, Aremark, Halden, Hvaler, Sarpsborg, Rakkestad, Fredrikstad, Råde, Moss, Våler, Skiptvedt, Indre Østfold, Vestby, Ås, Frogn, Nesodden, Nordre Follo, Enebakk, Lørenskog, Rælingen, Lillestrøm, Nittedal, Gjerdrum, Ullensaker, Nannestad, Asker og Bærum Skoledager elever Ferier, fridager, kommentarer August 10 Første skoledag: uke 33, onsdag 18.08 September 22 Oktober 16 Høstferie: uke 40: f.o.m. mandag 04.10 t.o.m. fredag 08.10 November 21 Onsdag 17.11 Fri for elever, felles plandag for lærere Desember 15 Juleferie f.o.m. onsdag 22.12 Januar 21 Juleferie t.o.m. søndag 02.01 Februar 15 Vinterferie uke 8: f.o.m. mandag 21.02 t.o.m. fredag 25.02 Mars 23 April 15 Påskeferie f.o.m lørdag 09.04 t.o.m. mandag 18.04 Mai 20 Fri/helgedag: 17.05, 26.05 Juni 12 Fri 06.06 Siste skoledag: fredag 17.06 Sum 190 Offentlige fridager: Søndag 01.05 Tirsdag 17.05 Torsdag 26.05 Kr. Himmelfartsdag Mandag 06.06 2. pinsedag Oslo, 25.06.2020 Skoleruta for skoleåret 2021-2022 for skoler i Hemsedal, Gol, Ål, Nes i Hallingdal, Hol, Nore og Uvdal, Modum, Flå, Ringerike, Hole, Krødsherad, Sigdal, Rollag, Flesberg, Øvre Eiker, Kongsberg, Drammen, Lier, Jevnaker og Lunner Skoledager elever Ferier, fridager, kommentarer August 10 Første skoledag: uke 33, onsdag 18.08 September 22 Oktober 16 Høstferie: uke 40: f.o.m. -
Norway Maps.Pdf
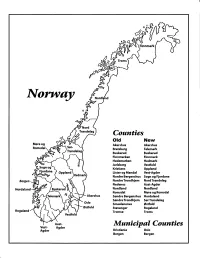
Finnmark lVorwny Trondelag Counties old New Akershus Akershus Bratsberg Telemark Buskerud Buskerud Finnmarken Finnmark Hedemarken Hedmark Jarlsberg Vestfold Kristians Oppland Oppland Lister og Mandal Vest-Agder Nordre Bergenshus Sogn og Fjordane NordreTrondhjem NordTrondelag Nedenes Aust-Agder Nordland Nordland Romsdal Mgre og Romsdal Akershus Sgndre Bergenshus Hordaland SsndreTrondhjem SorTrondelag Oslo Smaalenenes Ostfold Ostfold Stavanger Rogaland Rogaland Tromso Troms Vestfold Aust- Municipal Counties Vest- Agder Agder Kristiania Oslo Bergen Bergen A Feiring ((r Hurdal /\Langset /, \ Alc,ersltus Eidsvoll og Oslo Bjorke \ \\ r- -// Nannestad Heni ,Gi'erdrum Lilliestrom {", {udenes\ ,/\ Aurpkog )Y' ,\ I :' 'lv- '/t:ri \r*r/ t *) I ,I odfltisard l,t Enebakk Nordbv { Frog ) L-[--h il 6- As xrarctaa bak I { ':-\ I Vestby Hvitsten 'ca{a", 'l 4 ,- Holen :\saner Aust-Agder Valle 6rrl-1\ r--- Hylestad l- Austad 7/ Sandes - ,t'r ,'-' aa Gjovdal -.\. '\.-- ! Tovdal ,V-u-/ Vegarshei I *r""i'9^ _t Amli Risor -Ytre ,/ Ssndel Holt vtdestran \ -'ar^/Froland lveland ffi Bergen E- o;l'.t r 'aa*rrra- I t T ]***,,.\ I BYFJORDEN srl ffitt\ --- I 9r Mulen €'r A I t \ t Krohnengen Nordnest Fjellet \ XfC KORSKIRKEN t Nostet "r. I igvono i Leitet I Dokken DOMKIRKEN Dar;sird\ W \ - cyu8npris Lappen LAKSEVAG 'I Uran ,t' \ r-r -,4egry,*T-* \ ilJ]' *.,, Legdene ,rrf\t llruoAs \ o Kirstianborg ,'t? FYLLINGSDALEN {lil};h;h';ltft t)\l/ I t ,a o ff ui Mannasverkl , I t I t /_l-, Fjosanger I ,r-tJ 1r,7" N.fl.nd I r\a ,, , i, I, ,- Buslr,rrud I I N-(f i t\torbo \) l,/ Nes l-t' I J Viker -- l^ -- ---{a - tc')rt"- i Vtre Adal -o-r Uvdal ) Hgnefoss Y':TTS Tryistr-and Sigdal Veggli oJ Rollag ,y Lvnqdal J .--l/Tranbv *\, Frogn6r.tr Flesberg ; \. -

“Hole” in One for Nesbø
(Periodicals postage paid in Seattle, WA) TIME-DATED MATERIAL — DO NOT DELAY Travel Heritage Update No. 1 from A day to Hvis du tror du kan gjøre det, så celebrate all the St. Olaf Choir! kan du. – John Burroughs fathers Read more on page 9 Read more on page 14 Norwegian American Weekly Vol. 124 No. 23 June 14, 2013 Established May 17, 1889 • Formerly Western Viking and Nordisk Tidende $1.50 per copy News in brief Find more at blog.norway.com “Hole” in one for Nesbø News Cash worth NOK 17.2 million has Jo Nesbø’s tenth been confiscated by Norwegian Harry Hole thriller Customs so far this year, an increase of nearly 20 percent in was released one year. Customs fear that the in Norway on problem will increase with the Euro crisis. Of the confiscated June 6 to great money, NOK 9.2 million has been discovered among passengers excitement at the Oslo Airport Gardermoen during the first five months of this year. However, Customs estimate that NOK 2 – 3 billion STAFF COMPILATION is smuggled out of Norway Norwegian American Weekly each year. Large amounts are whitewashed and brought back. They believe the money may On June 6, the long awaited be linked to illegal import of tenth installment in the Harry Hole drugs, human trafficking and series, “Politi” (which means sim- prostitution. ply “Police”) was released in Nor- (Norway Post) way. Aschehoug, Jo Nesbø’s Nor- Business wegian publisher, arranged a big Statoil is drilling well number release-party with nearly a thou- 100 in the Barents Sea. -

Age-Friendly Tourism in Europe Jan Edøy Brussels,19
Setting the context of age-friendly tourism in Europe Jan Edøy Brussels,19. October 2017 Regions in Europe Members of the Oslo Region European Office • 8 counties: Akershus, Buskerud, Hedmark, Oppland, Oslo, Telemark, Vestfold and Östfold • 11 municipalities and 2 Universities • 30%of the territory of Norway • 50% of the population 2.5 million inhabitants, Tourism is a major contributor to OECD economies The direct contribution of tourism to OECD countries As percentage of GDP and employment Source: OECD The EU tourism industry EU tourism policy • EU treaties exclude any harmonisation of tourism laws and allow the EU only to support, coordinate or supplement the actions of the Member States. • EU tourism policy is rather limited, consisting mainly of providing financial support or legislating through other EU policies. Tourism in the treaties • The European Union mentioned tourism in the treaties for the first time in 1992. • In 2007, the EU created a specific section for tourism in the Treaty on TFEU in Article 195 - stating that EU action 'shall be aimed at: • a) encouraging the creation of a favourable environment for the development of undertakings in this sector; • b) promoting cooperation between the Member States, particularly by the exchange of good practice.' EU tourism strategy The strategy paper identified four priority areas for action: • simulate competitiveness in the European tourism sector; • promote the development of sustainable, responsible and high-quality tourism; • consolidate the image and profile of Europe as a -

Skiløyper Opheim-, Torpo- Og Skaraåsen 2016
Skiløyper Opheim-, Torpo- og Skaraåsen 2016 Løypekart og info frå Torpo Skiløypelag www.skisporet.no/buskerud/opheimtorpo Opplev en hyggelig skidag i solsiden av Hallingdal • Gol Skipark har 12 nedfarter • Løypelengder opp til 3500 meter • Høydeforskjell på 470 meter • Ny og flott Jibbepark • Egen barnebakke • 3 heiser • Skiutleie • Events Fra alpinanlegget er det også tilgang til løypenettet på Skaraåsen og Torpoåsen. Velkommen til en hyggelig skidag. www.golskipark.no 2 Torpo Skiløypelag 2016 Løypelaget arbeider heile tida for å utvikle og hogge og halde trasèane i orden om sommaren og vedlikehalde løypenettet på Torpo/Opheimsåsen dette høyrer også under løypelaget sine gjeremål og Skaraåsen på Golsida. Dette gjeld då og budsjett. Det er krattknust ein del løyper sist løypenettet frå Helsingset, Reinshovdstølen, haust, og i fleire traséar er det fjerna steinar og Nystølane, Opheimstølane, Grytingen i vest til planert med gravemaskin. Sjauset, Narveset, Smylistølane, Habbeset, Feten GPS-oppdatering av løypenettet og til toppen av Gol Skisenter/Skaran i aust. GPS-sendar i alle løypemaskinene i Ål, Hol, Gol, Vilkåra for kommunalt tilskot til løypekøyring i Nes og Hemsedal gjer at du kan gå inn på Ål og Gol er at løypene skal vera oppkøyrte til internett og sjå kva for løyper som er nyoppkjørte. visse tider. Dei minst værharde løypene skal vera Alle desse områda finn du på www.skisporet.no, oppkøyrte (ved behov) kvar laurdag og sundag www.al.no, eller www.hyttavaar.no Dersom de er frå veke 50 til veke 16 og kvar dag i vinterferie og ute i løypene når trøkkemaskinen kjem, gå godt påske når snøforholda tillet det. -

Lions Clubs International Club Membership Register Summary the Clubs and Membership Figures Reflect Changes As of September 2004
LIONS CLUBS INTERNATIONAL CLUB MEMBERSHIP REGISTER SUMMARY THE CLUBS AND MEMBERSHIP FIGURES REFLECT CHANGES AS OF SEPTEMBER 2004 CLUB CLUB LAST MMR FCL YR MEMBERSHI P CHANGES TOTAL DIST IDENT NBR CLUB NAME STATUS RPT DATE OB NEW RENST TRANS DROPS NETCG MEMBERS 3929 019603 AL 104 G 4 09-2004 32 0 0 0 0 0 32 3929 019607 DRAMMEN 104 G 4 08-2004 17 0 0 0 0 0 17 3929 019608 DRAMMEN VEST 104 G 4 07-2004 29 0 0 0 -1 -1 28 3929 019611 FLA 104 G 4 16 0 0 0 0 0 16 3929 019613 KRODSHERAD 104 G 4 09-2004 20 0 0 0 -1 -1 19 3929 019614 GOL 104 G 4 09-2004 23 1 0 0 0 1 24 3929 019616 HONEFOSS 104 G 4 27 0 0 0 0 0 27 3929 019617 HOL 104 G 4 09-2004 30 0 0 0 -1 -1 29 3929 019618 HURUM 104 G 4 08-2004 18 0 0 0 0 0 18 3929 019619 KONGSBERG 104 G 4 09-2004 36 1 0 0 -1 0 36 3929 019624 LIER 104 G 4 08-2004 27 0 0 0 -1 -1 26 3929 019625 LIER OST 104 G 4 24 0 0 0 0 0 24 3929 019629 MODUM 104 G 4 07-2004 28 0 0 0 -1 -1 27 3929 019631 NEDRE EIKER L C 104 G 4 04-2004 34 0 0 0 0 0 34 3929 019634 OVRE EIKER L C 104 G 4 09-2004 37 3 0 0 0 3 40 3929 019639 ROYKEN 104 G 4 09-2004 21 1 0 0 0 1 22 3929 019640 SIGDAL 104 G 4 09-2004 37 0 0 0 0 0 37 3929 019646 TYRISTRAND 104 G 4 09-2004 28 0 0 0 0 0 28 3929 019649 ASKER 104 G 4 09-2004 31 0 0 0 -1 -1 30 3929 019650 BORGEN 104 G 4 09-2004 11 0 0 0 0 0 11 3929 019652 BLAKSTAD 104 G 4 09-2004 22 0 0 0 -2 -2 20 3929 019663 NESBRU 104 G 4 08-2004 26 0 0 0 0 0 26 3929 019664 NESOYA 104 G 4 17 0 0 0 0 0 17 3929 019707 HOLMESTRAND 104 G 4 09-2004 30 0 0 0 -1 -1 29 3929 019709 HORTEN 104 G 4 09-2004 26 0 0 0 -2 -2 24 3929 029133 -

Arkiv › Trogstad-Menighetsblad-2006
FOR TRØGSTAD OG BÅSTAD Årgang 45 nr. 4 September 2006 Et glimt fra Afrika Vi var der! den gode viljen: side 3 NRK's TV aksjon den 22.oktober 2006 Krigens virkelighet En svensk 16-åring dro til Israel... side 2 Ny medarbeider i kirken vår... I dette intervjuet forteller hun både om "sitt oppdrag" og om seg selv... side 6 Profilen: Elisabeth Tveten Navnet skjemmer ingen: Elisabeth er både kongelig og bibelsk. side 9 Konfirmanter i Trøgstad og Båstad: Sammen igjen etter 50 år! Se bildene... side 11 Søndagen den 22. oktober viser vi igjen den Gode Vilje mot våre medmennesker på denne kloden. Det er stort, både for de som reddes og oss priviligerte som jo får en anledning til å gi. se mer på side 13 >>> Side 1 Fra redaktørens penn... Trøgstad prestegjeld Krigens virkelighet Kirkekontor: En svensk 16-åring dro til Israel for 35 år siden fordi hans Kommunehuset, Kirkeveien 17 lærerinne hadde fortalt så mange bibelhistorier fra dette landet. 1860 Trøgstad Han ble der. E-post: [email protected] Etter noen år ble han israelsk statsborger, giftet seg med ei Menighetsbladet på internett: israelsk kvinne og fikk tre barn. I dag bor familien i en kibbutz, han www.trokirk.no er registrert israelsk guide og er samtidig knyttet til det israelske De ansatte har også egne mail-adresser: forsvaret. [email protected] Under et besøk til landet sist vinter ble jeg kjent med Stefan. Nylig Ang. dåp, bryllup, vigsel; ring helst tirsdag kom det en E-post til en av reisedeltagerne fra Norge der jeg og torsdag klokka 9-11. -

Generelle Bestemmelser Og Retningslinjer Med Vedlegg
Plan-ID 201701 Kommuneplanens arealdel 2018 - 2030 Vedtatt i Askim bystyre 3. mai 2018, sak 27/18. GENERELLE BESTEMMELSER OG RETNINGSLINJER MED VEDLEGG Vedlegg 1: Oversikt over gjeldende reguleringsplaner i Askim kommune pr. 3.5.2018 Vedlegg 2: Beskrivelse av hensynssoner i plankartet. Bestemmelser og plankart er juridisk bindende. Retningslinjene (i kursiv) er kun av veiledende karakter og kan ikke brukes som hjemmelsgrunnlag for vedtak etter planen. §1. HENSIKTEN MED PLANEN Kommuneplanens areadel skal sikre en arealbruk fram til 2030 som bidrar til at Askim kommune oppnår de langsiktige målene for samfunnsutviklingen fastsatt i kommuneplanens samfunnsdel. I alle arealplaner og ved gjennomføring av tiltak skal det tas særlig hensyn til klima, folkehelse, barn og unge og Askims rolle som regionalt byområde. §2. EKSISTERENDE REGULERINGSPLANER Vedtatte/stadfestede reguleringsplaner gjelder fortsatt, jf. vedlegg «Oversikt over gjeldende reguleringsplaner i Askim kommune pr. 3.5.2018». Gammel plan gjelder så langt det ikke er motstrid til kommuneplanen. Nyere reguleringsplaner gjelder foran gamle reguleringsplaner. §3. KLIMA 1. Planleggingen skal bidra til å redusere innbyggernes og næringsvirksomhetenes klimagassutslipp (det skal legges til rette for bruk av fornybar energi ved planlegging og utbygging i nye byggeområder). 2. Planleggingen skal forholde seg til at Norge har forpliktet seg til minst 40 prosent utslippsreduksjon i 2030 sammenliknet med 1990. (Meld. St. 13, 2014-2015: Ny utslippsforpliktelse for 2030 – en felles løsning med EU) 3. Lokal håndtering av overvann skal være et gjennomgående prinsipp i arealplaner og ved gjennomføring av tiltak. §4. FOLKEHELSE I alle arealplaner og ved gjennomføring av tiltak skal det legges til rette for et helsefremmende samfunn bygget på prinsippene sosial utjevning, helse i alt vi gjør, bærekraftig utvikling, føre var og medvirkning. -

Suksesjon Av Ferskvannsinvertebrater I Et Nyetablert Damsystem I Trøgstad Kommune
74 NINA Fagrapport Suksesjon av ferskvannsinvertebrater i et nyetablert damsystem i Trøgstad kommune Asbjørn Magnar Hov Bjørn Walseng L AGSPILL E NTUSIASME I NTEGRITET K VALITET Samarbeid og kunnskap for framtidas miljøløsninger NINA Norsk institutt for naturforskning Suksesjon av ferskvannsinvertebrater i et nyetablert damsystem i Trøgstad kommune Asbjørn Magnar Hov Bjørn Walseng nina Fagrapport 074 NINAs publikasjoner Hov, A.M. & Walseng, B. 2003. Suksesjon av ferskvannsinverte- brater i et nyetablert damsystem i Trøgstad kommune. NINA utgir følgende faste publikasjoner: NINA Fagrapport 074. 50pp. NINA Fagrapport Oslo, desember 2003 Her publiseres resultater av NINAs eget forskningsarbeid, ISSN 0805-469x problemoversikter, kartlegging av kunnskapsnivået innen et ISBN 82-426-1424-5 emne, og litteraturstudier. Rapporter utgis også som et alterna- tiv eller et supplement til internasjonal publisering, der tids- Klassifisering av publikasjonen: aspekt, materialets art, målgruppe m.m. gjør dette nødvendig. Forurensning og miljøovervåking i limnisk miljø - Invertebrater Opplag: Normalt 300-500 Pollution and monitoring of fresh water ecosystems - Invertebrates NINA Oppdragsmelding Rettighetshaver: Dette er det minimum av rapportering som NINA gir til oppdrags- Norsk institutt for naturforskning (NINA) giver etter fullført forsknings- eller utredningsprosjekt. I tillegg til de emner som dekkes av fagrapportene, vil oppdragsmeldingene Publikasjonen kan siteres fritt med kildeangivelse også omfatte befaringsrapporter, seminar- og konferanse- foredrag, årsrapporter fra overvåkningsprogrammer, o.a. Opplaget er begrenset. (Normalt 50-100) NINA Project-Report Serien presenter resultater fra instituttets prosjekter når resultatene må gjøres tilgjengelige på engelsk. Serien omfatter original egenforskning, litteraturstudier, analyser av spesielle problem eller tema, etc. Opplaget varierer avhengig av behov og målgruppe. Temahefter Disse behandler spesielle tema og utarbeides etter behov bl.a. -

Og Vesentlighetsvurdering. Nore Og Uvdal Kommune
ROV September 2020 Risiko - og vesentlighetsanalyse En overordnet analyse av Nore og Uvdal kommune Viken kommunerevisjon Nore og Uvdal kommune | 2020 | Risiko- og vesentlighetsanalyse Innhold 1. Innledning ........................................................................................... 4 1.1. Bestilling ....................................................................................................... 4 1.2. Formål ......................................................................................................... 4 1.3. Sentrale bestemmelser ..................................................................................... 4 1.3.1. Forvaltningsrevisjon ........................................................................................... 4 1.3.2. Eierskapskontroll ............................................................................................... 5 1.4. Kommunens ansvar og roller .............................................................................. 6 1.5. Koronapandemien ........................................................................................... 7 2. Metode - leseveiledning ........................................................................... 8 2.1. Teorigrunnlag ................................................................................................. 8 2.2. Risiko ........................................................................................................... 9 2.3. Vesentlighet ................................................................................................ -

Nore Og Uvdal Kommune
Nore og Uvdal kommune Rødberg : 18.04.2017 Arkiv : L12 Saksmappe : 2015/1021 Avd. : Næring, miljø og kommunalteknikk Saksbehandler : Målfrid Toeneiet Sluttbehandling av reguleringsplan ID 2015012 Brøstrud /Sønstebø hytteområde MØTEBEHANDLING: Utvalg Møtedato Utvalgssak Hovedutvalg næring, miljø og kommunalteknikk 11.05.2017 35/17 Saken gjelder: Sluttbehandling av reguleringsplan ID 2015012 Brøstrud/Sønstebø hytteområde, del av sameiet gnr 11 bnr 11, på Dagalifjell. En godkjenning av ny reguleringsplan ID 2015012 Brøstrud/Sønstebø hytteområde innebærer at gjeldende reguleringsplan Brøstrud/Sønstebø sameie (ID 1973806) oppheves, og reguleringsplan Brøstrud/Sønstebø sameie (ID 1996817) blir delvis erstattet. Fakta: Forslag til reguleringsplan ID 2015012 Brøstrud/Sønstebø hytteområde ble vedtatt lagt ut til offentlig ettersyn ved delegert vedtak 172/17 datert 21.02.17. Planforslaget er utarbeidet av Sivilarkitekt Øystein Landsgård og Vidda Ressurs AS på vegne av grunneierne Vilhelm Håvardsrud og Arne Gunnar Haugen. Området strekker seg fra Ånevatn til Hagasetåsen 998-1075 meter over havet. Området ligger i fjellbjørkeskog. Planområdet omfattes av følgende reguleringsplaner: Brøstrud/Sønstebø sameie (ID 1996817) og Brøstrud/Sønstebø sameie (ID 1973806). Vedtak av ny reguleringsplan Brøstrud/Sønstebø hytteområde vil oppheve reguleringsplan Brøstrud/Sønstebø sameie (ID 1973806), og delvis erstatte Brøstrud/Sønstebø sameie (ID 1996817). Planområdet er avsatt til byggeområde for fritidsbebyggelse i kommunedelplan for Dagalifjell med Rødberg vedtatt 13.02.17. Planforslaget er i tråd med kommunedelplanen og omfattes således ikke av forskrift om konsekvensutredninger. Planområdet omfattes ikke av regional plan for Hardangervidda. Gjeldene reguleringsplan består av 28 tomter hvorav 2 ubebygde tomter. Det planlegges 29 nye tomter. Det ligger to seterområder innenfor planen. Ordinære tomter kan bebygges med inntil to bygninger med totalt 170 m2 BYA.