Lichen Simplex Chronicus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Diagnostic Approach to Pruritus
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by DigitalCommons@University of Nebraska University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln U.S. Air Force Research U.S. Department of Defense 2011 A Diagnostic Approach to Pruritus Brian V. Reamy Christopher W. Bunt Stacy Fletcher Follow this and additional works at: https://digitalcommons.unl.edu/usafresearch This Article is brought to you for free and open access by the U.S. Department of Defense at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in U.S. Air Force Research by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. A Diagnostic Approach to Pruritus BRIAN V. REAMY, MD, Uniformed Services University of the Health Sciences, Bethesda, Maryland CHRISTOPHER W. BUNT, MAJ, USAF, MC, and STACY FLETCHER, CAPT, USAF, MC Ehrling Bergquist Family Medicine Residency Program, Offutt Air Force Base, Nebraska, and the University of Nebraska Medical Center, Omaha, Nebraska Pruritus can be a symptom of a distinct dermatologic condition or of an occult underlying systemic disease. Of the patients referred to a dermatologist for generalized pruritus with no apparent primary cutaneous cause, 14 to 24 percent have a systemic etiology. In the absence of a primary skin lesion, the review of systems should include evaluation for thyroid disorders, lymphoma, kidney and liver diseases, and diabetes mellitus. Findings suggestive of less seri- ous etiologies include younger age, localized symptoms, acute onset, involvement limited to exposed areas, and a clear association with a sick contact or recent travel. Chronic or general- ized pruritus, older age, and abnormal physical findings should increase concern for underly- ing systemic conditions. -

Genital Lichen Simplex Chronicus (Eczema, Neurodermatitis, Dermatitis) !
Libby Edwards, MD Genital Lichen Simplex Chronicus (eczema, neurodermatitis, dermatitis) ! Lichen simplex chronicus (LSC), or eczema, is a common skin condition that is very itchy. Although not dangerous in any way, both the itching, and the pain from rubbing and scratching, can be miserable. Eczema/LSC of the genital area most often affects the scrotum of men, the vulva of women, or the rectal skin of both. Many people with eczema/LSC have had sensitive skin or eczema/LSC on other areas of the skin at some point, and many have a tendency towards allergies, especially hay fever or asthma. ! The skin usually appears red or dark, and thick from rubbing and scratching, sometimes with sores from scratching. ! The cause of eczema/LSC is not entirely clear. However, eczema/LSC starts with irritation that triggers itching. Often, at the office visit with the health care provider, the original infection or other initial cause of irritation is no longer present. Common triggers include a yeast or fungus infection, an irritating medication, moisturizer or lubricant, a wet bathing suit, anxiety or depression, over-washing, panty liners, sweat, heat, urine, a contraceptive jelly, an irritating condom, or any other activity or substance that can irritate the skin and start the itching. ! Although rubbing and scratching often feel good at first, rubbing irritates the skin and ultimately makes itching even worse, so that there is more scratching, then more itching, then more scratching. This is called the “itch-scratch cycle.” Treatment is very effective and requires clearing any infection and avoiding irritants as well as using a strong cortisone. -

ORIGINAL ARTICLE a Clinical and Histopathological Study of Lichenoid Eruption of Skin in Two Tertiary Care Hospitals of Dhaka
ORIGINAL ARTICLE A Clinical and Histopathological study of Lichenoid Eruption of Skin in Two Tertiary Care Hospitals of Dhaka. Khaled A1, Banu SG 2, Kamal M 3, Manzoor J 4, Nasir TA 5 Introduction studies from other countries. Skin diseases manifested by lichenoid eruption, With this background, this present study was is common in our country. Patients usually undertaken to know the clinical and attend the skin disease clinic in advanced stage histopathological pattern of lichenoid eruption, of disease because of improper treatment due to age and sex distribution of the diseases and to difficulties in differentiation of myriads of well assess the clinical diagnostic accuracy by established diseases which present as lichenoid histopathology. eruption. When we call a clinical eruption lichenoid, we Materials and Method usually mean it resembles lichen planus1, the A total of 134 cases were included in this study prototype of this group of disease. The term and these cases were collected from lichenoid used clinically to describe a flat Bangabandhu Sheikh Mujib Medical University topped, shiny papular eruption resembling 2 (Jan 2003 to Feb 2005) and Apollo Hospitals lichen planus. Histopathologically these Dhaka (Oct 2006 to May 2008), both of these are diseases show lichenoid tissue reaction. The large tertiary care hospitals in Dhaka. Biopsy lichenoid tissue reaction is characterized by specimen from patients of all age group having epidermal basal cell damage that is intimately lichenoid eruption was included in this study. associated with massive infiltration of T cells in 3 Detailed clinical history including age, sex, upper dermis. distribution of lesions, presence of itching, The spectrum of clinical diseases related to exacerbating factors, drug history, family history lichenoid tissue reaction is wider and usually and any systemic manifestation were noted. -

Common Dermatoses in Patients with Obsessive Compulsive Disorders Mircea Tampa Carol Davila University of Medicine and Pharmacy, Tampa [email protected]
Journal of Mind and Medical Sciences Volume 2 | Issue 2 Article 7 2015 Common Dermatoses in Patients with Obsessive Compulsive Disorders Mircea Tampa Carol Davila University of Medicine and Pharmacy, [email protected] Maria Isabela Sarbu Victor Babes Hospital for Infectious and Tropical Diseases, [email protected] Clara Matei Carol Davila University of Medicine and Pharmacy Vasile Benea Victor Babes Hospital for Infectious and Tropical Diseases Simona Roxana Georgescu Carol Davila University of Medicine and Pharmacy Follow this and additional works at: http://scholar.valpo.edu/jmms Part of the Medicine and Health Sciences Commons Recommended Citation Tampa, Mircea; Sarbu, Maria Isabela; Matei, Clara; Benea, Vasile; and Georgescu, Simona Roxana (2015) "Common Dermatoses in Patients with Obsessive Compulsive Disorders," Journal of Mind and Medical Sciences: Vol. 2 : Iss. 2 , Article 7. Available at: http://scholar.valpo.edu/jmms/vol2/iss2/7 This Review Article is brought to you for free and open access by ValpoScholar. It has been accepted for inclusion in Journal of Mind and Medical Sciences by an authorized administrator of ValpoScholar. For more information, please contact a ValpoScholar staff member at [email protected]. JMMS 2015, 2(2): 150- 158. Review Common dermatoses in patients with obsessive compulsive disorders Mircea Tampa1, Maria Isabela Sarbu2, Clara Matei1, Vasile Benea2, Simona Roxana Georgescu1 1 Carol Davila University of Medicine and Pharmacy, Department of Dermatology and Venereology 2 Victor Babes Hospital for Infectious and Tropical Diseases, Department of Dermatology and Venereology Corresponding author: Maria Isabela Sarbu, e-mail: [email protected] Running title: Dermatoses in obsessive compulsive disorders Keywords: Factitious disorders, obsessive-compulsive disorders, acne excoriee www.jmms.ro 2015, Vol. -

Triamcinolone Acetonide Injectable Suspension, USP)
KENALOG®-10 INJECTION (triamcinolone acetonide injectable suspension, USP) NOT FOR USE IN NEONATES CONTAINS BENZYL ALCOHOL For Intra-articular or Intralesional Use Only NOT FOR INTRAVENOUS, INTRAMUSCULAR, INTRAOCULAR, EPIDURAL, OR INTRATHECAL USE DESCRIPTION Kenalog®-10 Injection (triamcinolone acetonide injectable suspension, USP) is triamcinolone acetonide, a synthetic glucocorticoid corticosteroid with marked anti-inflammatory action, in a sterile aqueous suspension suitable for intralesional and intra-articular injection. THIS FORMULATION IS SUITABLE FOR INTRA-ARTICULAR AND INTRALESIONAL USE ONLY. Each mL of the sterile aqueous suspension provides 10 mg triamcinolone acetonide, with 0.66% sodium chloride for isotonicity, 0.99% (w/v) benzyl alcohol as a preservative, 0.63% carboxymethylcellulose sodium, and 0.04% polysorbate 80. Sodium hydroxide or hydrochloric acid may have been added to adjust pH between 5.0 and 7.5. At the time of manufacture, the air in the container is replaced by nitrogen. The chemical name for triamcinolone acetonide is 9-Fluoro-11β,16α,17,21-tetrahydroxypregna- 1,4-diene-3,20-dione cyclic 16,17-acetal with acetone. Its structural formula is: 1 Reference ID: 4241593 MW 434.50 CLINICAL PHARMACOLOGY Glucocorticoids, naturally occurring and synthetic, are adrenocortical steroids that are readily absorbed from the gastrointestinal tract. Naturally occurring glucocorticoids (hydrocortisone and cortisone), which also have salt- retaining properties, are used as replacement therapy in adrenocortical deficiency states. -
The Dyshidrotic Eczema Area and Severity Index – a Score Developed for the Assessment of Dyshidrotic Eczema
Clinical and Laboratory Investigations Dermatology 1999;198:265–269 Received: September 29, 1998 Accepted: February 19, 1999 The Dyshidrotic Eczema Area and Severity Index – A Score Developed for the Assessment of Dyshidrotic Eczema E. Vocks a S.G. Plötz b J. Ring a aDepartment of Dermatology and Allergology Biederstein, Technical University München, and bResearch Center Borstel, Center for Medicine and Bioscience, Borstel, Germany Key Words factors, such as atopic eczema, contact allergy or mycosis, Severity index • Dyshidrotic eczema • Pompholyx • but many cases are also classified as idiopathic [1–3]. As it Treatment study can be very resistant to treatment [4], studies with regard to new therapeutic modalities in dyshidrotic eczema are important. The evaluation of therapeutic effects is carried Abstract out by different methods. In most studies global assessment Background: Dyshidrotic eczema of the palms and soles methods like grading of improvement [5–8] are used. Hand is a common condition, which can be rather resistant to eczema scoring systems which are applied to eczema on the treatment. Therapy studies and their comparability are of palmar and dorsal hands are not specific for the distinct fea- clinical importance. Objective: As standardized assess- tures of dyshidrotic eczema [9]. Since the assessment meth- ment methods for the severity of this particular form of ods for dyshidrotic eczema are not standardized, therapeutic eczema are lacking, we developed a severity index for studies are not comparable and data cannot be utilized for dyshidrotic eczema. Methods: The Dyshidrotic Eczema epidemiologic purposes. As there is no specific scoring sys- Area and Severity Index (DASI) is based on the severity tem existing, we developed a severity index for dyshidrotic grade of single items – number of vesicles per square eczema on the occasion of a half-side treatment study with centimetre (V), erythema (E), desquamation (S) and itch tap water iontophoresis [10]. -

Skin Signs of Rheumatic Disease Gideon P
Skin Signs of Rheumatic Disease Gideon P. Smith MD PhD MPH Vice Chair for Clinical Affairs Director of Rheumatology-Dermatology Program Director of Connective Tissue Diseases Fellowship Associate Director of Clinical Trials Department of Dermatology Massachusetts General Hospital Harvard University www.mghcme.org Disclosures “Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest to disclose.” www.mghcme.org CONNECTIVE TISSUE DISEASES CLINIC •Schnitzlers •Interstitial •Chondrosarcoma •Eosinophilic Fasciitis Granulomatous induced •Silicone granulomas Dermatitis with Dermatomyositis Arthritis •AML arthritis with •Scleroderma granulomatous papules •Cutaneous Crohn’s •Lyme arthritis with with arthritis •Follicular mucinosis in papular mucinosis JRA post-infliximab •Acral Anetoderma •Celiac Lupus •Calcinosis, small and •Granulomatous exophytic •TNF-alpha induced Mastitis sarcoid •NSF, Morphea •IgG4 Disease •Multicentric Reticul •EED, PAN, DLE ohistiocytosis www.mghcme.org • Primary skin disease recalcitrant to therapy Common consults • Hair loss • Nail dystrophy • Photosensitivity • Cosmetic concerns – post- inflammatory pigmentation, scarring, volume loss, premature photo-aging • Erythromelalgia • Dry Eyes • Dry Mouth • Oral Ulcerations • Burning Mouth Syndrome • Urticaria • Itch • Raynaud’s • Digital Ulceration • Calcinosis cutis www.mghcme.org Todays Agenda Clinical Presentations Rashes (Cutaneous Lupus vs Dermatomyositis vs ?) Hard Skin (Scleroderma vs Other sclerosing disorders) www.mghcme.org -

Swimmer's Itch Fact Sheet
Fact Sheet for the general public Swimmer’s Itch (Cercarial Dermatitis) What is swimmer's itch? Swimmer's itch, also called cercarial dermatitis (sir-CARE-ee-uhl der-muh-TIGHT-iss), appears as a skin rash caused by an allergic reaction to certain parasites that infect some birds and mammals. These microscopic parasites are released from infected snails into fresh and salt water (such as lakes, ponds, and oceans). While the parasite’s preferred host is the specific bird or mammal, if the parasite comes into contact with a swimmer, it burrows into the skin causing an allergic reaction and rash. Swimmer’s itch is found throughout the world and is more frequent during summer months. How does water become infested with the parasite? The adult parasite lives in the blood of infected animals such as ducks, geese, gulls, swans, and certain aquatic mammals such as muskrats and beavers. The parasites produce eggs that are passed in the feces of infected birds or mammals. If the eggs land in or are washed into water, the eggs hatch, releasing small, free-swimming larvae. These larvae swim in the water in search of a certain species of aquatic snail. If the larvae find one of these snails, they infect the snail, multiply and undergo further development. Infected snails release a different type of larvae (or cercariae, hence the name cercarial dermatitis) into the water. This larval form then swims about searching for a suitable host (bird, muskrat) to continue the life cycle. Although humans are not suitable hosts, the larvae burrow into the swimmer’s skin, and may cause an allergic reaction and rash. -
Understanding Eczema / Atopic Dermatitis
Understanding Atopic Dermatitis An educational health series from National Jewish Health If you would like further information about National Jewish Health, please write to: National Jewish Health 1400 Jackson Street Denver, Colorado 80206 or visit: njhealth.org Understanding Atopic Dermatitis An educational health series from National Jewish Health IN THIS ISSUE About Atopic Dermatitis 2 What Causes Atopic Dermatitis? 3 Do You Have Atopic Dermatitis? 3 Should You Go to an Expert? 4 What Are Your Goals? 4 Avoiding Things that Make Itching and Rash Worse 5 Treatment and Medication Therapy 9 Soak and Seal 9 What Medicines Will Help? 10 Action Plan for Atopic Dermatitis 13 What to Do When Symptoms Are Severe 14 Living with Atopic Dermatitis 15 Remember Your Goals 15 Glossary 16 Note: This information is provided to you as an educational service of National Jewish Health. It is not meant as a substitute for your own doctor. © Copyright 2018, National Jewish Health About Atopic Dermatitis Atopic dermatitis is a common chronic skin disease. It is also called atopic eczema. Atopic is a term used to describe allergic conditions such as asthma and hay fever. Both dermatitis and eczema mean inflammation of the skin. People with atopic dermatitis tend to have dry, itchy and easily irritated skin. They may have times when their skin is clear and other times when they have rash. INFANTS AND SMALL CHILDREN In infants and small children, the rash is often present on face, as well as skin around the knees and elbows. TEENAGERS AND ADULTS In teenagers and adults, the rash is often present in the creases of the wrists, elbows, knees or ankles, and on the face or neck. -

How to Treat Dandruff
HOW TO TREAT DANDRUFF Dandruff is a common scalp condition in which small pieces of dry skin flake off of the scalp. The most effective way to treat and control dandruff is to use dandruff shampoo and scalp treatments. Follow these tips from dermatologists to get the best results. Dandruff is a common scalp condition in which small pieces of dry skin flake off of the scalp. If you have dark hair or you’re wearing dark colors, you may notice the flakes in your hair or on your shoulders. Dandruff may also make your scalp itch. Many people believe that dandruff is caused by poor hygiene, but this is not true. Although infrequent shampooing can make dandruff more obvious, researchers are still studying the causes, which appear to be complex. The most effective way to treat and control dandruff is to use dandruff shampoo and scalp treatments. Follow these tips from dermatologists to get the best results: 1. Follow the instructions on the dandruff shampoo bottle. There are many different dandruff shampoos, and each contains different active ingredients for controlling symptoms. To get the best results, always follow the instructions on the bottle. For example, some dandruff shampoos require that you lather the shampoo into the hair and scalp and leave the shampoo in for about five minutes before rinsing. Others should not be left on the scalp. 2. If you are Caucasian or Asian, shampoo daily and use dandruff shampoo twice a week. If using one dandruff shampoo does not bring relief, try alternating between dandruff shampoos with different active ingredients. -
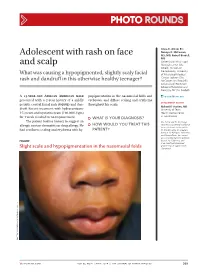
Adolescent with Rash on Face and Scalp
Photo RoUNDS Anna K. Allred, BS; Nancye K. McCowan, Adolescent with rash on face MS, MD; Robert Brodell, MD University of Mississippi and scalp Medical Center (Ms. Allred); Division of Dermatology, University What was causing a hypopigmented, slightly scaly facial of Mississippi Medical Center, Jackson (Drs. rash and dandruff in this otherwise healthy teenager? McCowan and Brodell); University of Rochester School of Medicine and Dentistry, NY (Dr. Brodell) A 13-year-old African American male popigmentation in the nasomesial folds and [email protected] presented with a 2-year history of a mildly eyebrows, and diffuse scaling and erythema DEpartment EDItOR pruritic central facial rash (FIGURE) and dan- throughout his scalp. Richard p. Usatine, MD druff. Recent treatment with hydrocortisone University of Texas 1% cream and nystatin cream (100,000 U/gm) Health Science Center at San Antonio for 1 week resulted in no improvement. ● What is youR diAgnosis? The patient had no history to suggest an Ms. Allred and Dr. McCowan allergic contact dermatitis or drug allergy. He ● HoW Would you TReAT THIS reported no potential conflict of interest relevant to this article. had confluent scaling and erythema with hy- pATIENT? Dr. Brodell serves on speaker’s bureaus for Allergan, Galderma, and PharmaDerm, has served as a consultant and on advisory Figure boards for Galderma, and is an investigator/received grant/research support from Slight scale and hypopigmentation in the nasomesial folds Genentech. PHO T o COU RT ESY OF : R o B e RT BR ODELL , MD jfponline.com Vol 63, no 4 | ApRIL 2014 | The jouRnAl of Family PracTice 209 PHOTO RoUNDS Diagnosis: the Malassezia yeast and topical steroids are Seborrheic dermatitis used to suppress inflammation. -

Chronic Pruritic Vulva Lesion
Photo RoUNDS Stephen Colden Cahill, DO Chronic pruritic vulva lesion College of Osteopathic Medicine, Michigan State University, East Lansing; The patient was not sexually active and denied any and Lakeshore Health vaginal discharge. So what was causing the intense Partners, Holland, Mich itching on her labia? [email protected] Department eDItOr richard p. Usatine, mD University of Texas Health Science Center at San Antonio During a routine exam, a 45-year-old Cau- both of her labia majora (FIGURE). Throughout casian woman complained of intense itching the lesion, there were scattered areas of exco- The author reported no potential conflict of interest on her labia. She said that the itching had been riation. Her labia minor were spared. relevant to this article. an issue for more than 9 months and that she A speculum and bimanual exam were found herself scratching several times a day. normal. No inguinal lymphadenopathy was She denied any vaginal discharge and said she present. hadn’t been sexually active in years. She had tried over-the-counter antifungals and topical ● WhaT is your diagnosis? Benadryl, but they provided only limited relief. The patient had red thickened plaques ● HoW Would you TREAT THIS with accentuated skin lines (furrows) covering PATIENT? Figure Red thickened plaques on labia majora p ho T o cour T esy of: St ephen c olden c ahill, DO jfponline.com Vol 62, no 2 | february 2013 | The journal of family pracTice 97 PHOTO RoUNDS Diagnosis: taneous lesion of unknown etiology. It can Lichen simplex chronicus be found throughout the body, including the This patient was given a diagnosis of lichen mucous membranes.