NCCC Guidelines for Management of Late Onset (≥ 7 DOL) Neonatal Sepsis SUSPECT SEPSIS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ceftazidime for Injection) PHARMACY BULK PACKAGE – NOT for DIRECT INFUSION
PRESCRIBING INFORMATION FORTAZ® (ceftazidime for injection) PHARMACY BULK PACKAGE – NOT FOR DIRECT INFUSION To reduce the development of drug-resistant bacteria and maintain the effectiveness of FORTAZ and other antibacterial drugs, FORTAZ should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTION Ceftazidime is a semisynthetic, broad-spectrum, beta-lactam antibacterial drug for parenteral administration. It is the pentahydrate of pyridinium, 1-[[7-[[(2-amino-4 thiazolyl)[(1-carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thia-1 azabicyclo[4.2.0]oct-2-en-3-yl]methyl]-, hydroxide, inner salt, [6R-[6α,7β(Z)]]. It has the following structure: The molecular formula is C22H32N6O12S2, representing a molecular weight of 636.6. FORTAZ is a sterile, dry-powdered mixture of ceftazidime pentahydrate and sodium carbonate. The sodium carbonate at a concentration of 118 mg/g of ceftazidime activity has been admixed to facilitate dissolution. The total sodium content of the mixture is approximately 54 mg (2.3 mEq)/g of ceftazidime activity. The Pharmacy Bulk Package vial contains 709 mg of sodium carbonate. The sodium content is approximately 54 mg (2.3mEq) per gram of ceftazidime. FORTAZ in sterile crystalline form is supplied in Pharmacy Bulk Packages equivalent to 6g of anhydrous ceftazidime. The Pharmacy Bulk Package bottle is a container of sterile preparation for parenteral use that contains many single doses. The contents are intended for use in a pharmacy admixture program and are restricted to the preparation of admixtures for intravenous use. THE PHARMACY BULK PACKAGE IS NOT FOR DIRECT INFUSION, FURTHER DILUTION IS REQUIRED BEFORE USE. -

Activity of Aztreonam in Combination with Ceftazidime-Avibactam Against
Diagnostic Microbiology and Infectious Disease 99 (2021) 115227 Contents lists available at ScienceDirect Diagnostic Microbiology and Infectious Disease journal homepage: www.elsevier.com/locate/diagmicrobio Activity of aztreonam in combination with ceftazidime–avibactam against serine- and metallo-β-lactamase–producing ☆ ☆☆ ★ Pseudomonas aeruginosa , , Michelle Lee a, Taylor Abbey a, Mark Biagi b, Eric Wenzler a,⁎ a College of Pharmacy, University of Illinois at Chicago, Chicago, IL, USA b College of Pharmacy, University of Illinois at Chicago, Rockford, IL, USA article info abstract Article history: Existing data support the combination of aztreonam and ceftazidime–avibactam against serine-β-lactamase Received 29 June 2020 (SBL)– and metallo-β-lactamase (MBL)–producing Enterobacterales, although there is a paucity of data against Received in revised form 15 September 2020 SBL- and MBL-producing Pseudomonas aeruginosa. In this study, 5 SBL- and MBL-producing P. aeruginosa (1 Accepted 19 September 2020 IMP, 4 VIM) were evaluated against aztreonam and ceftazidime–avibactam alone and in combination via broth Available online xxxx microdilution and time-kill analyses. All 5 isolates were nonsusceptible to aztreonam, aztreonam–avibactam, – – Keywords: and ceftazidime avibactam. Combining aztreonam with ceftazidime avibactam at subinhibitory concentrations Metallo-β-lactamase produced synergy and restored bactericidal activity in 4/5 (80%) isolates tested. These results suggest that the VIM combination of aztreonam and ceftazidime–avibactam may be a viable treatment option against SBL- and IMP MBL-producing P. aeruginosa. Aztreonam © 2020 Elsevier Inc. All rights reserved. Ceftazidime–avibactam Synergy 1. Introduction of SBLs and MBLs harbored by P. aeruginosa are fundamentally different than those in Enterobacterales (Alm et al., 2015; Kazmierczak et al., The rapid global dissemination of Ambler class B metallo-β- 2016; Periasamy et al., 2020; Poirel et al., 2000; Watanabe et al., lactamase (MBL) enzymes along with their increasing diversity across 1991). -

Global Assessment of the Antimicrobial Activity of Polymyxin B Against 54 731 Clinical Isolates of Gram-Negative Bacilli
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector ORIGINAL ARTICLE 10.1111/j.1469-0691.2005.01351.x Global assessment of the antimicrobial activity of polymyxin B against 54 731 clinical isolates of Gram-negative bacilli: report from the SENTRY antimicrobial surveillance programme (2001–2004) A. C. Gales1, R. N. Jones2,3 and H. S. Sader1,2 1Division of Infectious Diseases, Universidade Federal de Sa˜o Paulo, Sa˜o Paulo, Brazil, 2JMI Laboratories, North Liberty, IA, USA, and 3Tufts University School of Medicine, Boston, MA, USA ABSTRACT In total, 54 731 Gram-negative bacilli isolated worldwide between 2001 and 2004 from diverse sites of infection were tested for susceptibility to polymyxin B by the broth reference microdilution method, with interpretation of results according to CLSI (formerly NCCLS) guidelines. Polymyxin B showed excellent potency and spectrum against 8705 Pseudomonas aeruginosa and 2621 Acinetobacter spp. isolates (MIC50, £ ⁄ ⁄ 1mg L and MIC90,2mg L for both pathogens). Polymyxin B resistance rates were slightly higher for carbapenem-resistant P. aeruginosa (2.7%) and Acinetobacter spp. (2.8%), or multidrug-resistant (MDR) P. aeruginosa (3.3%) and Acinetobacter spp. (3.2%), when compared with the entire group (1.3% for P. aeruginosa and 2.1% for Acinetobacter spp.). Among P. aeruginosa, polymyxin B resistance rates varied from 2.9% in the Asia-Pacific region to only 1.1% in Europe, Latin America and North America, while polymyxin B resistance rates ranged from 2.7% in Europe to 1.7% in North America and Latin America £ ⁄ % among Acinetobacter spp. -
A Phase I, 3-Part Placebo-Controlled Randomised Trial to Evaluate the Safety, Tolerability and Pharmacokinetics of Aztreonam-Av
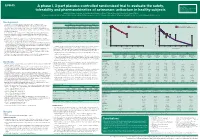
EV0643 Contactinformation: A phase I, 3-part placebo-controlled randomised trial to evaluate the safety, SeamusO’Brien AstraZenecaResearch&Development Macclesfield,Cheshire,UK tolerability and pharmacokinetics of aztreonam-avibactam in healthy subjects [email protected] Timi Edeki1, Diansong Zhou2, Frans van den Berg3, Helen Broadhurst4, William C. Holmes5, Gary Peters3, Maria Sunzel6, Seamus O’Brien4 1AstraZeneca, Wilmington, DE, USA; 2AstraZeneca, Waltham, MA, USA; 3Hammersmith Medicines Research, London, UK; 4AstraZeneca, Macclesfield, UK; 5AstraZeneca, Gaithersburg, MD, USA; 6Contractor at AstraZeneca, Wilmington, DE, USA Background Table 1.Subjects’baselinecharacteristics Figure 1. Geometricmean(A)aztreonamand(B)avibactamconcentration-timeprofilesinPartAfollowingindividualandcombinedadministrationofaztreonam2000mgandavibactam600mgby1-hIVinfusion Part A Part B Part C • Theemergenceandglobaldisseminationofmetallo-β-lactamase(MBL)-producing (A) (B) Enterobacteriaceae,includingNDM-typeandVIM-type,whichareresistanttocarbapenems, Active Placebo Active Placebo Active Placebo 100 Aztreonam 2000 mg alone (n=7) 100 Avibactam 600 mg alone (n=8) representsanurgentthreattohumanhealthforwhichfewtreatmentoptionscurrentlyexist.1, 2 (n=8) (n=4) (n=40) (n=16) (n=18) (n=6) Aztreonam-avibactam 2000-600 mg (n=7) Aztreonam-avibactam 2000-600 mg (n=7) • Aztreonam,amonobactamβ-lactam,isstabletoAmblerclassBMBLsincludingNDM-typeand Mean(SD)age,years 31(7) 34(7) 30(7) 27(5) 49(19) 51(19) VIM-type.However,bacteriathatexpressMBLsfrequentlyco-expressotherclassesofβ-lactamase -

UNASYN® (Ampicillin Sodium/Sulbactam Sodium)
® UNASYN (ampicillin sodium/sulbactam sodium) To reduce the development of drug-resistant bacteria and maintain the effectiveness of UNASYN® and other antibacterial drugs, UNASYN should be used only to treat infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTION UNASYN is an injectable antibacterial combination consisting of the semisynthetic antibacterial ampicillin sodium and the beta-lactamase inhibitor sulbactam sodium for intravenous and intramuscular administration. Ampicillin sodium is derived from the penicillin nucleus, 6-aminopenicillanic acid. Chemically, it is monosodium (2S, 5R, 6R)-6-[(R)-2-amino-2-phenylacetamido]-3, 3-dimethyl-7-oxo-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylate and has a molecular weight of 371.39. Its chemical formula is C16H18N3NaO4S. The structural formula is: COONa O CH 3 N CH O 3 NH S NH 2 1 Reference ID: 4053909 Sulbactam sodium is a derivative of the basic penicillin nucleus. Chemically, sulbactam sodium is sodium penicillinate sulfone; sodium (2S, 5R)-3,3-dimethyl-7-oxo-4-thia- 1-azabicyclo [3.2.0] heptane-2-carboxylate 4,4-dioxide. Its chemical formula is C8H10NNaO5S with a molecular weight of 255.22. The structural formula is: COONa CH 3 O N CH 3 S O O UNASYN, ampicillin sodium/sulbactam sodium parenteral combination, is available as a white to off-white dry powder for reconstitution. UNASYN dry powder is freely soluble in aqueous diluents to yield pale yellow to yellow solutions containing ampicillin sodium and sulbactam sodium equivalent to 250 mg ampicillin per mL and 125 mg sulbactam per mL. The pH of the solutions is between 8.0 and 10.0. -

Antimicrobial Stewardship Guidance
Antimicrobial Stewardship Guidance Federal Bureau of Prisons Clinical Practice Guidelines March 2013 Clinical guidelines are made available to the public for informational purposes only. The Federal Bureau of Prisons (BOP) does not warrant these guidelines for any other purpose, and assumes no responsibility for any injury or damage resulting from the reliance thereof. Proper medical practice necessitates that all cases are evaluated on an individual basis and that treatment decisions are patient-specific. Consult the BOP Clinical Practice Guidelines Web page to determine the date of the most recent update to this document: http://www.bop.gov/news/medresources.jsp Federal Bureau of Prisons Antimicrobial Stewardship Guidance Clinical Practice Guidelines March 2013 Table of Contents 1. Purpose ............................................................................................................................................. 3 2. Introduction ...................................................................................................................................... 3 3. Antimicrobial Stewardship in the BOP............................................................................................ 4 4. General Guidance for Diagnosis and Identifying Infection ............................................................. 5 Diagnosis of Specific Infections ........................................................................................................ 6 Upper Respiratory Infections (not otherwise specified) .............................................................................. -

Penicillin Allergy Guidance Document
Penicillin Allergy Guidance Document Key Points Background Careful evaluation of antibiotic allergy and prior tolerance history is essential to providing optimal treatment The true incidence of penicillin hypersensitivity amongst patients in the United States is less than 1% Alterations in antibiotic prescribing due to reported penicillin allergy has been shown to result in higher costs, increased risk of antibiotic resistance, and worse patient outcomes Cross-reactivity between truly penicillin allergic patients and later generation cephalosporins and/or carbapenems is rare Evaluation of Penicillin Allergy Obtain a detailed history of allergic reaction Classify the type and severity of the reaction paying particular attention to any IgE-mediated reactions (e.g., anaphylaxis, hives, angioedema, etc.) (Table 1) Evaluate prior tolerance of beta-lactam antibiotics utilizing patient interview or the electronic medical record Recommendations for Challenging Penicillin Allergic Patients See Figure 1 Follow-Up Document tolerance or intolerance in the patient’s allergy history Consider referring to allergy clinic for skin testing Created July 2017 by Macey Wolfe, PharmD; John Schoen, PharmD, BCPS; Scott Bergman, PharmD, BCPS; Sara May, MD; and Trevor Van Schooneveld, MD, FACP Disclaimer: This resource is intended for non-commercial educational and quality improvement purposes. Outside entities may utilize for these purposes, but must acknowledge the source. The guidance is intended to assist practitioners in managing a clinical situation but is not mandatory. The interprofessional group of authors have made considerable efforts to ensure the information upon which they are based is accurate and up to date. Any treatments have some inherent risk. Recommendations are meant to improve quality of patient care yet should not replace clinical judgment. -

Antibiotic Review
8/28/19 Disclosure 2 E. Monee’ Carter-Griffin DNP, MA, RN, ACNP-BC Antibiotic has no financial relationships with commercial Review interests to disclose. Any unlaBeled and/or E. Monee’ Carter-Griffin, DNP, MA, RN, ACNP-BC unapproved uses of drugs or products will Be Associate Chair for Advanced Practice Nursing disclosed. University of Texas at Arlington, College of Nursing & Health Innovation Dallas Pulmonary & Critical Care, PA • Identify the general characteristics of • SusceptiBility à determine which antibiotics. antibiotics a bacteria is sensitive to • Discuss the mechanism of action, • à pharmacokinetics, and spectrum of activity MIC lowest concentration of drug that inhiBits growth of the Bacteria for the most common antiBiotic drug classes. Antibiotic Objectives • Identify commonly prescriBed antiBiotics • Trough à lowest concentration of within the drug classes including dosage Lingo drug in bloodstream range and indication for prescribing. – Collect prior to administration of • Identify special considerations for specific drug antibiotics and/or drug classes. • Peak à highest concentration of • Practice appropriate prescriBing for common drug in bloodstream bacterial infections. • Review Basic antiBiotic stewardship 3 4 principles. • Penicillins • Bactericidal or bacteriostatic • Cephalosporins • Narrow or Broad spectrum • Carbapenems General • Can elicit allergic responses Antibiotic • MonoBactam Characteristics • Affect normal Body flora Drug Classes • Macrolides • Fluoroquinolones • Sulfonamides • Tetracyclines 5 6 1 8/28/19 • Penicillins – Natural penicillins 8 – Aminopenicillins Penicillins Penicillins – Anti-staphylococcal penicillins • Mechanism of action àbactericidal à – Anti-pseudomonal penicillins interrupts cell wall synthesis 7 • Pharmacokinetics • Spectrum of Activity – Gram positive organisms Natural – Penicillin G à mostly given IM, But Natural • Streptococcus species (e.g. S. Penicillins one variation can Be given IV Penicillins pyogenes) • Poorly aBsorBed via PO • Some enterococcus species (e.g. -

Staphylococcus Aureus Bloodstream Infection Treatment Guideline
Staphylococcus aureus Bloodstream Infection Treatment Guideline Purpose: To provide a framework for the evaluation and management patients with Methicillin- Susceptible (MSSA) and Methicillin-Resistant Staphylococcus aureus (MRSA) bloodstream infections (BSI). The recommendations below are guidelines for care and are not meant to replace clinical judgment. The initial page includes a brief version of the guidance followed by a more detailed discussion of the recommendations with supporting evidence. Also included is an algorithm describing management of patients with blood cultures positive for gram-positive cocci. Brief Key Points: 1. Don’t ignore it – Staphylococcus aureus isolated from a blood culture is never a contaminant. All patients with S. aureus in their blood should be treated with appropriate antibiotics and evaluated for a source of infection. 2. Control the source a. Removing infected catheters and prosthetic devices – Retention of infected central venous catheters and prosthetic devices in the setting of S. aureus bacteremia (SAB) has been associated with prolonged bacteremia, treatment failure and death. These should be removed if medically possible. i. Retention of prosthetic material is associated with an increased likelihood of SAB relapse and removal should be considered even if not clearly infected b. Evaluate for metastatic infections (endocarditis, osteomyelitis, abscesses, etc.) – Metastatic infections and endocarditis are quite common in SAB (11-31% patients with SAB have endocarditis). i. All patients should have a thorough history taken and exam performed with any new complaint evaluated for possible metastatic infection. ii. Echocardiograms should be strongly considered for all patients with SAB iii. All patients with a prosthetic valve, pacemaker/ICD present, or persistent bacteremia (follow up blood cultures positive) should undergo a transesophageal echocardiogram 3. -

Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S
Antimicrobial Activity of Ceftaroline Combined with Avibactam Tested Against Contemporary (2012) Helio S. Sader, MD, PhD JMI Laboratories Bacteria Collected from USA Patients with Acute Bacterial Skin and Skin Structure Infections (ABSSSIs) North Liberty, IA, USA ECCMID 2013 www.jmilabs.com HS SADER, RK FLAMM, RN JONES ph. 319.665.3370 P1620 fax 319.665.3371 JMI Laboratories, North Liberty, Iowa, USA [email protected] Table 2. Antimicrobial activities of ceftaroline-avibactam, ceftaroline and comparator agents when tested against gram-negative organisms from Abstract Introduction Results skin and skin structure infections (USA, 2012). Conclusions Objective: To evaluate the activity of ceftaroline Ceftaroline, the active metabolite of the prodrug ceftaroline • The most common organisms were S. aureus (3,481; Organism (no tested)/ MIC (mg/L) %S / %I / %R • Ceftaroline-avibactam was highly active antimicrobial agent 50% 90% Range CLSIa EUCASTa (CPT)-avibactam (AVI) tested against bacteria from fosamil, is a cephalosporin with notable in vitro bactericidal 50.5% MRSA), E. coli (444; 13.3% ESBL-phenotype), β- E. coli (444) against ESBL-phenotype and carbapenem- ABSSSI collected in USA hospitals in 2012. CPT activity against organisms commonly responsible for haemolytic streptococci (βHS; 389) and Klebsiella spp. Ceftaroline-avibactam 0.03 0.06 ≤0.015 – 0.5 - / - / - - / - / - non-susceptible Enterobacteriaceae Ceftaroline 0.12 32 ≤0.015 – >32 83.3 / 2.7 / 14.0 83.3 / 0.0 / 16.7 fosamil is a novel parenteral cephalosporin community-acquired -

Cephalosporins Can Be Prescribed Safely for Penicillin-Allergic Patients ▲
JFP_0206_AE_Pichichero.Final 1/23/06 1:26 PM Page 106 APPLIED EVIDENCE New research findings that are changing clinical practice Michael E. Pichichero, MD University of Rochester Cephalosporins can be Medical Center, Rochester, NY prescribed safely for penicillin-allergic patients Practice recommendations an allergic reaction to cephalosporins, ■ The widely quoted cross-allergy risk compared with the incidence of a primary of 10% between penicillin and (and unrelated) cephalosporin allergy. cephalosporins is a myth (A). Most people produce IgG and IgM antibodies in response to exposure to ■ Cephalothin, cephalexin, cefadroxil, penicillin1 that may cross-react with and cefazolin confer an increased risk cephalosporin antigens.2 The presence of of allergic reaction among patients these antibodies does not predict allergic, with penicillin allergy (B). IgE cross-sensitivity to a cephalosporin. ■ Cefprozil, cefuroxime, cefpodoxime, Even penicillin skin testing is generally not ceftazidime, and ceftriaxone do not predictive of cephalosporin allergy.3 increase risk of an allergic reaction (B). Reliably predicting cross-reactivity ndoubtedly you have patients who A comprehensive review of the evidence say they are allergic to penicillin shows that the attributable risk of a cross- U but have difficulty recalling details reactive allergic reaction varies and is of the reactions they experienced. To be strongest when the chemical side chain of safe, we often label these patients as peni- the specific cephalosporin is similar to that cillin-allergic without further questioning of penicillin or amoxicillin. and withhold not only penicillins but Administration of cephalothin, cepha- cephalosporins due to concerns about lexin, cefadroxil, and cefazolin in penicillin- potential cross-reactivity and resultant IgE- allergic patients is associated with a mediated, type I reactions. -

Estimation and Use of Serum Levels in the Evaluation of the New Penicillins J
Postgrad Med J: first published as 10.1136/pgmj.40.Suppl.17 on 1 December 1964. Downloaded from 17 demonstrate a chemotherapeutic effect of a extremely difficult to show clinically that one compound that has a reasonable degree of effective antibiotic is in fact better than another activity against a certain pathogen, particularly effective antibiotic and if comparison is to be if the dosage used in the trial is high enough made, very large numbers of patients are to provide adequate free antibiotic levels in required for it is not possible to carry out a serum and tissues. Unfortunately, with so comparitive trial at threshold dosages when many new antibiotics at our disposal, it is treating active human infections. ESTIMATION AND USE OF SERUM LEVELS IN THE EVALUATION OF THE NEW PENICILLINS J. M. BOND National Institute for Medical Research, Mill Hill, London, N.W.7. PENICILLINS are reversibly bound to serum membrane, and secondly no that there was Protected by copyright. albumin, and in their bound form are bio- differential filtration of the antibiotic itself, logically inactive, although the activity is not as occurred with certain other similar destroyed and can be recovered by dissociation techniques. of the antibiotic/protein complex. Whatever When comparing penicillins, two sources of its therapeutic significance, this binding of variation in serum binding have to be con- penicillins is important when assaying serum sidered. Firstly there is the well-known varia- levels, especially when these results are to be tion in percentage binding between different used to compare by laboratory tests the possible penicillins to the same medium.