96 Pp Naca Book for Web 2003
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2017 SEAT Report Jwaneng Mine
JWANENG MINE SEAT 3REPORT 2017 - 2020 Contents INTRODUCTION TO JWANENG MINE’S SEAT 14 EXISTING SOCIAL PERFORMANCE 40 1. PROCESS 4. MANAGEMENT ACTIVITIES 1.1. Background and Objectives 14 4.1. Debswana’s Approach to Social Performance 41 and Corporate Social Investment 1.2. Approach 15 4.1.1. Approach to Social Performance 41 1.3. Stakeholders Consulted During SEAT 2017 16 4.1.2. Approach to CSI Programmes 41 1.4. Structure of the SEAT Report 19 4.2. Mechanisms to Manage Social Performance 41 2. PROFILE OF JWANENG MINE 20 4.3. Ongoing Stakeholder Engagement towards 46 C2.1. Overview of Debswana’s Operational Context 20 Social Performance Management 2.2. Overview of Jwaneng Mine 22 DELIVERING SOCIO-ECONOMIC BENEFIT 49 2.2.1. Human Resources 23 5. THROUGH ALL MINING ACTIVITIES 2.2.2. Procurement 23 5.1. Overview 50 2.2.3. Safety and Security 24 5.2. Assessment of Four CSI/SED Projects 52 2.2.4. Health 24 5.2.1. The Partnership Between Jwaneng Mine 53 Hospital and Local Government 2.2.5. Education 24 5.2.2. Diamond Dream Academic Awards 54 2.2.6. Environment 25 5.2.3. Lefhoko Diamond Village Housing 55 2.3. Future Capital Investments and Expansion 25 Plans 5.2.4. The Provision of Water to Jwaneng Township 55 and Sese Village 2.3.1. Cut-8 Project 25 5.3. Assessing Jwaneng Mine’s SED and CSI 56 2.3.2. Cut-9 Project 25 Activities 2.3.3. The Jwaneng Resource Extension Project 25 SOCIAL AND ECONOMIC IMPACTS 58 (JREP) 6. -
List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O
Primary School Leaving Examination 2010 List of Examination Centres by Region Bobirwa Region Centr Name Addres Place Phone 0101 Bobonong Primary School P.O. Box 48 BOBONONG 2619207 0103 Borotsi Primary School P.O. Box 136 BOBONONG 819208 0107 Gobojango Primary School Private Bag 8 BOBONONG 2645436 0108 Lentswe-Le-Moriti Primary School Private Bag 0019 BOBONONG 0110 Mabolwe Primary School P.O. Box 182 SEMOLALE 2645422 0111 Madikwe Primary School P.O. Box 131 BOBONONG 2619221 0112 Mafetsakgang primary school P.O. Box 46 BOBONONG 2619232 0114 Mathathane Primary School P.O. Box 4 MATHATHANE 2645110 0117 Mogapi Primary School P.O. Box 6 MOGAPI 2618545 0119 Molalatau Primary School P.O. Box 50 MOLALATAU 845374 0120 Moletemane Primary School P.O. Box 176 TSETSEBYE 2646035 0123 Sefhophe Primary School P.O. Box 41 SEFHOPHE 2618210 0124 Semolale Primary School P.O. Box 10 SEMOLALE 2645422 0131 Tsetsejwe Primary School P.O. Box 33 TSETSEJWE 2646103 0133 Modisaotsile Primary School P.O. Box 591 BOBONONG 2619123 0134 Motlhabaneng Primary School Private Bag 20 BOBONONG 2645541 0135 Busang Primary School P.O. Box 47 TSETSEBJE 2646144 0138 Rasetimela Primary School Private Bag 0014 BOBONONG 2619485 0139 Mabumahibidu Primary School P.O. Box 168 BOBONONG 2619040 0140 Lepokole Primary School P O Box 148 BOBONONG 4900035 0141 Agosi Primary School P O Box 1673 BOBONONG 71868614 0142 Motsholapheko Primary School P O Box 37 SEFHOPHE 2618305 0143 Mathathane DOSET P.O. Box 4 MATHATHANE 2645110 0144 Tsetsebye DOSET P.O. Box 33 TSETSEBYE 3024 Bobonong DOSET P.O. Box 483 BOBONONG 2619164 Saturday, September 25, List of Examination Centres by Region Page 1 of 39 Boteti Region Centr Name Addres Place Phone 0201 Adult Education Private Bag 1 ORAPA 0202 Baipidi Primary School P.O. -

Refundable Fee of P280.00 (Two Hundred and Eighty Pula Only) VAT Inclusive
PUBLIC TENDER NOTICE TENDER NO: BOCRA/PT/006/2020.2021 SUPPLY, INSTALLATION AND COMMISSIONING OF ICT EQUIPMENT AT TWELVE (12) TRIBAL ADMINISTRATIONS IN KWENENG DISTRICT The Botswana Communications Regulatory Authority (BOCRA or the Authority) hereby invites experienced and reputable companies to tender for the Supply, Installation and Commissioning of ICT Equipment at twelve (12) Tribal Administrations in Kweneng District. The tender is reserved for 100% citizen-owned companies who are registered with the Public Procurement and Asset Disposal Board (PPADB) under the following codes and subcodes; Code 203: Electrical, Electronic, Mechanical and ICT Supplies Subcode 01: Electrical and Electronic Equipment, Spares and Accessories (includes ICT, photographic equipment, and others). Youth owned companies in Botswana shall purchase the ITT at 50% of the purchase price as per Presidential Directive CAB 14 (B)/2015. The Invitation to Tender (ITT) document may be purchased at the BOCRA Head Office by interested companies at a non-refundable fee of P280.00 (Two Hundred and Eighty Pula Only) VAT inclusive. Payment must be made in the form of bank transfer or deposits to the following bank details: Bank Name: First National Bank Botswana Ltd Branch Name: Mall Branch Code: 28-28-67 Account Name: Botswana Communications Regulatory Authority Bank Account No: 62011115088 Swift Code: FIRNBWGX Reference: BTA0001 Tender documents shall be issued upon provision of Proof of Payment (POP). All funds transfer bank charges shall be borne by the bidder. Compulsory -

Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization
Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization. Item Type text; Electronic Dissertation Authors Ijagbemi, Bayo, 1963- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 17:13:55 Link to Item http://hdl.handle.net/10150/196133 LAND TENURE REFORMS AND SOCIAL TRANSFORMATION IN BOTSWANA: IMPLICATIONS FOR URBANIZATION by Bayo Ijagbemi ____________________ Copyright © Bayo Ijagbemi 2006 A Dissertation Submitted to the Faculty of the DEPARTMENT OF ANTHROPOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2006 2 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Bayo Ijagbemi entitled “Land Reforms and Social Transformation in Botswana: Implications for Urbanization” and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy _______________________________________________________________________ Date: 10 November 2006 Dr Thomas Park _______________________________________________________________________ Date: 10 November 2006 Dr Stephen Lansing _______________________________________________________________________ Date: 10 November 2006 Dr David Killick _______________________________________________________________________ Date: 10 November 2006 Dr Mamadou Baro Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. -

Botswana Semiology Research Centre Project Seismic Stations In
BOTSWANA SEISMOLOGICAL NETWORK ( BSN) STATIONS 19°0'0"E 20°0'0"E 21°0'0"E 22°0'0"E 23°0'0"E 24°0'0"E 25°0'0"E 26°0'0"E 27°0'0"E 28°0'0"E 29°0'0"E 30°0'0"E 1 S 7 " ° 0 0 ' ' 0 0 ° " 7 S 1 KSANE Kasane ! !Kazungula Kasane Forest ReserveLeshomo 1 S Ngoma Bridge ! 8 " ! ° 0 0 ' # !Mabele * . MasuzweSatau ! ! ' 0 ! ! Litaba 0 ° Liamb!ezi Xamshiko Musukub!ili Ivuvwe " 8 ! ! ! !Seriba Kasane Forest Reserve Extension S 1 !Shishikola Siabisso ! ! Ka!taba Safari Camp ! Kachikau ! ! ! ! ! ! Chobe Forest Reserve ! !! ! Karee ! ! ! ! ! Safari Camp Dibejam!a ! ! !! ! ! ! ! X!!AUD! M Kazuma Forest Reserve ! ShongoshongoDugamchaRwelyeHau!xa Marunga Xhauga Safari Camp ! !SLIND Chobe National Park ! Kudixama Diniva Xumoxu Xanekwa Savute ! Mah!orameno! ! ! ! Safari Camp ! Maikaelelo Foreset Reserve Do!betsha ! ! Dibebe Tjiponga Ncamaser!e Hamandozi ! Quecha ! Duma BTLPN ! #Kwiima XanekobaSepupa Khw!a CHOBE DISTRICT *! !! ! Manga !! Mampi ! ! ! Kangara # ! * Gunitsuga!Njova Wazemi ! ! G!unitsuga ! Wazemi !Seronga! !Kaborothoa ! 1 S Sibuyu Forest Reserve 9 " Njou # ° 0 * ! 0 ' !Nxaunxau Esha 12 ' 0 Zara ! ! 0 ° ! ! ! " 9 ! S 1 ! Mababe Quru!be ! ! Esha 1GMARE Xorotsaa ! Gumare ! ! Thale CheracherahaQNGWA ! ! GcangwaKaruwe Danega ! ! Gqose ! DobeQabi *# ! ! ! ! Bate !Mahito Qubi !Mahopa ! Nokaneng # ! Mochabana Shukumukwa * ! ! Nxabe NGAMILAND DISTRICT Sorob!e ! XurueeHabu Sakapane Nxai National Nark !! ! Sepako Caecae 2 ! ! S 0 " Konde Ncwima ° 0 ! MAUN 0 ' ! ! ' 0 Ntabi Tshokatshaa ! 0 ° ! " 0 PHDHD Maposa Mmanxotai S Kaore ! ! Maitengwe 2 ! Tsau Segoro -

2019 GENERAL ELECTIONS REPORT II Keireng A
REPORT TO THE MINISTER FOR PRESIDENTIAL AFFAIRS, GOVERNANCE AND PUBLIC ADMINISTRATION ON THE 2019 GENERAL ELECTIONS 2019 GENERAL ELECTIONS I REPORT Honourable Justice Abednego B. Tafa Mr. John Carr-Hartley Members of CHAIRMAN DEPUTY CHAIRMAN The Independent Electoral Commission Mrs. Agnes Setlhogile Mrs. Shaboyo Motsamai Dr. Molefe Phirinyane COMMISSIONER COMMISSIONER COMMISSIONER Mrs. Martha J. Sayed Vacant COMMISSIONER COMMISSIONER 2019 GENERAL ELECTIONS REPORT II Keireng A. Zuze Doreen L. Serumula SECRETARY DEPUTY SECRETARY Executive Management of the Secretariat Keolebogile M. Tshitlho Dintle S. Rapoo SENIOR MANAGER MANAGER CORPORATE SERVICES ELECTIONS AFFAIRS & FIELD OPERATIONS Obakeng B. Tlhaodi Uwoga H. Mandiwana CHIEF STATE COUNSEL MANAGER HUMAN RESOURCE & ADMINISTRATION 2019 GENERAL ELECTIONS REPORT III Strategic Foundations ........................................................................................................................... I Members of The Independent Electoral Commission ................................................ II Executive Management of the Secretariat........................................................................... III Letter to The Minister for Presidential Affairs, Governance and Public Administration ............................................................................................................... 1 ACKNOWLEDGEMENTS.................................................................................................................. 2 ACRONYMS ............................................................................................................................................... -
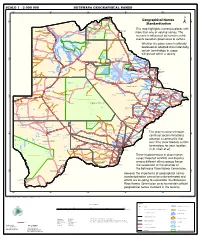
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

Establishment of Subordinate Land Boards (Amendment) Order
CHAPTER 32:02 - TRIBAL LAND: SUBSIDIARY LEGISLATION INDEX TO SUBSIDIARY LEGISLATION Establishment of Subordinate Land Boards (Amendment) Order Establishment of Subordinate Land Boards Order Tribal Land (Establishment of Land Tribunals) Order Tribal Land (Subordinate Land Boards) Regulations Tribal Land Regulations ESTABLISHMENT OF SUBORDINATE LAND BOARDS ORDER (under section 19) (15th June, 1973) ARRANGEMENT OF PARAGRAPHS PARAGRAPH 1. Citation 2. Establishment 3. Area of jurisdiction 4. Functions Schedule S.I. 47, 1973, S.I. 3, 1979, S.I. 125, 1979, S.I. 132, 1980, S.I. 78, 1981, S.I. 81, 1981, S.I. 110, 1981, S.I. 68, 1982, S.I. 5, 1984, S.I. 92, 1984, S.I. 36, 1986, S.I. 55,1987, S.I. 97, 1989, S.I. 45, 1992, S.I. 66, 1994, S.I. 53, 2002. 1. Citation Copyright Government of Botswana This Order may be cited as the Establishment of Subordinate Land Boards Order. 2. Establishment The subordinate land boards referred to in the second column of the Schedule hereto are established as the subordinate land boards within the district named in the first column of the said Schedule. 3. Area of jurisdiction The area of jurisdiction in respect of which each subordinate Land Board will perform its functions shall be the area or villages stated in relation to each subordinate land board in the third column of the Schedule. 4. Functions (1) The functions under customary law which vest in the subordinate land authority which are transferred to the subordinate land board shall include the hearing, grant or refusal of applications to use land for— ( a) building residences or extensions thereto; ( b) ploughing to a maximum extent of land determined by the tribal land board; ( c) grazing cattle or other stock; ( d) communal uses in the village. -

SABONET Report No 18
ii Quick Guide This book is divided into two sections: the first part provides descriptions of some common trees and shrubs of Botswana, and the second is the complete checklist. The scientific names of the families, genera, and species are arranged alphabetically. Vernacular names are also arranged alphabetically, starting with Setswana and followed by English. Setswana names are separated by a semi-colon from English names. A glossary at the end of the book defines botanical terms used in the text. Species that are listed in the Red Data List for Botswana are indicated by an ® preceding the name. The letters N, SW, and SE indicate the distribution of the species within Botswana according to the Flora zambesiaca geographical regions. Flora zambesiaca regions used in the checklist. Administrative District FZ geographical region Central District SE & N Chobe District N Ghanzi District SW Kgalagadi District SW Kgatleng District SE Kweneng District SW & SE Ngamiland District N North East District N South East District SE Southern District SW & SE N CHOBE DISTRICT NGAMILAND DISTRICT ZIMBABWE NAMIBIA NORTH EAST DISTRICT CENTRAL DISTRICT GHANZI DISTRICT KWENENG DISTRICT KGATLENG KGALAGADI DISTRICT DISTRICT SOUTHERN SOUTH EAST DISTRICT DISTRICT SOUTH AFRICA 0 Kilometres 400 i ii Trees of Botswana: names and distribution Moffat P. Setshogo & Fanie Venter iii Recommended citation format SETSHOGO, M.P. & VENTER, F. 2003. Trees of Botswana: names and distribution. Southern African Botanical Diversity Network Report No. 18. Pretoria. Produced by University of Botswana Herbarium Private Bag UB00704 Gaborone Tel: (267) 355 2602 Fax: (267) 318 5097 E-mail: [email protected] Published by Southern African Botanical Diversity Network (SABONET), c/o National Botanical Institute, Private Bag X101, 0001 Pretoria and University of Botswana Herbarium, Private Bag UB00704, Gaborone. -

List of Cities in Botswana
List of cities in Botswana The following is a list of cities and towns in Botswana with population of over 3,000 citizens. State capitals are shown in boldface. Population Female Rank Name District Census District [1] Male Population 2001. Population 1. Gaborone South-East District Gaborone 186,007 91,823 94,184 2. Francistown North-East District Francistown 83,023 40,134 42,889 3. Molepolole Kweneng District Kweneng East 62,739 28,617 34,122 4. Serowe Central District Central Serowe/Palapye 52,831 25,400 27,431 5. Selibe Phikwe Central District Selibe Phikwe 49,849 24,334 25,515 6. Maun North-West District Ngamiland East 49,822 23,714 26,108 7. Kanye Southern District Ngwaketse 48,143 22,451 25,692 8. Mahalapye Central District Central Mahalapye 43,538 21,120 22,418 9. Mogoditshane Kweneng District Kweneng East 40,753 20,972 19,781 10. Mochudi Kgatleng District Kgatleng 39,349 18,490 20,859 11. Lobatse South-East District Lobatse 29,689 14,202 15,487 12. Palapye Central District Central Serowe/Palapye 29,565 13,995 15,570 13. Ramotswa South-East District South East 25,738 12,027 13,711 14. Moshupa Southern District Ngwaketse 22,811 10,677 12,134 15. Tlokweng South-East District South East 22,038 10,568 11,470 16. Bobonong Central District Central Bobonong 21,020 9,877 11,143 17. Thamaga Kweneng District Kweneng East 20,527 9,332 11,195 18. Letlhakane Central District Central Boteti 19,539 9,848 9,691 19. -

University of Botswana Faculty of Health Science Department of Nursing Challenges Faced by Hiv-Infected Adolescents in Rural Ar
UNIVERSITY OF BOTSWANA FACULTY OF HEALTH SCIENCE DEPARTMENT OF NURSING CHALLENGES FACED BY HIV-INFECTED ADOLESCENTS IN RURAL AREAS OF BOTSWANA NAME: MATLHODI GOSA BASUHI ID NO.200106336 PROPOSAL IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR MASTE COMMUNITY HEALTH NURSING SUPERVISOR: DR T.R. MONAU TABLE OF CONTENTS Acknowledgement --------------------------------------------------------------------------------------1 Operational Definitions --------------------------------------------------------------------------------2 Abstract ---------------------------------------------------------------------------------------------------4 List of Abbreviations -----------------------------------------------------------------------------------6 CHAPTER 1: INTRODUCTION AND PROBLEM STATEMENT-----------------------------7 1.1 Introduction ------------------------------------------------------------------------------------------7 1.2 General Background --------------------------------------------------------------------------------7 1.3 Statement of the problem---------------------------------------------------------------------------9 1.4 Justification -----------------------------------------------------------------------------------------13 1.5 Aim and Objectives of the study-----------------------------------------------------------------14 1.6 Conceptual Definitions----------------------------------------------------------------------------15 1.8 Summary---------------------------------------------------------------------------------------------16 -

Download File
Annual Report 2019 GROWING A CONNECTED AND DIGITALLY DRIVEN SOCIETY CONTENTS 1 About this Report INTRODUCTION 01 6 Chairman’s Statement 8 Board of Directors 10 Chief Executive’s Statement 14 Management 16 Executive Management GOVERNANCE 02 20 Role of the Board 22 Board Participation 23 Internal Audit 24 National Broadband Strategy 25 Project Management 26 UASF Strategy REVIEWS 03 30 Market Performance Review 64 Customer Protection 67 Stakeholder Engagement 72 Corporate Social Investment 73 Human Capital Management 75 Organisational Capital FINANCIAL STATEMENTS 04 80 General Information 81 Board Members’ Report 82 Board Members’ Responsibilities and Approval 83 Independent Auditor's Report 88 Consolidated and Separate Statements of Financial Position 89 Consolidated and Separate Statements of Comprehensive Income 90 Consolidated and Separate Statements of Cash Flows 91 Consolidated and Separate Statements of Changes in Equity 93 Accounting Policies 107 Notes to the Annual Financial Statements The following supplementary information does not form part of the Annual Financial Statements and is unaudited: 128 Detailed Income Statement REPORT APPROACH To truly demonstrate how BOCRA has performed in the period under review, we know we need to assess ourselves across a number of key spheres; these being: against our Strategic Plan ABOUT THIS and Policy, Commercial, Legal, Financial, Market and Technology. We cannot REPORT and must not work in silos without appreciation of our surrounding ecosystem, for these stand to shape who we are and what we do, as well as how strongly we deliver. This Report is therefore holistic in looking at an integrated reporting style. TELECOMMUNICATIONS BROADCASTING POSTAL INTERNET PRINTED SECTION ONLINE SECTION This printed Integrated Annual Report strives to provide a holistic An online version of this Integrated overview of the performance of Annual Report can be found at BOCRA and its efforts throughout the www.bocra.org.bw period under review, designed with clear sections and themes for the ease of the reader.