A Novel Phenotype Related to Partial Loss of Function Mutations of the Follicle Stimulating Hormone Receptor
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diagnosis of Abnormalities in Gonadal Development BERNARD GONDOS, M.D
ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 12, No. 4 Copyright © 1982, Institute for Clinical Science, Inc. Diagnosis of Abnormalities in Gonadal Development BERNARD GONDOS, M.D. Department of Pathology, University of Connecticut, Farmington, CT 06032 ABSTRACT The role of the clinical laboratory in the diagnosis of abnormalities in gonadal development is reviewed, beginning with a description of the normal differentiation of the ovary and testis and the major types of disorders encountered. The conditions are classified as resulting from abnormal go nadal differentiation, defective endocrine function or excessive endocrine activity. Germ cell neoplasms are also reviewed. Laboratory procedures utilized in evaluation of gonadal abnormalities include cytogenetic, hor monal, and histopathologic studies. Standard procedures are described as well as newer methods which have undergone increasing use in recent years and other specialized procedures which are under investigation for possible clinical application. Introduction tors may all play a role in the development of structural and functional abnormalities The role of the laboratory in the diagno of gonadal differentiation. As a result, sis of abnormalities in gonadal develop classifications of intersex disorders and ment is particularly important. Because of abnormalities of hormone production are the many varieties of such disorders and often confusing. their complex pathogenesis, the types of The present report reviews the labora laboratory tests utilized are quite varied. tory diagnosis of disorders of gonadal de The applications and significance of these velopment, beginning with a consider tests should be clearly understood, since ation of normal gonadal differentiation proper utilization and evaluation may be and a brief summary of the main categor critical in determining gender role assign ies of abnormalities. -

Prenatalscreen® Standard Technical Report
About PrenatalScreen® Prenatal Test PrenatalScreen® Prenatal Test is a genetic test that analyses fetal DNA, obtained from CVS or amniotic fluid following an invasive prenatal diagnosis, to screen for monogenic disorders in the fetus. Using the latest technologies, including Next Generation Sequencing (NGS), PrenatalScreen® Prenatal Test screen 744 genes for mutations causing over 1.000 severe genetic disorders in the fetus. PrenatalScreen® Prenatal Test allows for a comprehensive care and enables patients to make more informed reproductive decisions. Offering PrenatalScreen® Prenatal Test to a patient during pregnancy allows her to gain more knowledge about the potential to pass along a condition to the fetus. Aim of the test PrenatalScreen® Prenatal Test analyses DNA extracted from fetal cells in the amniotic fluid, collected through amniocentesis, or in the chorionic villi through villocentesis (CVS). The aim of this diagnositc test is to assess severe genetic diseases in the fetus, including the most common diseases in the European population. Genes listed in Table 1 were selected according to the incidence in the population of the disease caused by mutations in such genes, the severity of the clinical phenotype at birth and the importance of the related pathogenetic picture, in accordance with the indications of the American College of Medical Genetics (ACMG)(Grody et al., Genet Med 2013:15:482–483). PrenatalScreen®: Indication for testing PrenatalScreen® Prenatal Test is intended for patients who meet any of the following criteria: • Personal/familial anamnesis of hereditary genetic diseases; • For expectant mothers wishing to reduce the risk of a genetic diseases in the fetus; • For natural or in vitro fertilization (IVF)-derived pregnancies: • For couples using heterologus IVF procedures (egg/sperm donors). -

(12) Patent Application Publication (10) Pub. No.: US 2010/0210567 A1 Bevec (43) Pub
US 2010O2.10567A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2010/0210567 A1 Bevec (43) Pub. Date: Aug. 19, 2010 (54) USE OF ATUFTSINASATHERAPEUTIC Publication Classification AGENT (51) Int. Cl. A638/07 (2006.01) (76) Inventor: Dorian Bevec, Germering (DE) C07K 5/103 (2006.01) A6IP35/00 (2006.01) Correspondence Address: A6IPL/I6 (2006.01) WINSTEAD PC A6IP3L/20 (2006.01) i. 2O1 US (52) U.S. Cl. ........................................... 514/18: 530/330 9 (US) (57) ABSTRACT (21) Appl. No.: 12/677,311 The present invention is directed to the use of the peptide compound Thr-Lys-Pro-Arg-OH as a therapeutic agent for (22) PCT Filed: Sep. 9, 2008 the prophylaxis and/or treatment of cancer, autoimmune dis eases, fibrotic diseases, inflammatory diseases, neurodegen (86). PCT No.: PCT/EP2008/007470 erative diseases, infectious diseases, lung diseases, heart and vascular diseases and metabolic diseases. Moreover the S371 (c)(1), present invention relates to pharmaceutical compositions (2), (4) Date: Mar. 10, 2010 preferably inform of a lyophilisate or liquid buffersolution or artificial mother milk formulation or mother milk substitute (30) Foreign Application Priority Data containing the peptide Thr-Lys-Pro-Arg-OH optionally together with at least one pharmaceutically acceptable car Sep. 11, 2007 (EP) .................................. O7017754.8 rier, cryoprotectant, lyoprotectant, excipient and/or diluent. US 2010/0210567 A1 Aug. 19, 2010 USE OF ATUFTSNASATHERAPEUTIC ment of Hepatitis BVirus infection, diseases caused by Hepa AGENT titis B Virus infection, acute hepatitis, chronic hepatitis, full minant liver failure, liver cirrhosis, cancer associated with Hepatitis B Virus infection. 0001. The present invention is directed to the use of the Cancer, Tumors, Proliferative Diseases, Malignancies and peptide compound Thr-Lys-Pro-Arg-OH (Tuftsin) as a thera their Metastases peutic agent for the prophylaxis and/or treatment of cancer, 0008. -

WES Gene Package Disorders of Sex Development (DSD)
Whole Exome Sequencing Gene package Disorders of Sex Development (DSD), version 4, 8‐7‐2016 Technical information After DNA was enriched using Agilent Sureselect Clinical Research Exome (CRE) Capture, samples were run on the Illumina Hiseq platform. The aim is to obtain 50 million total reads per exome with a mapped fraction >0.98. The average coverage of the exome is ~50x. Data are demultiplexed by Illumina software bcl2fastq. Reads are mapped to the genome using BWA (reference: http://bio‐bwa.sourceforge.net/). Variant detection is performed by Genome Analysis Toolkit (reference: http://www.broadinstitute.org/gatk/). Analysis is performed in Cartagenia using The Variant Calling File (VCF) followed by filtering. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM Transcript median % covered % covered gene symbol gene ID depth >10x >20x AMH Persistent Mullerian duct syndrome, type I, 261550 600957 NM_000479.3 47 100 83 AMHR2 Persistent Mullerian duct syndrome, type II, 261550 600956 NM_020547.2 98 100 100 AR Androgen insensitivity, 300068 313700 NM_000044.3 46 96 89 Spinal and bulbar muscular atrophy of Kennedy, 313200 Androgen insensitivity, partial, with or without breast cancer, 312300 {Prostate -

Essential Roles of COUP-TFII in Leydig Cell Differentiation and Male Fertility
Essential Roles of COUP-TFII in Leydig Cell Differentiation and Male Fertility Jun Qin1, Ming-Jer Tsai1,2*, Sophia Y. Tsai1,2* 1 Department of Molecular and Cellular Biology, Baylor College of Medicine, Houston, Texas, United States of America, 2 Program in Developmental Biology, Baylor College of Medicine, Houston, Texas, United States of America Abstract Chicken Ovalbumin Upstream Promoter-Transcription Factor II (COUP-TFII; also known as NR2F2), is an orphan nuclear receptor of the steroid/thyroid hormone receptor superfamily. COUP-TFII-null mice die during the early embryonic development due to angiogenesis and cardiovascular defects. To circumvent the early embryonic lethality and investigate the physiological function of COUP-TFII, we knocked out COUP-TFII gene in a time-specific manner by using a tamoxifen inducible Cre recombinase. The ablation of COUP-TFII during pre-pubertal stages of male development results in infertility, hypogonadism and spermatogenetic arrest. Homozygous adult male mutants are defective in testosterone synthesis, and administration of testosterone could largely rescue the mutant defects. Notably, the rescued results also provide the evidence that the major function of adult Leydig cell is to synthesize testosterone. Further phenotypic analysis reveals that Leydig cell differentiation is arrested at the progenitor cell stage in the testes of null mice. The failure of testosterone to resumption of Leydig cell maturation in the null mice indicates that COUP-TFII itself is essential for this process. In addition, we identify that COUP-TFII plays roles in progenitor Leydig cell formation and early testis organogenesis, as demonstrated by the ablation of COUP-TFII at E18.5. -

Disorders of Sex Development Panel
Abnormal Genitalia/ Disorders of Sex Development Panel Test code: EN0201 Is a 62 gene panel that includes assessment of non-coding variants. Is ideal for patients presenting with ambiguous genitalia, patients suspected to have a disorder of sexual development and patients suspected to have congenital adrenal hyperplasia (CAH). About Abnormal Genitalia/ Disorders of Sex Development Disorders of sex development (DSD) are a group of congenital conditions characterized by problems in the course of gender patterning, gonadal and sex development. It has been estimated that 1% – 2% of live births have some aspect of DSD. Approximately 5% of infants with DSD have ambiguous genitalia and indeterminate sex at birth. However, the vast majority of these patients do not require corrective surgery. Patients with 46,XY DSD have often impaired androgen synthesis or action and may have normal female external genitalia, while patients with 46,XX DSD conditions have often androgen excess. In 46,XX females, congenital adrenal hyperplasia (CAH) caused by 21-hydroxylase deficiency (21-OHD) is the most common cause of DSD. The estimated prevalence of CAH is 1:10,000 and 90%-95% of cases are due to mutations in CYP21A2. The severity of the condition often depends on the residual enzyme activity subdiving CYP21A2 mutations in severe (classic phenotype, enzyme activity 0%-10%) and mild (non-classic, enzyme activity 20%-50%). Androgen insensitivity syndrome (AIS), caused by mutations in AR, is characterized by feminization of external genitalia and atypical sexual development in 46,XY individuals. The condition may be complete, partial or mild, depending on the level of androgen insensitivity. -

Download CGT Exome V2.0
CGT Exome version 2. -

Early Assessment of Ambiguous Genitalia
LEADING ARTICLE 401 Determination of sex (through duplication of Xp21) and Arch Dis Child: first published as 10.1136/adc.2002.011312 on 21 April 2004. Downloaded from ....................................................................................... Wnt4 (through duplication of 1p35), have been associated with impaired gonadal development and undervirilisa- Early assessment of ambiguous tion in a small number of karyotypic 46 XY males. genitalia Mutations or duplications in the various genes responsible for gonadal A L Ogilvy-Stuart, C E Brain differentiation and the subsequent development of the internal and exter- ................................................................................... nal genital phenotype genes may be responsible for gonadal dysgenesis and A multidisciplinary problem in some cases complete sex reversal (table 1). o discover that there is uncertainty the differentiation of the gonad. The Wnt4 is also expressed in the about the sex of one’s newborn differentiation of the gonad in turn Mu¨llerian ducts and in the absence of Tbaby is devastating and often determines the development of both anti-Mu¨llerian hormone (AMH) (also incomprehensible for most parents. It the internal genital tracts and the known as Mu¨llerian inhibiting sub- is paramount that clear explanations external genitalia and thus phenotypic stance) and testosterone, Mu¨llerian and investigations are commenced sex, which occurs later in development structures develop, while the Wolffian promptly, and that no attempt is made (from about 5–6 weeks of gestation). ducts involute.4 AMH promotes regres- to guess the sex of the baby. Extreme Both male and female genitalia differ- sion of Mu¨llerian structures and as the sensitivity is required, and ideally the entiate from the same structures along only source of AMH in the fetus is the baby should be managed in a tertiary the urogenital ridge. -

Biomarkers of Male Hypogonadism in Childhood and Adolescence
Adv Lab Med 2020; 20200024 Review Rodolfo A. Rey* Biomarkers of male hypogonadism in childhood and adolescence https://doi.org/10.1515/almed-2020-0024 Introduction Received December 22, 2019; accepted January 19, 2020; published online April 21, 2020 Hypogonadism in males is typically defined as a testicular failure characterized by androgen deficiency. Although this Abstract definition is widely accepted in the endocrinology of adults, Objectives: The objective of this review was to charac- it is hardly useful in pediatric patients [1]. To better under- fi terize the use of biomarkers of male hypogonadism in stand the dif culties that may arise from an inadequate use fi childhood and adolescence. of this de nition of hypogonadism in children and adoles- Contents: The hypothalamic-pituitary-gonadal (HPG) axis cents, it is necessary to consider the developmental physio- is active during fetal life and over the first months of pathology of the hypothalamic-pituitary-gonadal (HPG) axis. postnatal life. The pituitary gland secretes follicle stimu- lating hormone (FSH) and luteinizing hormone (LH), whereas the testes induce Leydig cells to produce testos- Developmental physiology of the terone and insulin-like factor 3 (INSL), and drive Sertoli HPG axis cells to secrete anti-Müllerian hormone (AMH) and inhibin B. During childhood, serum levels of gonadotropins, Testis differentiation occurs by the 6th week of embryonic testosterone and insulin-like 3 (INSL3) decline to unde- development (week 8 after last menstrual period (LMP)) tectable levels, whereas levels of AMH and inhibin B before HPG axis function is activated [2]. The seminiferous remain high. During puberty, the production of gonado- cords originate from interaction of Sertoli cells, which sur- tropins, testosterone, and INSL3 is reactivated, inhibin B round germ cells, whereas Leydig cells appear in interstitial increases, and AMH decreases as a sign of Sertoli cell tissue. -
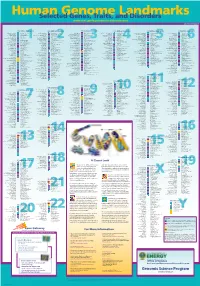
Genomeposter2009.Pdf
Fold HumanSelected Genome Genes, Traits, and Landmarks Disorders www.ornl.gov/hgmis/posters/chromosome genomics.energy. -

The Endocrine Function of Osteocalcin Regulated by Bone Resorption: a Lesson from Reduced and Increased Bone Mass Diseases
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Archivio della ricerca- Università di Roma La Sapienza International Journal of Molecular Sciences Review The Endocrine Function of Osteocalcin Regulated by Bone Resorption: A Lesson from Reduced and Increased Bone Mass Diseases Michela Rossi 1 , Giulia Battafarano 1, Jessica Pepe 2, Salvatore Minisola 2 and Andrea Del Fattore 1,* 1 Bone Physiopathology Group, Multifactorial Disease and Complex Phenotype Research Area, Bambino Gesù Children’s Hospital, IRCCS, 00146 Rome, Italy; [email protected] (M.R.); [email protected] (G.B.) 2 Department of Internal Medicine and Medical Disciplines, Sapienza University of Rome, 00186 Rome, Italy; [email protected] (J.P.); [email protected] (S.M.) * Correspondence: [email protected] Received: 28 August 2019; Accepted: 10 September 2019; Published: 11 September 2019 Abstract: Bone is a peculiar tissue subjected to a continuous process of self-renewal essential to assure the integrity of the skeleton and to explicate the endocrine functions. The study of bone diseases characterized by increased or reduced bone mass due to osteoclast alterations has been essential to understand the great role played by osteocalcin in the endocrine functions of the skeleton. The ability of osteoclasts to regulate the decarboxylation of osteocalcin and to control glucose metabolism, male fertility, and cognitive functions was demonstrated by the use of animal models. In this review we described how diseases characterized by defective and increased bone resorption activity, as osteopetrosis and osteoporosis, were essential to understand the involvement of bone tissue in whole body physiology. -

Expanded Carrier Screening: a Current Perspective
European Journal of Obstetrics & Gynecology and Reproductive Biology 230 (2018) 41–54 Contents lists available at ScienceDirect European Journal of Obstetrics & Gynecology and Reproductive Biology journal homepage: www.elsevier.com/locate/ejogrb Review article Expanded carrier screening: A current perspective a a, b c Enrica Mastantuoni , Gabriele Saccone *, Huda B. Al-Kouatly , Mariano Paternoster , a a a a Pietro D’Alessandro , Bruno Arduino , Luigi Carbone , Giuseppina Esposito , a a a b Antonio Raffone , Valentino De Vivo , Giuseppe Maria Maruotti , Vincenzo Berghella , a Fulvio Zullo a Department of Neuroscience, Reproductive Sciences and Dentistry, School of Medicine, University of Naples Federico II, Naples, Italy b Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA, USA c Department of Advanced Biomedical Sciences, School of Medicine, University of Naples Federico II, Naples, Italy A R T I C L E I N F O A B S T R A C T Article history: Prenatal carrier screening has expanded to include a large number of genes offered to all couples Received 26 June 2018 considering pregnancy or with an ongoing pregnancy. Expanded carrier screening refers to identification Received in revised form 9 August 2018 of carriers of single-gene disorders outside of traditional screening guidelines. Expanded carrier Accepted 10 September 2018 screening panels include numerous autosomal recessive and X-linked genetic conditions, including those Available online xxx with a very low carrier frequency, as well as those with mild or incompletely penetrant phenotype. Therefore, the clinical utility of these panels is still subject of debate.